
Abstract
Background
Acoustic radiation force impulse (ARFI) elastography has been used to assess liver stiffness non-invasively. However, its usefulness in alpha-1 antitripsin-deficient (AATD) individuals is unknown.
Purpose
To assess if liver fibrosis is present in a cohort of AATD individuals using ARFI elastography.
Material and Methods
Eighty-three participants aged 38–39 years, except for two who were aged 40 years, underwent ultrasound elastography of the liver with ARFI technique. Twenty-nine were homozygote ZZ genotype, PiZZ (14 men, 15 women); 12 were SZ genotype, Pi SZ (8 men, 4 women), and 42 were healthy volunteers, PiMM (16 men, 26 women). Three specific liver anatomical regions were examined: segments 2/3 (left lobe) in the subcostal plane, and 5/6 and 7/8 (right lobe) in the intercostal space. In each region, three measurements were registered.
Results
There was no statistically significant difference between ARFI-median in the AATD group and the control group (P value = 0.877) and neither between AATD groups (PiZZ and PiSZ) with a P value = 0.259. The ARFI-median was lower in the right liver lobe than in the left lobe in all groups and the difference between both lobes was statistically significant (P = 0.001). No statistically significant difference was found in ARFI-median of the right liver lobe between the AATD group and the control group (P = 0.759), nor between the AATD group (P = 0.384). No gender difference was found in ARFI-median.
Conclusions
ARFI values in AATD individuals aged 38–39 years showed no difference compare to healthy participants.
Keywords
Introduction
Chronic liver diseases have been extensively studied and examined using different techniques because they represent an important public health issue. The prognosis of chronic liver disease depends on the progression of liver fibrosis. A crucial aspect is to establish the stage of fibrosis with the goal of establishing possible therapeutic strategies and prognosis. Research has been focused on the most common causes of development of liver fibrosis such as Hepatitis C and B and alcohol consumption. But, there are other systemic diseases like alpha-1-antitrypsin deficiency (AATD) that also develops fibrosis and cirrhosis in its late stage.
AATD is a common cause of chronic liver disease, mainly in those homozygotes phenotype ZZ. In this population, the estimated risk for development of liver cirrhosis and/or liver cancer in late adulthood is about 25% (1). Thus, the American Society of Respiratory Medicine and The European Respiratory Society recommend testing for AATD in all individuals “with unexplained liver disease, including neonates, children, and adults, especially the elderly” (2,3).
Many efforts have been made to develop non-invasive diagnostic tools for detection of liver fibrosis including the need for grading its stage in order to reduce liver biopsies. Ultrasound is the most commonly used and studied non-invasive diagnostic modality thus far, and elastography, its principal technique to measure liver stiffness. The principal approach of elastography is the measurement of tissue elasticity, in other words, quantifying the mechanic deformation when a mechanical force is applied on a tissue.
There are different ultrasound elastographic methods. They have recently been well described by Sporea (4) and Frulio (5). The most studied are those that use shear wave techniques: transient elastography TE (best known as FibroScan®), Acoustic Radiation Force Impulse ARFI quantification (Siemens, Philips) and Real-Time Shear Wave Elastography (Supersonic Imagine, Aixplorer system).
In the early 2000s, Nightingale et al. (6) described the acoustic radiation force as “a phenomenon associated with the propagation of acoustic waves in attenuating media.” It was the beginning of what the technique can offer now. The ARFI technique has been developed by Siemens on Acuson S2000 and S3000 devices (Issaquah, WA, USA), and by Philips on the iU22 device (Bothell, WA, USA).
The principles of the ARFI technique are based on the following three steps. The first step is to obtain a baseline B-mode image of reference by conventional ultrasound of the region of interest (ROI). The second step is to transmit an acoustic “push” impulse through the tissue in the ROI that will experience a small displacing mechanical force. Once the push pulse has passed through, the tissue begins to relax towards its original configuration. The third step is to apply conventional sonographic tracking beams during a short time interval (ms) that will provide data that are compared with the reference image for computing tissue displacements resulting from the push pulse. Those wave displacements occur on a certain velocity and ARFI technology with Virtual Touch Tissue Quantification® software measures the value of shear wave speed. The time between the generation of the shear wave and detection of the peak is utilized to compute the shear wave velocity at that point (p-SWV). The results are expressed in meters per second (m/s). The more stiff a region of tissue, the greater a shear wave’s speed as it travels through this region. The measurement of the shear wave velocity is made for a selected ROI which is determined by the examiner. This ROI has standard dimensions of 1 × 0.6 cm and can be placed at a maximum depth of 8 cm.
The aim of the study was to measure liver elasticity in a cohort of AATD individuals aged 38–39 years compared to healthy volunteers using p-SWV with ARFI technique in order to detect liver fibrosis, if it were to be present.
Material and Methods
Participants
The study was approved by the local ethics committee and written informed consent was obtained by each participant for the investigations.
All the participants were born between 1972 and 1974. The individuals with AATD belong to the national register for alpha-1-antitripsin deficiency. Eighty-three participants aged 38–39 years, with the exception of two who were aged 40 years, underwent ultrasound elastography of the liver with the ARFI technique. Twenty-nine were homozygote ZZ genotype, PiZZ (14 men, 15 women); 12 were SZ genotype, Pi SZ (8 men, 4 women), and 42 were healthy volunteers, PiMM (16 men, 26 women). The AATD participants are controlled periodically at the local department of the Respiratory Medicine and Allergology with biochemical tests which include ALT, AST, GGT, ALP bilirubin, PIII-NP, INR, albumin, and platelets between others, in order to assess if they have any signs of liver alteration.
Liver examination
Each individual was examined with an Acuson S2000 ultrasound system (SIEMENS, Erlanger, Germany), using a 4C1 MHz curved array probe with acoustic radiation force impulse (ARFI) technology, using the Virtual Touch technology for tissue stiffness quantification developed by Siemens for measurement of the point shear wave velocity (p-SWV – m/s) in tissue. ARFI elastography was performed with the participant lying in the dorsal decubitus position with the right arm elevated above the head and was asked to stop breathing for a moment without deep inspiration, in order to minimize invalid SWV measurements due to breathing motion. The individuals were fasting for at least 3 h before the examination.
Each participant was examined in three specific liver anatomical regions: segments 2/3 (left lobe) in the subcostal plane, and 5/6 and 7/8 (right lobe) in the intercostal space, in accordance with the segmental anatomical classification of Couinaud (7), which is accepted as standard. At each region, three measurements were registered. The ROI location varied to the best fit in order to avoid vascular and biliary structures from register.
Examinations were performed by two experienced radiologists (OE and SD) who were blinded to the group of the patient.
The mean and median values were calculated at each location. Body mass index (BMI) and gender were included in the analysis as influence factors.
Data were analyzed using XLStat 2015 for Windows. Pearson correlation, independent Student’s t-test, and multiple linear regression were applied where appropriate.
Results
None of the participants included in this study showed alterations that could indicate liver disease in the tests performed at the local department of Respiratory Medicine and Allergology. The results of clinical assessment of liver function are not presented here because they have recently been extensively reported and published by the group of clinicians that contributed with the individuals for this study (8) and therefore lies beyond the scope of this article.
Demographic data of 83 individuals included in the analysis. The results are given for each individual group.

BMI, body mass index; SD, standard deviation; Pi, protein inhibitor.
Median, mean, and depth for each liver lobe and participant group.

SWV, shear wave velocity; m/s, meter per second; SD, standard deviation; Pi, protein inhibitor.
The mean values of SWV were higher in all groups in comparison to the median values. Mean and median values of SWVs of the left lobe were higher than the right lobe as other publications have shown. The median of SWV was lower in the right liver lobe than in the left lobe in all groups and the difference between both lobes were statistically significant (P = 0.001).
There was no statistically significant difference in the median of SWVs between men and women in the whole group (P = 0.238).
There was no statistically significant difference between the median of SWVs in the AATD group and the control group (P value = 0.877) and neither between the AATD groups (PiZZ and PiSZ) with a P value = 0.259.
There was no statistical difference in the median of SWV measurements of the right liver lobe between the AATD group and the control group (P = 0.759), nor between the AATD groups (P = 0.384).
Fig. 1 shows the median of SWV measurements of the right lobe in each group by gender.
P-SWV measurements across subjects by gender.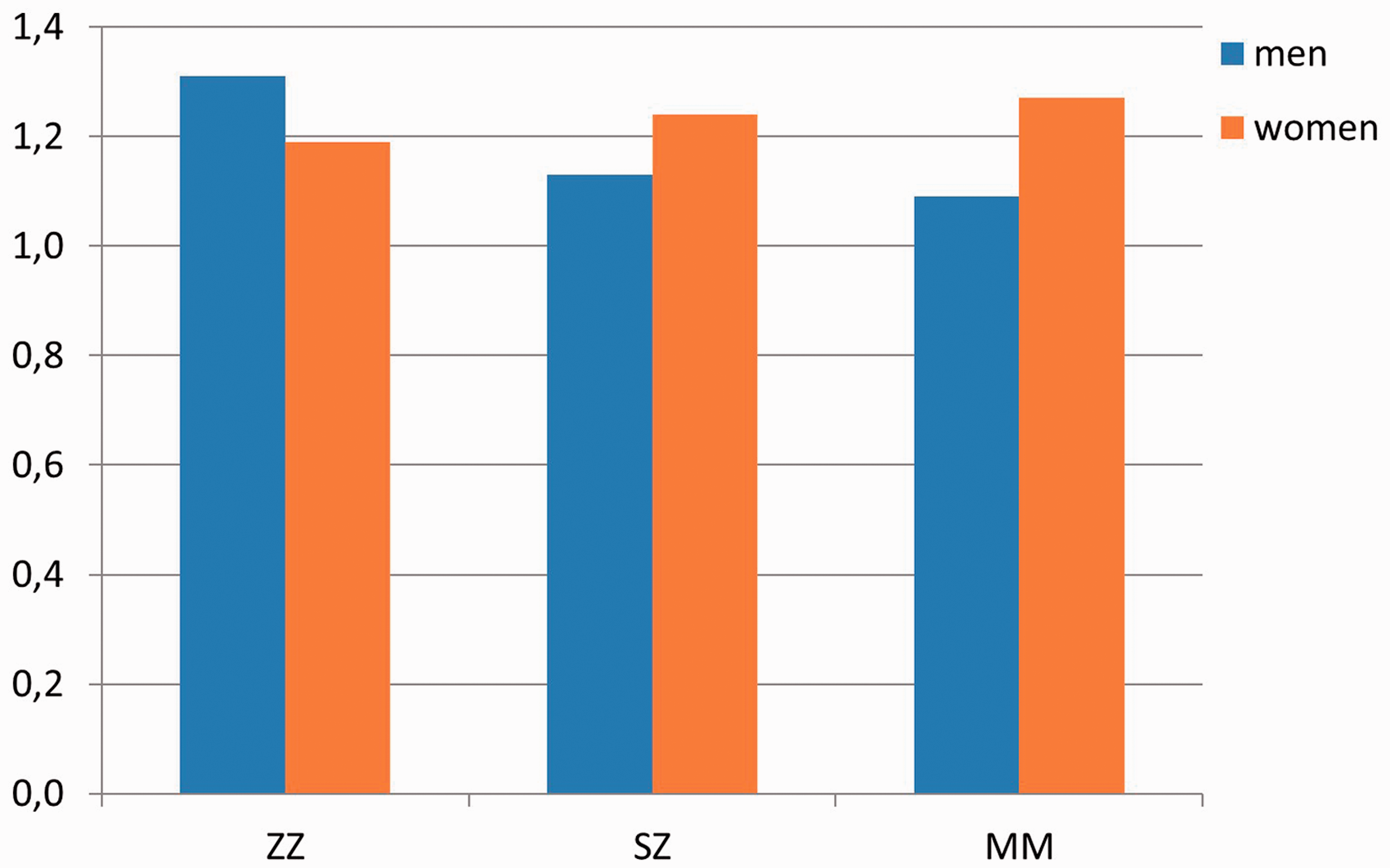
The mean depth in all groups was 5.22 ± 0.59 cm (range = 3.2–7 cm). The depth was correlated with SWV measurements (P = 0.026).
Discussion
Globally, our results are comparable with other published articles (9–12) for healthy volunteers in the range of 0.97–1.56 m/s. We found increased ARFI values in the left liver lobe as many other authors have demonstrated. Those results are not included in the analysis. A histological correlation with ARFI was not possible to carry out due to the ethical implications of performing biopsies in asymptomatic and/or individuals with normal liver function tests as well as in healthy participants.
We tried to compare our SWVs results with cut-off values (m/s) for predicting the stages of fibrosis described by Lupsor et al. (13) (F ≥ 1: 1.19; F ≥ 2: 1.34; F ≥ 3: 1.61; and F ≥ 4: 2.00) and Sporea et al. (14) based on Metavir staging system (F ≥ 1: 1.19; F ≥ 2: 1.21; F ≥ 3: 1.58; and F ≥ 4: 1.82) in the assumption that healthy participants belong to the F0 stage (no known history of liver disease with normal liver function test). When comparing with both cut-off systems, our group of PiZZ participants, with a median of SWV of 1.38 ± 0.36 m/s, should belong to stage F ≥ 2. According to the pooled meta-analysis by Friedrich-Rust et al. (15) (cut-off values F ≥ 2: 1.34; F ≥ 3: 1.55; and F ≥ 4: 1.80), F ≥ 2 is defined as significant fibrosis, F ≥ 3 as severe fibrosis, and F ≥ cirrhosis. This was a worrisome finding for us due to the negative results of biochemical tests and clinical status. The prospective study of Wan et al. (16) showed that SWV measurement with ARFI technique correlates best with fibrosis grades and inflammatory stages 3 and above and may not be as useful in fibrosis stages 2 or lower, when those proposed cut-off values are used. This study could possibly explain our slightly higher results in the PiZZ group.
It is very difficult to interpret our results for clinical implementation based on the results and interpretations that the different authors give to their findings.
There are some limitations in our study. Our study was planned and performed before the definitive guidelines and recommendations from the World Federation for Ultrasound in Medicine & Biology (WFUMB) first came out in 2015 (17,18) after previous guidelines from the European Federation of Societies for Ultrasound in Medicine & Biology (EFSUMB) 2013 (19,20). The optimal conditions pointed out in the latest recommendations were not completely fulfilled. Fasting was not as long as 4–8 h as reported before. The examinations were in the afternoon due to geographical reasons (participants from the whole country were recruited) and the CT scan was not available. The ROI placement at 1.5–2.0 cm beneath Glissons’s capsule was at the limit in three very thin individuals, all of them in the control group. At least ten valid measurements from the right liver lobe are required. We made a total of six. Confounding factors such as liver inflammation, obstructive cholestasis, liver congestion, acute hepatitis, and infiltrative liver disease that can give overestimation of liver fibrosis were assumed as not present, due to the asymptomatic status of the participants.
The factors mentioned above could influence our slightly higher results, especially in the PiZZ cohort, that consequently cause them to be classified in the group of significant fibrosis although they did not present any clinical or biochemical signs of alteration.
It is known that individuals with severe AATD have the potential to develop liver fibrosis as well as lung emphysema. The probability to find altered values in a relatively young population with this protein deficiency was very low but nevertheless unknown. What is not known yet is when, along the course of sickness, they will develop liver fibrosis.
In a recently published study (21), ARFI elastography using SWV measurement showed robustness with similar results reported by other groups with other elastography techniques. Elastography as ultrasound technique is not so wide spread in Scandinavia as is in the rest of Europe and the world. Very little is known of its use in the clinical praxis in hospitals. To our knowledge this is the first study to try to assess liver fibrosis in an asymptomatic cohort of individuals with AATD. We have tried with this retrospective analysis to establish a starting point in the follow-up of liver status in patients with AATD using ultrasound elastography. This cohort has been followed each fourth year with biochemical blood samples, spirometric measurements, and since the age of 30 years with low dose computed tomography of the chest. There is a special interest in the early diagnosis of the disease in order to prevent all the possible alterations that the protein deficiency carries on. This cohort will be followed in the next decade with the same battery of tests including imaging. It is expected that in their late 40s, the change in lifestyle and the age itself can influence their liver status. At that point, it would be interesting to evaluate the liver again with ultrasound elastography and compare this with the actual results without excluding other non-invasive imaging alternatives such as magnetic resonance elastography that shows promise in the detection of liver fibrosis as has been published recently by Kim et al. (22).
In conclusion, we have demonstrated that the median of SWV measurements by the ARFI technique in participants with AATD compared to controls at aged 38–39 years were in the interval of what has been reported for healthy individuals. Evidence of liver fibrosis based on the SWV results in the cohort of PiZZ could not be excluded in light of the actual literature.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.