
Abstract
Background
Peritoneovenous shunts (PVS) are widely used for palliation of intractable ascites caused by peritoneal carcinomatosis (PC) or liver cirrhosis (LC). Some patients who need PVS have renal dysfunction. However, renal dysfunction is considered a relative contraindication. Therefore, it is important to assess renal function before PVS placement.
Purpose
To evaluate the relationship between PVS and renal function.
Material and Methods
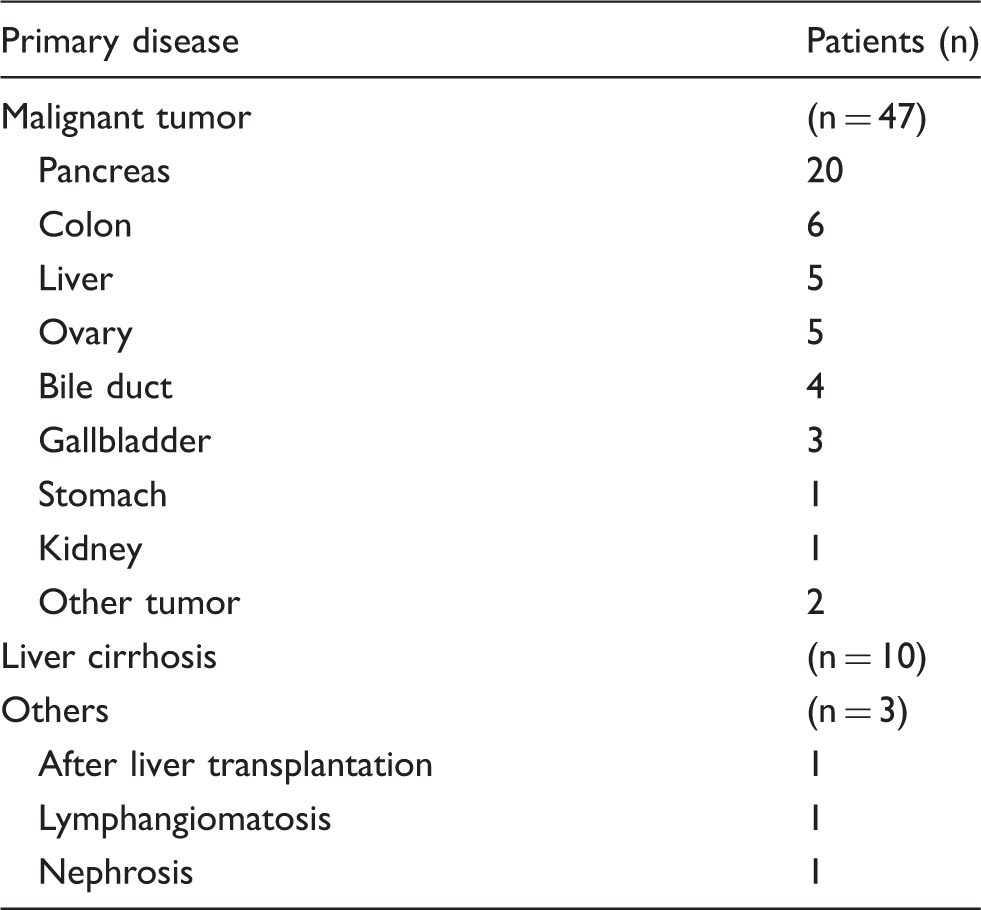
Between October 2007 and July 2015, 60 patients (PC = 47; LC = 10; others = 3) underwent PVS placement for intractable ascites. Changes in estimated glomerular filtration rate (eGFR) and other adverse events (AEs) were retrospectively analyzed.
Results
Changes in eGFR before, one day after, and one week after PVS placement could be evaluated in 46 patients. The median eGFR before, one day after, and one week after was 56.5, 59.1, and 64.7 mL/min/1.73 m2, respectively (P < 0.05). These values were 61.6, 72, and 67.1 mL/min/1.73 m2, respectively, in PC patients (n = 34; P < 0.05) and 28.5, 27, and 37.2 mL/min/1.73 m2, respectively, in LC patients (n = 10; P < 0.05). In 17 patients with moderate to severe renal dysfunction (eGFR < 45), these values were 23.4, 23.7, and 30.5 mL/min/1.73 m2, respectively. The most frequent AE was PVS catheter obstruction, which occurred in 12 patients (20.7%). Clinical disseminated intravascular coagulation occurred in six patients (10.3%) and caused death in three patients (5.2%).
Conclusion
PVS placement for intractable ascites is associated with various AEs. However, PVS appeared to promote renal function, especially in patients with renal impairment.
Introduction
Patients who have liver cirrhosis (LC) and peritoneal carcinomatosis (PC) may develop intractable ascites (1,2). Aspiration of ascitic fluid may provide temporary relief. However, paracentesis must be repeated frequently and results in the loss of endogenous circulating proteins (3). Diuretic therapy is also commonly ineffective and results in a reduction in circulating blood volume (3). This non-response of ascites to medical treatment causes pain, anorexia, dyspnea, reduced mobility, and poor quality of life (QOL). Peritoneovenous shunt (PVS) is an effective method for palliation of intractable ascites caused by PC or LC (2,4–7). Renal dysfunction is considered to be a relative contraindication for PVS because a rapidly increased overload volume is intolerable and might cause severe complications (8). However, some patients who need PVS have renal dysfunction. Therefore, assessing renal function is important before PVS placement and the dilemma exists regarding whether to implant PVS or not in patients with renal dysfunction. The purpose of this study was to evaluate the influence of PVS implantation on renal function.
Material and Methods
Patients
This retrospective study included consecutive patients who underwent PVS implantation in our hospital, between October 2007 and July 2015, for intractable ascites mainly due to LC or PC. Intractable ascites was defined as follows: (i) ascites that could not be managed by repeated abdominal paracentesis and/or diuretic therapy; or (ii) ascites that induced deterioration in QOL. The indications for PVS implantation were: (i) intractable ascites; (ii) absence of severe heart failure; and (iii) ascites without infection or mucinous component. Written informed consent was obtained from each patient before PVS implantation. Our institutional review board approved this retrospective study.
PVS
We used a PVS kit (Denver-PAK; Denver Biomaterials, Inc., Golden, CO, USA) in all patients. PVS procedures were divided into a one-step and two-step placement. In the one-step placement, conventional PVS procedures were performed percutaneously under ultrasonographic guidance and fluoroscopy using an interventional radiological technique (4–6). As a rule, catecholamine was used to support cardiac function and diuresis 1–3 days postoperatively. Gabexate mesilate was also used to prevent disseminated intravascular coagulopathy (DIC) on these days. In the two-step placement, a trial infusion was applied in patients for whom conventional PVS was considered inappropriate because of coagulation disorders, advanced renal failure, or poor performance status (9). As two-step placements, we used an externalized PVS method reported by Tokue et al. (9) or a manual ascitic return method by connecting a central venous catheter and an abdominal drainage catheter. In the manual ascitic return method, we manually returned about 1500 mL of ascites into the vein per day to evaluate side effects. After evaluating the temporal PVS response, conventional PVS implantations were applied in these patients.
Clinical outcome measures
Technical success, clinical efficacy, adverse events (AEs), and renal function parameters related to PVS placements were retrospectively reviewed and collected from medical records. In the case of a patient who underwent repeated PVS placement, only the first PVS placement was included in the analysis. Serious adverse events (SAEs) were defined as medical occurrences related to the procedure that were life-threatening or required additional intervention or surgery. Estimated glomerular filtration rate (eGFR) was used for evaluating renal function parameters. Based on the eGFR values (mL/min/1.73 m2), renal dysfunction was classified as follows: severe dysfunction (eGFR < 30), moderate dysfunction (30 ≤ eGFR < 45), mild dysfunction (45 ≤ eGFR < 60), and normal function (60 ≤ eGFR). Since the calculation of eGFR could not be adapted for patients aged < 18 years, they were excluded from the analysis of renal function. eGFR data before PVS placement, one day after PVS placement, and one week after PVS placement were collected. Pre- and postoperative eGFR were compared using the Wilcoxon signed rank test. All statistical analyses were performed using Statcel4 (Nebula Company, Bunkyo-ku, Tokyo, Japan). P values < 0.05 were considered statistically significant.
Results
Patient characteristics
Clinical characteristics of patients.

Primary disease details.

Process of PVS placement. We attempted two-step placement in patients with a poor general condition and renal function. One patient could not undergo conventional PVS placement because he had a fever and continued shivering after trial infusion. PVS, peritoneovenous shunt.
Technical and clinical outcomes and complications
Of the 59 patients (PC = 46 patients, LC = 10 patients, others = 3 patients) who underwent conventional PVS placements, technical success was achieved in 58 (98.3%). Technical failure occurred in one patient with PC who underwent abdominal paracentesis just before the PVS procedure, and the insertion of an abdominal catheter was technically impossible. Additional PVS placement was not performed because the patient declined. After PVS placement in 58 patients, immediate palliation of abdominal distention was achieved in 49 patients (84.5%). Among the 45 PC patients in whom PVS was successfully implanted, 32 died 1–267 days after the procedure (median = 36 days). The other 13 PC patients were lost to follow-up since they were at a terminal stage and were transferred to other palliative care hospitals. Among the ten LC patients, seven died 14–695 days after PVS (median = 299 days), two survived (627 days and 805 days, respectively), and one was lost to follow-up.
Adverse events (AEs) in peritoneal carcinomatosis (PC), liver cirrhosis (LC), and others.

Values are n (%).
DIC, disseminated intravascular coagulation.
Relationship between PVS and renal function
The changes in eGFR before, one day after, and one week after PVS placement could be evaluated in 46 patients. The median eGFR values before, one day after, and one week after were 56.5, 59.1, and 64.7 mL/min/1.73 m2, respectively (P < 0.05) (Fig. 2). In PC patients (n = 34) these values were 61.6, 72, and 67.1 mL/min/1.73 m2, respectively (P < 0.05); in LC patients (n = 10) 28.5, 27, and 37.2 mL/min/1.73 m2, respectively (P < 0.05) (Fig. 3). The 46 patients were also divided into three renal function groups: severe dysfunction (n = 11), moderate dysfunction (n = 6), and normal to mild dysfunction (n = 29). In these three groups, eGFR values tended to be higher after PVS placement (Fig. 4). In particular, in 17 patients with moderate to severe renal dysfunction (eGFR < 45), eGFR was 23.4, 23.7, and 30.5 mL/min/1.73 m2, respectively, and the renal function one week after PVS was significantly improved (P < 0.05).
Relationship between PVS and renal function. The median eGFR values in 46 patients before, one day after, and one week after were 56.5, 59.1, and 64.7 mL/min/1.73 m2, respectively. The renal function post-PVS was significantly improved (P < 0.05). PVS, peritoneovenous shunt. Renal function comparison between PC and LC. PC, peritoneal carcinomatosis; LC, liver cirrhosis. Changes of eGFR among three renal function groups. The renal function tended to be improved one week after PVS placement. (a) Severe renal dysfunction (11 patients); (b) moderate renal dysfunction (6 patients); (c) normal to mild renal dysfunction (29 patients). PVS, peritoneovenous shunt.


Discussion
Medically intractable ascites due to LC or PC causes significant morbidity. The PVS (Denver shunt) is currently used to treat both cirrhotic and malignant ascites (2,7,10). Transjugular intrahepatic portosystemic shunt (TIPS) is another treatment option for persons with cirrhotic ascites (11). TIPS can theoretically reduce portal venous pressure and decrease ascites formation. However, an increased frequency and severity of hepatic encephalopathy and liver failure are also associated with TIPS (7). Therefore, we performed PVS for intractable cirrhotic ascites. The clinical effectiveness rate of PVS in our study was 84.5% and was comparable with previous reports (8,10). Despite the considerable clinical effectiveness of PVS, it is associated with several complications, including DIC, pulmonary edema, pulmonary embolism, and infection. Sugawara et al. (8) reported in their retrospective analysis of 133 patients that abnormalities in coagulation without clinical symptoms (subclinical DIC) after PVS placement was 27.8%; clinical DIC occurred in 5.3%. Therefore, PVS cannot be performed without risks and careful patient selection is recommended (2,10). Moreover, the prediction of clinical DIC before PVS placement is impossible; we experienced clinical DIC in six cases (10%) in our study and death occurred in three of these cases within one week after PVS placement. Thus, DIC may be caused by the introduction of procoagulants into the systemic circulation (12,13). Trial infusion seems useful in some patients for assessing patient tolerance for subsequent PVS placement (9).
Since PVS is associated with overloaded volume that might cause death, renal failure is one of the relative contraindications for PVS (10). Bieligk et al. also reported that preoperative impaired renal function was a predictive factor of poor prognosis after PVS insertion (3). Therefore, careful assessment of renal function is important before PVS placement. However, some patients who need PVS tend to have associated renal dysfunction. In this study, we evaluated the influence on renal function of PVS using eGFR. The eGFR values one week after PVS placement were significantly higher than those before PVS placement in both the PC and LC groups. In patients with moderate to severe renal dysfunction, in particular, eGFR values were also improved after PVS placement. From our results, increased circulating blood volume due to PVS may induce effective renal blood flow and diuretic effect. Similar results are reported in cirrhotic patients with intractable ascites where GFR significantly improved after PVS placement during the waiting period before liver transplantation (14). Seike et al. also reported that creatinine decreased five days after PVS placement in PC patients (15). To our knowledge, this is the first report where the relationship between renal function and PVS was evaluated using eGFR. Since patients with intractable ascites of LC or PC often develop reversible renal dysfunction, early PVS placement might improve renal function and prevent irreversible renal failure.
The main limitations of this study must be acknowledged. This was a retrospective analysis of patients who underwent PVS at a single institution and the study had a small sample size. Patients with severe renal impairment might be excluded from PVS procedures and complications related to renal failure were presumably avoided.
In conclusion, PVS placement for intractable ascites appeared to promote renal function, especially in patients with moderate to severe renal impairment. However, PVS placement was associated with various AEs. Prudent preoperative evaluation and postprocedural monitoring are necessary to preclude SAEs after PVS.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.