
Abstract
Background
Congenital abnormalities of the gastrointestinal tract are increasingly being evaluated by prenatal magnetic resonance imaging (MRI). However, there is a paucity of reports describing the normal quantitative development of the fetal colon and rectum on MRI.
Purpose
To provide growth curves of the MRI estimated diameter of the fetal colon and rectum as a function of gestational age.
Material and Methods
This is a retrospective review of 191 singleton fetal MRI studies at 25–39 weeks of gestation. Measurements included maximal diameter of the ascending, transverse, and descending colon on coronal and sagittal views, maximal diameter of the rectum on coronal and sagittal views, and maximal diameter of the rectum at the level of the bladder base on sagittal views. Median growth curves were built using a generalized additive model. Confidence regions were built for 10th, 25th, 75th, and 90th percentiles.
Results
Smoothed growth curves for the median, and one and three quartiles for each of the five sections as a function of gestational age were calculated. All graphs had a slightly exponential curve.
Conclusion
This study provides normal ranges of the prenatal colon and rectum as a function of gestational age. They may serve as reference values when interpreting fetal MRI.
Introduction
The overall incidence of congenital gastrointestinal (GI) anomalies is in the range of 1–15 per 10,000 live births. Many congenital GI anomalies result in intestinal obstruction and may affect the caliber of different segments of the GI tract. On prenatal imaging, abnormally small or dilated colon and rectum often provide a clue to diagnosis.
Malformations potentially affecting the large bowel caliber include anorectal atresia, low intestinal atresia, small left colon syndrome, meconium ileus, megacystis-microcolon-intestinal hypoperistalsis, and Hirshprong’s disease.
Although prenatal magnetic resonance imaging (MRI) is becoming more common, there are few data regarding the size of the colon and rectum and their growth throughout gestation. In addition, it is not known whether ultrasound (US)-derived curves of fetal colon diameters can be used when interpreting MRI studies.
Reference values can be of assistance to differentiate normal from pathological findings, especially in equivocal cases, and thus contribute to the overall prenatal management.
The aim of this study is twofold: first, to provide normal ranges of the prenatal colon and rectum as a function of gestational age for fetuses aged 25–37 weeks; and second, to compare them with normal US-derived values.
Material and Methods
The hospital’s institutional review board approved this retrospective study.
The reports of all fetal body MRI examinations performed during 2005–2014 in our institution were retrieved from the hospital’s electronic files. Indications for the exams were reviewed; multiple pregnancies and patients referred for fetal GI disorders or related abnormalities such as poly or oligohydramnion were excluded.
MRI studies were performed after premedication with oral Diazepam 5 mg on a 1.5-T unit (Signa HDxt 1.5T or Optima MR360, GE Healthcare, Milwaukee, WI, USA) with the patient in the supine or left lateral decubitus position. Sequences included T2-weighted (T2W) single shot fast spin echo, T2W fast spin echo, and T1-weighted (T1W) fast spoiled gradient-recalled echo.
MRI images were reviewed by pediatric radiologists (all authors) blinded to gestational age and original interpretation in joint sessions in consension by two radiologists or by a single pediatric radiologist. The colon and rectum were identified on T1W images due to the bright signal of meconium. The caliber of the colon and rectum were measured for each MRI study on T1W images at nine different segments: ascending, transverse, and descending colon in both sagittal and coronal views; and rectum in sagittal and coronal views and rectum in sagittal view at the level of the bladder base. With the exception of the rectum at the level of the bladder base, all measurements were done where the colon was both widest and clearly depicted. Measurements were taken by placing electronic calipers on the outside border of the meconium. Examples of measurements are shown in Fig. 1.
Examples of measurements: (a) left colon; (b) right colon; and (c) sagittal view of rectum with measurements at bladder base (arrow) and maximal rectal diameter (arrowhead). B, bladder.
In order to preserve unity, a segment of the colon or rectum was deemed inadequate for measurement if it was not in a true sagittal or coronal plane or if its border was blurred due to fetal movement. An MRI examination had to have at least one adequate measurement to be included in the analysis.
MRI image quality was assessed according to the distinctness of the colonic borders on T1W series and graded into three groups: group 1 = all colonic segments had well-defined borders and were measurable on both the sagittal and coronal planes; group 2 = only some of the colonic segments were measurable; and group 3 = motion and other artefacts rendered all colonic segments unmeasurable or the whole abdomen was not included in the T1 series.
As there was only one study each for the gestational ages of 19, 22, and 23 weeks, these measurements were excluded from the final statistical analysis.
Statistical analysis
The smoothed growth curves were built using a generalized additive model as it was realized in the R package gamlss. The curves were plotted for the 10th, 25th, 50th (median), 75th, and 90th percentiles. Inter-observer and intra-observer variance were calculated using the intraclass correlation coefficient (ICC) and Landis and Koch’s Benchmark scale. A P value < 0.05 was considered statistically significant. All calculations and plots were obtained using R 3.3.1. Comparisons with US, that were published by Zalel et al. (1), were done using two-way ANOVA for grouped data as it was implemented in the ind.twoway.second function of R package rpsychi. We used Benjamini–Hochberg false discovery rate (FDR) correction for multiple comparisons when comparing the five growth curves with the corresponding results of Zalel et al. (1,2).
Results
Reasons for referral to fetal body MRI.

Number (%) of adequate measurements per segment/view.


Growth curve of the left colon: (a) sagittal view and (b) coronal view.
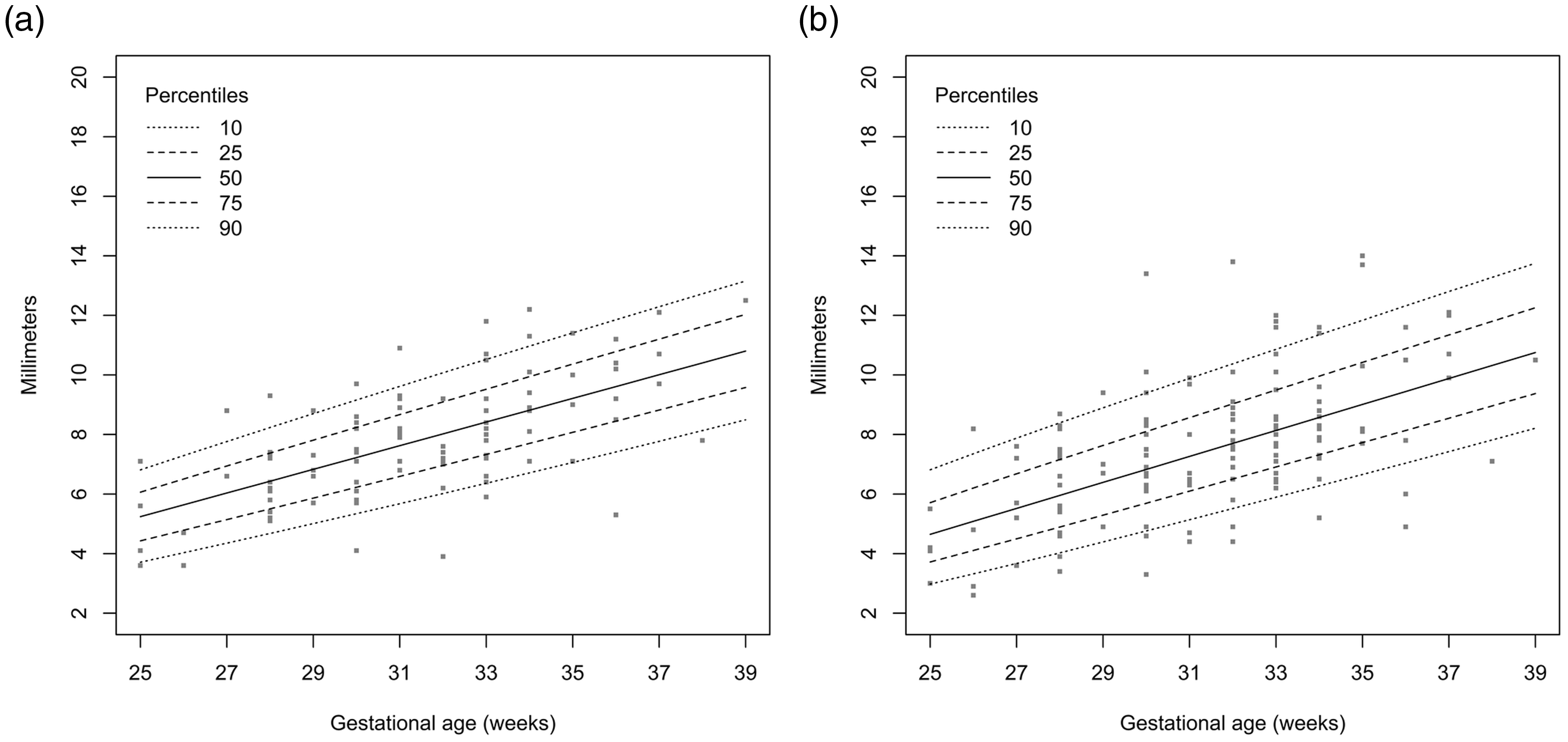
Growth curve of the right colon (a) sagittal view and (b) coronal view.

Growth curve of the transverse colon: (a) sagittal view and (b) coronal view.

Growth curve of the rectum in the sagittal plane.

Growth curve of the rectum in the sagittal plane at the level of bladder base.

Growth curve of the rectum in the coronal plane.
Number of segments measured per gestational age.

Difference between US measurements and MRI measurements.

Discussion
Recent years have shown a growth in the use of MRI for the evaluation of pregnancies. Although US remains the mainstay for the diagnosis of most fetal abnormalities, at our institution MRI is often called upon for auxiliary analysis or for confirmation of equivocal findings anomalies, including suspected bowel obstruction. Moreover, some studies have even shown MRI’s superiority for certain bowel obstructions (3). Therefore, the purpose of this study was to create standard normal values with growth curves to which suspected pathology can be compared.
The fetal colon and rectum are easily identified by the presence of meconium bright on T1W sequences as early as 13 weeks of gestational age and until term (4). After 20 weeks, there is functional obstruction of the anal canal due to high pressure in the anal sphincter. As a result, meconium, rich in epithelial cells, bile, and mucous, accumulates and eventually fills the entire large bowel. The bright signal on T1W images is due to the high concentration of fatty acids, amino acids, organic acids, sterols, and ketone bodies (5).
Numerical reference values are available for the MRI appearance of fetal lungs, kidneys, central nervous system, and eyes (6–13). However, in our search of the literature we found only one study with diameter measurements of the normal large bowel and rectum on MRI (4). This study included only 40 normal fetuses without quartile. In their study of 379 healthy pregnancies, Zalel at al. (1) published growth curves of the normal fetal large bowel by US. Due to inherent differences between the modalities, one cannot be sure if US can be reliably and accurately adapted to MRI. Rubesova et al. (14) have provided normative values for the total large bowel volume on MRI. Total colonic volume may be more accurate for assessing certain GI anomalies, but at present, until advanced software is available, the described method of drawing regions of interest of the colon on each slice may be time-consuming.
The rectal diameter may be affected indirectly by esophageal and duodenal atresia since both are associated with anal atresia. Both jejunal and ilieal atresia have shown micro-rectum with decreased signal on T1W sequences (3). Congenital anorectal malformations include a spectrum of anomalies ranging from imperforate anus to persistent cloaca due to failure of the uro-rectal septum to descend in the embryo. On fetal MRI the rectum may be dilated and if a vesico-rectal fistula is present the rectum will have a low signal on T1W imaging and a high signal on T2W imaging (3). Megacystis microcolon intestinal hypoperistalsis syndrome is a rare congenital disease characterized by functional bladder outlet obstruction and poor intestinal motility. Prenatal MRI will show an enlarged bladder, hydronephrosis, and absent or small colon with an associated midgut malrotation (3). Small left colon syndrome typically presents after birth as distal bowel obstruction and is associated with pregnancies of diabetic mothers. Typical neonatal findings are an abnormally narrow left colon with proximal dilation and an abrupt transition zone. Although usually diagnosed prenatally, MRI in the last weeks of pregnancy has the potential to demonstrate the altered calibers of the colon. Although Hirschprung’s disease is one of the most common causes of intestinal obstruction in the newborn, it is also usually diagnosed in the neonatal period and prenatal diagnosis is rare (15). If Hirschsprung’s disease presents prenatally, it is typically due to total colonic aganglionosis and shows dilated small bowel with normal colon caliber.
It is important to note that after FDR correction, our results did not differ significantly from those of Zalel et al. (Table 4) (1). This may indicate that established US measurements of other organs can be used on MRI studies. Our curves were slightly exponential whereas the US estimates were sigmoid. This is probably because our study group included fetuses from 25 weeks of gestation and theirs from 19 weeks.
We found that it was often difficult to differentiate the right colon from the adjacent distal ilial loops which are often a bright signal due to meconium. This is probably the reason that the right colon was the least adequately depicted.
The main limitation of this study is the lack of postnatal follow-up. Many of the pregnancies were outside referrals and therefore follow-up was not available. However, we only included fetuses with normal GI tracts on prenatal US and on the MRI studies, and we have >10 years of MRI fetal body reading experience with excellent postnatal correlation for infants born in our institution. In fact, none of the infants born to these pregnancies was diagnosed with a bowel disorder. Although we excluded pregnancies referred for GI disorders, our study is not purely representative of the general population as all pregnancies had an abnormality or suspected abnormality by US. The number of pregnancies for some of the pregnancies was relatively small (Table 3). Further studies with larger patient numbers may render growth curves more representative of pregnancies.
In conclusion, we present normal growth curves for the fetal colon and rectum as seen on T1W MRI at a gestational age of 25–39 weeks, including the 10th, 25th, 50th (median), 75th, and 90th percentiles. The data provided herein can be useful for radiologists interpreting fetal MRI studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.