
Abstract
A 29-year-old woman with partial placenta increta was treated by bilateral uterine artery embolization (UAE) for bleeding with hemorrhagic shock two months after delivery, resulting in permanent hemostasis. The patient underwent a total of three magnetic resonance imaging (MRI) examinations—before UAE and four days and four months after UAE. At four months, MRI showed a fully regenerated uterus with preserved perfusion and complete resolution of residual placental tissue.
Keywords
Introduction
Abnormal placentation is a rare (0.12–0.9%) complication of pregnancy with a high morbidity rate (1). Three forms are distinguished, depending on the depth of invasion of the uterine wall by the trophoblast: placenta accreta (∼80%); placenta increta (∼15%); and placenta percreta (∼5%).
Ultrasound (US) is the diagnostic gold standard for the assessment of abnormal placentation (2,3). However, in ambiguous US findings or suspicion of posterior placenta accreta, magnetic resonance imaging (MRI) has shown higher accuracy in the differentiation of the degree of placental invasion and provides information on the regional anastomotic vascular system (2–4).
Established treatment options include manual separation of the placenta and hysterectomy; however, there is a trend towards more conservative treatment options such as uterine artery embolization (UAE), which is minimally invasive, has few risks, and preserves fertility in most patients. To prevent possible complications, a close and safe follow-up consisting of clinical examinations and imaging of those patients is needed.
Case report
A 29-year-old woman spontaneously delivered a healthy boy (first pregnancy, first delivery). The placenta was retained and an attempt to separate the placenta manually and by curettage was discontinued after loss of 2000 mL blood. Ultrasound confirmed suspected partial placenta increta at the posterior uterine wall.
A first MRI was performed using a 1.5-T MR unit (Magnetom Avanto, Siemens Healthineers, Erlangen, Germany), performing T2-weighted half Fourier-acquired single shot turbo spin echo (HASTE) and T1-weighted (T1W) three-dimensional fast low angle shot (3D FLASH) sequences. T1W images (FLASH) in axial planes were obtained before and after an injection of 14 mL gadoterate meglumine (Dotarem, Guerbet, Aulnay-sous-Bois, France). MRI demonstrated a thinned posterior uterine wall with a hyperperfused placental residue, 6 cm in size, with flow voids and T2 dark bands (Fig. 1).
MRI before UAE: fat-saturated T1W TSE images acquired after administration of Gd-DOTA four weeks before UAE. Placenta increta with perfused residual placenta in the endometrial cavity with strong vessels at the posterior uterine wall and flow voids (arrows).
An interdisciplinary team made a decision for conservative management with close clinical monitoring as the patient wished strongly to have further children.
Two months after delivery, the patient developed severe vaginal bleeding and hemorrhagic shock which was treated by Bakri balloon tamponade and manual uterus compression.
Catheter angiography showed the hypervascularized placental residue from both uterine arteries (Fig. 2).
Pelvic angiography before UAE with uterine hyperperfusion from both uterine arteries (arrows) eight weeks postpartum.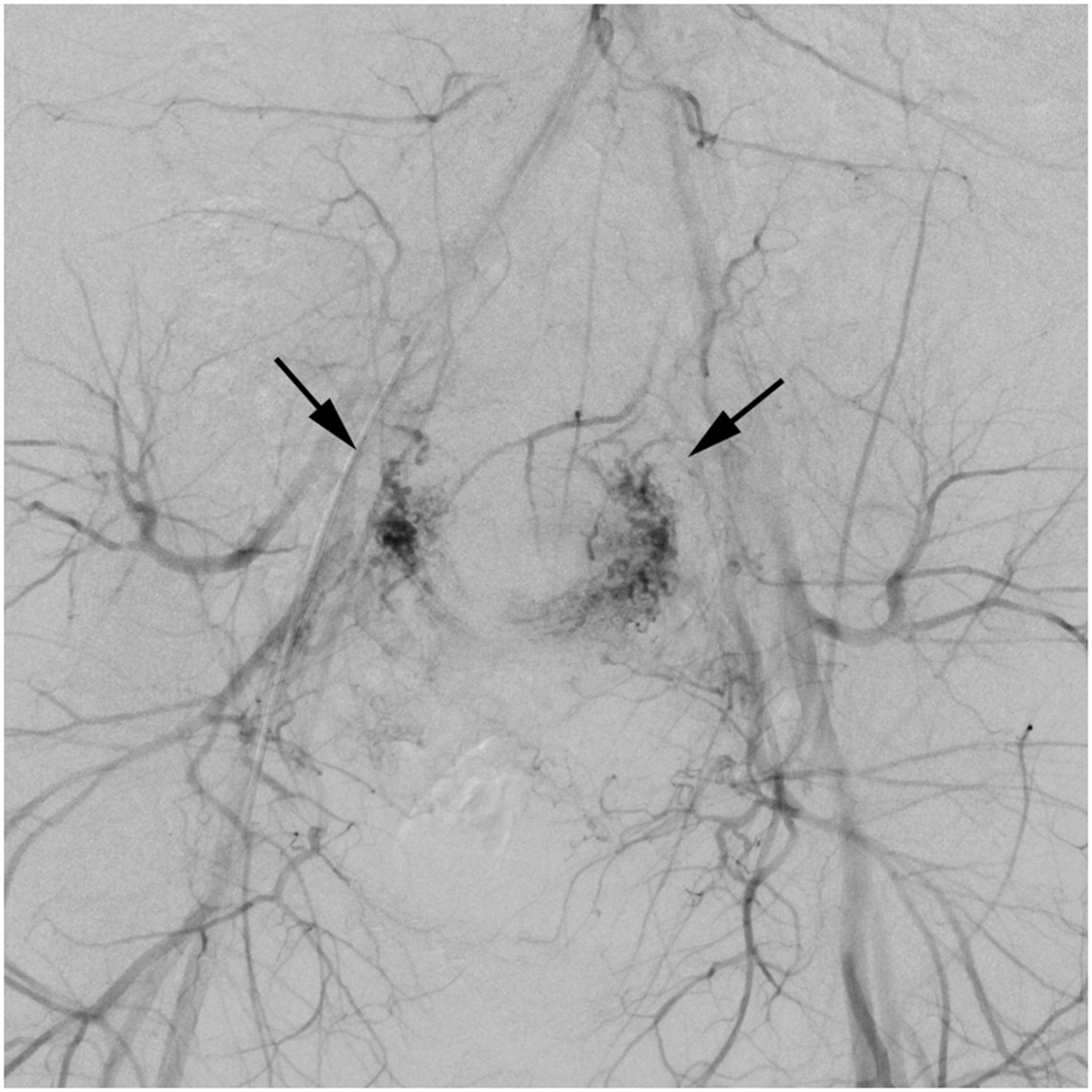
Both internal iliac arteries were probed with a 4F RIM catheter (Cordis, Fremont, CA, USA), and bilateral transarterial UAE was performed via a 2.5F Cantata microcatheter (Cook Medical, Bloomington, IN, USA), using polyvinyl ethanol particles (PVE) (Contour PVA Embolization Particles 500–710 µm, Boston Scientific, Marlborough, MA, USA). Additional absorbable gelatin foam particles (Gelfoam, absorbable gelatin sponge, Pfizer, New York, NY, USA) were injected, once marked flow reduction had been accomplished, to achieve complete stasis and at the same time avoiding a permanent occlusion of any vaginal side branches (Fig. 3).
Angiography before and after UAE: (a) contrast-enhanced angiogram of the left uterine artery prior to embolization with a 4F RIM catheter showing strongly enhanced, dilated corkscrew-like side branches (arrow). (b) Angiogram obtained after embolization via a 2.5 F microcatheter using polyvinyl ethanol particles (size = 500–710 µm) and administration of absorbable gelatin foam particles until stasis of blood flow is accomplished. (c) Angiogram of the right uterine artery prior to embolization. (d) Angiogram of the right uterine artery obtained after embolization.
The outcome of embolization was monitored by two further MRI examinations. The first follow-up MRI, performed four days after UAE, showed shrinkage and no perfusion of the residual placenta, while there was normal perfusion of the myometrium (Fig. 4a). Four months after UAE, no residual placental tissue was present in the endometrial cavity (Fig. 4b). The first menstrual bleeding began two weeks after UAE and a regular menstrual cycle of 26 days was restored thereafter.
MRIs after UAE: fat-saturated T1W TSE images acquired after administration of Gd-DOTA four days and four months after UAE. (a) Image acquired four days after UAE showing completely perfused uterus and non-perfused residual placental tissue in the endometrial cavity. (arrow) (b) Follow-up MRI four months after UAE showing normal-sized uterus with normal perfusion and no residual placenta in the endometrial cavity. There was no evidence of residual placental tissue and there was no relevant enhancement or contrast medium pooling.
Discussion
The prevalence of abnormal placentation is increasing as more Cesarean deliveries are performed. All three forms—placenta accreta, increta, and percreta—are associated with a high risk of peripartal hemorrhage and have a maternal mortality rate of up to 7% (5).
Distinguishing the three types of abnormal placentation is a diagnostic challenge. The two more invasive forms– placenta increta and percreta – have the highest mortality rate due to the high risk of profuse hemorrhage and infection. In these cases, conservative management is the preferred treatment and manual separation of the placenta is contraindicated. In cases with extensive residual placenta or after unsuccessful conservative treatment, hysterectomy is the safest treatment option.
UAE is a reliable method for stopping postpartum hemorrhage, where high success rates of up to 92% have been reported (6). More recently, there has been an interest in the prophylactic use of UAE for preventing hemorrhage after delivery in women with abnormal placentation. A review about the multidisciplinary management of patients with placenta percreta showed that women having adjunctive interventional radiology such as UAE, balloon occlusion of the internal iliac arteries, or both had a significant lower blood loss than those without this treatment (7). Complication rates of 3–13.3% have been reported (8–10), with severe complications being an absolute exception. Adverse effects on fertility are rare, and a pregnancy rate of 87.2% has been reported after UAE (10). While US is still the diagnostic gold standard in the assessment of abnormal placentation, MRI has proved to be very useful in doubtful cases and to evaluate the degree of myometrial invasion of the placenta. Both imaging modalities are widely used as diagnostic tools in abnormal placentation and have comparable sensitivity in the diagnosis (2–4). However, only few studies describe the potential of MRI in the follow-up of conservatively treated cases with abnormal placentation so far. Especially in cases of UAE, MRI seems to be a suitable imaging tool for follow-up, allowing both tissue characterization and assessment of myometrial viability. By evaluating the degree of placental vascularity, it may help to predict delay regarding complete placental resorption (11).
In the case presented here, we accomplished successful treatment of partial placenta increta with a single UAE and without postinterventional complications. What is noteworthy is the total recovery of the myometrium despite deep infiltration of the residual placenta, which could be visualized with MRI.
In conclusion, this case teaches us that bilateral UAE can be a very successful and fertility-sparing, minimally invasive treatment option in patients with postpartum hemorrhage due to abnormal placentation. The timely consideration of prophylactic UAE in patients with abnormal placentation, even if asymptomatic, may be helpful to prevent complications. Assessment of the perfusion and viability of the post-treatment uterus with MRI allows reliable evaluation of outcome after UAE.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Bernhard Gerbauer receives speaker honorarium and/or travel allowances from BAYER, Pfizer, Roche, Parexel, Cook, Sirtex, Boston Scientific, C.R. BARD, AngioDynamics, Siemens, Philips.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.