
Abstract
Background
There are limited studies about testicular microlithiasis (TML) and background information such as health, lifestyle, and socioeconomic status.
Purpose
To assess the prevalence of TML in relation to socioeconomic status and ethnicity.
Material and Methods
From a database of scrotal ultrasound examinations in a single institution, all men who underwent routine ultrasound examinations for a variety of symptoms from 1998 to 2015 were included. Skilled observers performed all examinations, and presence of any form of intra-testicular calcification, including TML, was recorded on the examination report and a representative image obtained and stored. A total of 1105 cases with TML were reviewed and random sample of 1105 controls from the same database was also reviewed. Demographics were recorded including ethnicity (white, black, and others) and socioeconomic groups (IMD Quintile).
Results
Black men had increased prevalence of TML (odds ratio [OR] = 2.17, 95% confidence interval [CI] = 1.72–2.75) compared with white men. Among the 1105 TML cases, 423 (38.3%) were white, 273 (24.7%) black, 152 (13.8%) had other ethnicities, and 257 (23.2%) had no ethnicity recorded. In the control group of 1105 men without TML, 560 (50.7%) were white, 171 (15.5%) black, 111 (10.0%) had other specified ethnicities, and 263 (23.8%) had no ethnicity recorded. Men from the most deprived socioeconomic groups had higher prevalence of TML than men in the most affluent groups, with a trend in OR from the least deprived to the most deprived group.
Conclusion
Pathogenesis and clinical relevance of TML is unknown but our results point towards possible ethnic and socioeconomic variation in the underlying causes of TML.
Keywords
Introduction
Testicular microlithiasis (TML) is a common condition, with a prevalence close to 6% in adults (1). TML can be readily visualized on an ultrasound examination of the testicles. Priebe and Garret described testicular calcification in 1970, when noticed on a pelvic X-ray of a four-year-old boy (2), TML detected by ultrasound was subsequently described by Doherty in 1987 (3).
TML is characterized by the appearance of minute calcifications in the lumen of the seminiferous tubules (4,5), and is shown on ultrasound as bright echogenic foci of 1–3 mm in diameter within the testicular parenchyma. There is no acoustic shadowing, and TML can be either unilateral or bilateral. TML may be widespread throughout the whole testicle or have a more limited distribution. TML detection has low inter-observer variability by ultrasound (κ = 0.86) (6).
TML has been suggested to be associated with testicular cancer, but this relationship remains debatable. Furthermore, ultrasound follow-up does not appear to benefit patients with no additional risk factors (7–9). The causes and pathogenesis of TML are unknown. However, it seems that there might be an association between ethnicity and the presence of TML. Peterson et al. found variation in TML prevalence between ethnic groups of asymptomatic men (1). Several studies report a higher risk of testicular cancer in men of high economic status (10,11). To our knowledge no information exists about socioeconomic status in men with TML.
Our aim was to assess the prevalence of TML in ethnic and socioeconomic groups in England.
Material and Methods
All testicular ultrasound examinations were performed by skilled, experienced operators following a standard protocol, which included obtaining representative images of normal and abnormal findings. A standard examination report documented identification of abnormalities including TML (Fig. 2) and macrocalcification (>3 mm). Images and the examination report were stored on a central database. All data were collected as a part of routine clinical practice. This study was not defined as a research study according to the National Health Service “defining research” decision tool and therefore in the UK there was no requirement for a submission to be made for ethics committee approval.
An image of a testicle with appearances of classical TML.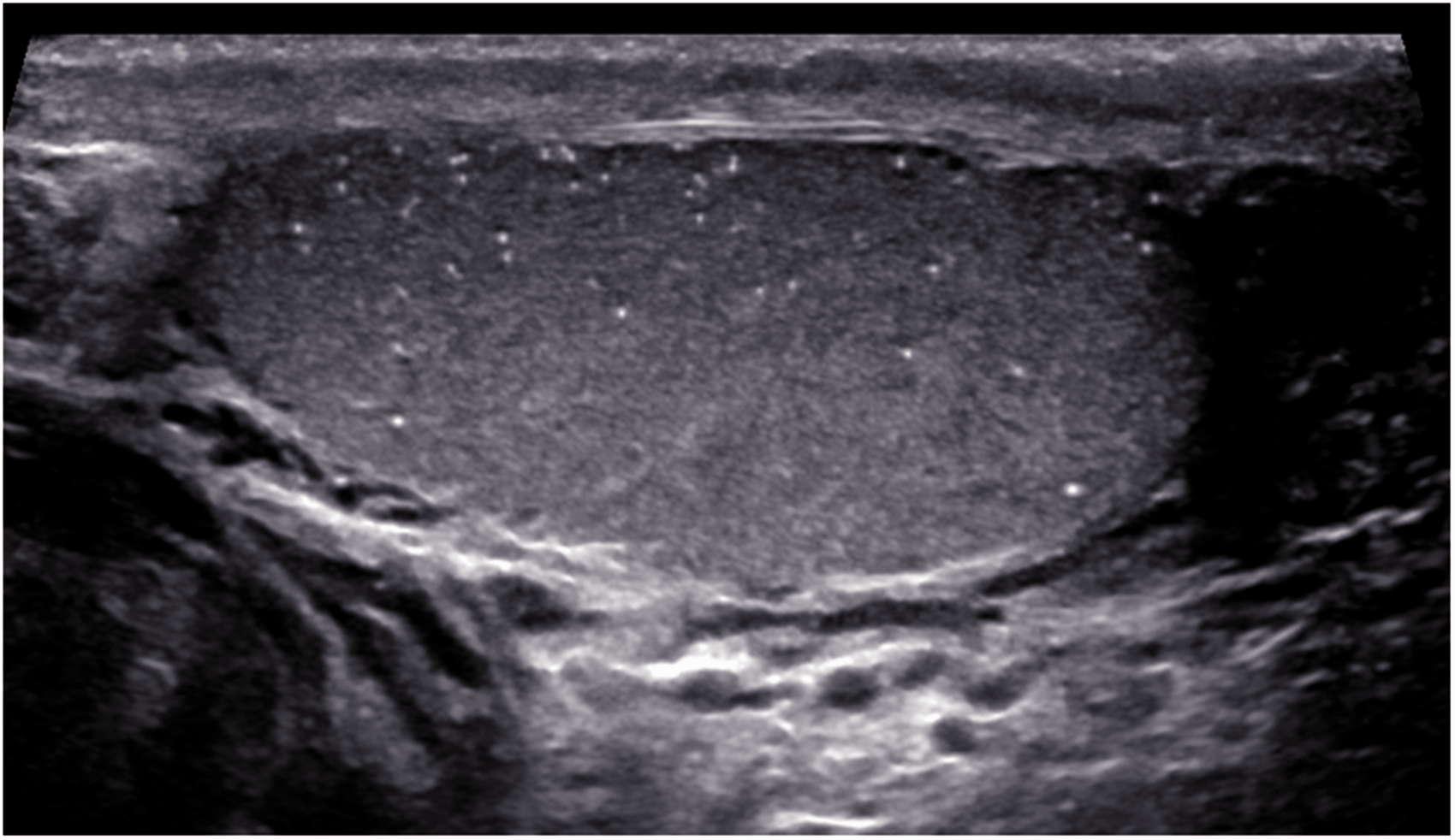
Database
A search of two archiving systems, a radiology reporting system (Complete Radiology Image System (CRIS™), Healthcare Software Systems, Mansfield, UK) and a Picture Achieve Communication System (PACS, Centricity™, GE Healthcare, Barrington, IL, USA) in King’s College Hospital in southeast London, included a total of 39,961 ultrasonography examinations of the scrotum between 1998 and 2015. The predominant indications for a scrotal ultrasound examination included pain, discomfort, lump, or testicular mass, and reflect the referral pattern to the department in general. This TML population has been described previously in other publications (12–14).
TML cases
From the 39,961 scrotum examinations, a search of the ultrasound reports (search terms: calcification, microlithiasis, TM, and TML) identified a total of 1105 men with TML. We gathered information from these TML cases (≥ 5 microliths), the laterality of TML (left, right, or bilateral), and if any macrocalcification (> 3 mm) was present.
Controls
A random cohort of 1105 patients with no record of TML from the study population of 39,961 examinations served as a control group.
Data
From the Electronic Patient Record System (iSoft™ Clinical Manager, Sidney, Australia) and PACS we obtained the following data on TML cases and controls; age at time of examination; year; ethnicity; and home address postcode.
Patient age and year were derived at the time TML was diagnosed, and among controls age and year were derived from the randomly selected ultrasound examination. Ethnicity was categorized into four groups: white; black; other specified ethnicities; and not known.
Socioeconomic status was derived from the home address postcode. The postcodes in England are shared among 20–100 households and postcodes are conventionally used to derive socioeconomic status (15). The deprivation index was assessed from the Index of Multiple Deprivation 2015 (IMD 2015) (16,17).
Statistical analysis
In order to compare characteristics of TML cases and controls, we calculated prevalence ORs for TML in relation to age, year, ethnicity, and socioeconomic status, using logistic regression. Age was included in the model as a second-order polynomium. We calculated OR with a 95% CI using STATA statistical software (version 14.1, STATA corporation, College Station, TX, USA).
Results
The median age of the TML cases was 37 years (age range = 1–88 years) and for the controls 38 years (age range = 1–92 years) (Fig. 1).
The age distribution of TML cases and control patients.
Of the 1105 TML cases, 168 (15.2%) men had TML in the right testicle, 155 (14.0%) in the left testicle, 599 (54.2%) were bilateral, and in 183 (16.6%) cases laterality was unspecified.
A total of 113 men had limited TML and 990 had classic TML and in two patients TML was unspecified. In addition, macrocalcifications were found in 159 TML cases (14.4%).
The distribution of ethnicity and socioeconomic status between the TML cases and the control group.

IMD quintile 1 is the most affluent and IMD quintile 5 the most deprived.
IMD, index of multiple deprivation; OR1, adjusted for age and year; OR2, adjusted for age and year and mutually adjusted.
Black men had increased prevalence of TML compared with white men (OR = 2.17, 95% CI = 1.72–2.75) (Table 1). Men from the least deprived socioeconomic group had the lowest prevalence of TML (OR = 0.19, 95% CI = 0.12–0.30) compared with the IMD quintile 4, and men from the most deprived socioeconomic group had the highest prevalence of TML (OR = 1.05, 95% CI = 0.86–1.30) compared with the IMD quintile 4. Mutual adjustment of ethnicity and socioeconomic status attenuated the associations slightly, but both remained independently associated with TML.
When we restricted the case group to include only men with macrocalcifications, a lower prevalence of macrocalcifications were seen in the least deprived socioeconomic groups (OR = 0.19, 95% CI = 0.06–0.64) compared with the most deprived socioeconomic groups (OR = 1.17, 95% CI = 0.71–1.93). This trend was also seen when we restricted the case group to include only cases of men with limited TML or only cases of men with classic TML.
Discussion
Overall, we found black men had a higher prevalence of TML compared with white men, and men from the most deprived socioeconomic groups had the highest prevalence of TML. To our knowledge, this is the first report of TML in relation to socioeconomic status.
The prevalence of TML in the general population is unknown. Peterson et al. investigated 1504 healthy asymptomatic men aged 18–35 years and found an overall TML prevalence of 5.6%. Subdividing according to ethnicity and prevalence in white, Asian/Pacific, Hispanic, and black men was found to be 4.0%, 5.6%, 8.5%, and 14.1% (1). Other studies have assessed the prevalence of TML in symptomatic patients to be around 8–18% (13,18–20).
Testicular macrocalcifications have only been rarely described in the literature and have typically been viewed as of no clinical significance (21–23). The prevalence of macrocalcifications has been reported to be 2.0% (67/3435 scrotal ultrasound-examined patients) (24), 2.7% (23/868 scrotal ultrasound-examined patients) (25), and 9.6% (73/758 scrotal ultrasound-examined patients with testicular pain) (26). We found 14.4% of TML cases to have macrocalcifications. It has been suggested that macrocalcifications could be associated with malignant tumors (22,27) or trauma (22); further studies are required to verify these relationships. A number of reports have suggested that metastatic germ cell tumors can be traced to a regressed calcification area within a testis, raising the concept of a “burnt-out tumor” as the source of metastases (28–30).
In daily clinical practice, men with TML and additional risk factors are offered ultrasound follow-up. TML varies among different ethnicities and ethnicity could be considered a risk factor. Trabert et al. investigated testicular cancer incidence from 1973 to 2007 worldwide and found the incidence of testicular cancer varying between ethnic groups. The highest rates were observed in European and North American countries and lowest in Asian and African countries, e.g. Norway had an incidence rate of 10.5 per 100,000 man-years compared with Uganda with 0.3 per 100,000 man-years. Black men have a low rate of testicular cancer (31). In our study, we found that black men had the highest prevalence of TML, which is the reverse of the known variation in testicular cancer incidence. This argues against an overt association between TML and testicular cancer, or a causal link between the two. Also, the diverse group “other specified ethnicities” had a higher TML prevalence than white, which also suggests that ethnicity is a risk factor.
The strength of this study is the large number of included patients and the availability of information on ethnicity and socioeconomic status. Postcodes in England are usually only shared among 20–100 households and the derived socioeconomic status is highly indicative of a range of health outcomes (15). It is possible that ethnicity was entered in the hospital systems with a degree of error, but we know that the recorded information correctly indicates, for example, the known difference in prostate cancer incidence in black and white men (32).
TML is a symptomless condition and is often seen incidentally in scrotal ultrasound examinations. The indication for an ultrasound examination of the scrotum is variable and our study population is selected on the indication for ultrasound examination. However, given that these indications are wide and TML does not typically have specific symptoms, we consider it most likely that the observed associations are real and would be replicated in a study of the general population.
In conclusion, black men had a higher prevalence of TML than white men and TML prevalence was higher among the most socioeconomic deprived groups. Our results point towards a possible variation in the underlying causes of TML related to ethnicity.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: The Region of Southern Denmark supported this study.