
Abstract
Background
The primary neuroendocrine skin cancer, Merkel cell carcinoma (MCC), has a well-known predilection to metastasize systemically. However, the experience of systemic metastases in MCC is mainly disseminated through case reports due to the rarity of MCC.
Purpose
To elucidate the frequency and locations of systemic metastasis in MCC by reviewing the imaging of patients with metastatic MCC in a national cohort.
Material and Methods
Patients with diagnosed metastatic MCC by imaging studies in Finland during 1999–2012 were included in this study. We reviewed their imaging studies to evaluate the most frequent sites for systemic metastasis and determined the latency between the primary tumor diagnosis and systemic metastasis. The material includes 30 MCC patients with complete imaging series and 187 examinations, of which 102 (54%) were CT images.
Results
The mean latency from the primary tumor diagnosis to systemic metastasis was 2.1 years and the mean latency between the radiologic diagnosis of the metastases and death was 299 days. Metastases were recorded in several organ systems in most of the cases, and at least two separate metastatic sites in 63% of the cases. Metastatic spread was noted in 60% of the cases in distant lymph nodes. Liver and lungs were the most affected solid organs.
Conclusion
Systemic metastasis in MCC has no predilection site, basically every organ system can be involved. Most of the systemic metastases were recorded during the first two years after the MCC diagnosis.
Introduction
Merkel cell carcinoma (MCC) is a rare neuroendocrine skin cancer that occurs mainly in fair-skinned, elderly individuals. Globally, 80% of the tumors are initiated by Merkel cell polyoma virus (MCV) DNA integration into the cancer cells early in MCC development (1). MCC has an inherent capacity for early and aggressive local and systemic dissemination (2). Approximately 65–70% of the patients present with clinically localized disease to the skin (American Joint Committee on Cancer [AJCC] stage I or II), 25–26% have palpable regional lymphadenopathy AJCC stage III, and 5–8% have distant metastasis, AJCC stage IV (3,4). The draining lymph node basin is most commonly the first site of metastasis, in 27–60% of the cases (5,6). Distant dissemination occurs in up to 40–50% of patients that develop visceral metastasis, particularly prevalent in the lungs, liver, and bone (7,8). Owing to the aggressive course of the disease, its mortality exceeds those of other forms of skin cancers (9). About one-third of the patients die of MCC including all stages and courses of disease (10).
Current treatment guidelines for MCC entail imaging studies during the course of the disease (11), from the preoperative stage to the postoperative follow-up. In addition to the clinical examination, ultrasound (US) of the loco regional nodes and total body positron emission tomography–computed tomography (PET-CT) will complete the staging in preoperative examinations (11) and direct the choice of the surgical treatment modality. In the follow-up, nodal US and CT or PET-CT are proposed (11). However, it is not clear whether imaging has any role in the follow-up of MCC patients.
The rarity of the prevalence of MCC limits the amount of information on the experiences on systemic metastases in MCC and the available information is mainly case reports. Reasons for this paucity of information might lie in the fact that when the disease has metastasized, it is considered incurable (11). This retrospective study was designed to assess the most frequent sites for systemic dissemination in MCC and to determine the latency between the primary tumor diagnosis and systemic metastasis by imaging.
Material and Methods
The study was approved by the Ethics Committee of the Helsinki University Hospital. The Ministry of Health and Social Affairs granted authors the permission to collect the patient data for study purposes. Permission to retrieve all images for study purpose was granted by the National Institute for Health and Welfare. Inclusion criteria for this study was that patient was diagnosed with systemic metastases MCC and images were available for review. No informed consent was required as all the patients had deceased prior to the study commencing.
Our group has gathered primary MCC tumor samples available in Finland since 1978. Immunohistochemistry served to validate all of the diagnoses. To accompany the tumor samples, comprehensive patient records have been gathered from hospital files and Finnish Cancer Registry records. The ongoing MCC projects of our research group continue to use this database.
A total of 57 MCC patients diagnosed between 1979 and 2013 with systemic metastases were identified. Imaging studies of these patients were retrieved for analysis. When autopsy was performed, the autopsy report was compared with the radiologic findings. All medical records and images were reviewed and detailed data on patient and tumor characteristics, including tumor size, location, stage of disease at the time of diagnosis, local recurrence, local and systemic metastasis, and survival, were obtained from the hospital and primary healthcare center files of the patients fitting the inclusion criteria. All included patients were staged according to the AJCC classification for this study (3). A total of 27 patients were excluded from this study because, due to archiving regulations, no imaging studies were available.
Imaging series were re-evaluated blindly by an experienced radiologist (EL), and lesions were categorized on the basis of the anatomical locations. Distant lymph node metastasis was classified as systemic metastasis to the lymph nodes beyond the nearest regional area of the primary tumor.
Results
Demographic, treatment, tumor, and latency data for 30 patients with MCC.

BSc, bone scintigraphy; CT, computed tomography; DLN, distant lymph nodes; FDG-PET-CT, fluoro deoxy glucose positron emission tomography–computed tomography; MRI, magnetic resonance imaging; NA, not available; ST, subcutaneous tissue; THX, thorax; US, ultrasound.
All patients received some type of treatment for their MCC before the detection of the metastases. In 28 patients (93%) the treatment was surgical intervention (Table 1). In 13 (43%) of the cases, surgery was the only treatment before the detection of metastatic spread. The most frequent adjuvant treatment was radiation therapy given to 14 (46%) cases followed by chemotherapy in two cases (7%).
Of the 187 imaging examinations, 102 (54%) were CT images, 62 (33%) were conventional chest X-ray images, 12 (6%) were magnetic resonance imaging (MRI), seven (3.7%) were ultrasound exams, two (1%) were PET-CT, and two (1%) were bone scintigraphy.
Mean latencies between presentation and metastases diagnosis by imaging stratified by time and site of the metastases.

Sites, numbers of metastases, and imaging modalities in 30 patients with MCC.
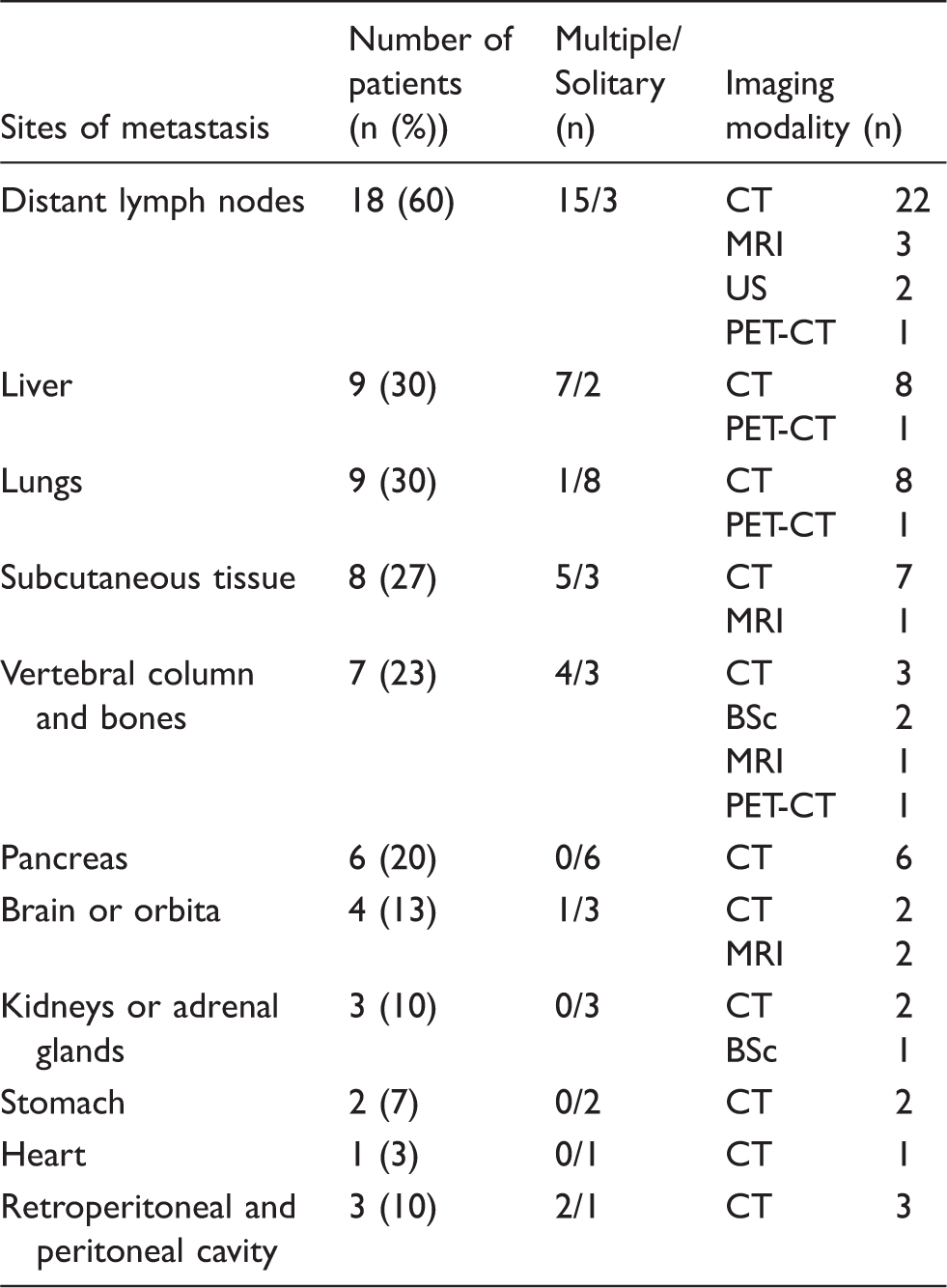
Typically, metastases in the distant lymph nodes, retroperitoneal and peritoneal cavity, liver, subcutaneous tissue, and bones presented with multiple metastatic foci (Figs. 1 and 2). In the lungs, pancreas, stomach, and heart, the metastasis usually presented as a solitary focus.
Multiple liver metastases in a patient with primary tumor in the neck (patient 1). Most of the metastases are enhanced by contrast medium in the arterial phase images (a) and show washout in venous phase images (b). Large retroperitoneal, peritoneal and subcutaneous metastases in a patient with primary tumor in the neck (patient 27).

Discussion
The imaging studies in patients with metastatic MCC were reviewed. No predilection site for distant metastases were found, as every visceral organ, skeletal system, subcutaneous tissue, and distant lymph nodes were involved. However, there is presently no clear agreement on the role of imaging in the management and follow-up of MCC (12). A recent European consensus advocates follow-up with nodal US together with once a year CT or PET-CT for up to five years (11). The NCCN Clinical Practice Guidelines in Oncology on MCC recommends imaging studies to be performed as clinically indicated during the follow-up (13).
The most frequent metastatic site found in this study was distant lymph nodes. This finding was in concordance with previous studies (12). The liver and lungs were the most frequently affected solid organs, which was in line with previous literature (7,8). Current treatment guidelines for MCC consider surgery the mainstay of treatment (11,13). Sentinel node biopsy is indicated for patients with clinically node negative disease, whatever the size of the tumor, in combination with wide excision of the primary tumor (11,13). Sentinel node biopsy may reveal thus patients with occult metastasis and predict unfavorable course of disease (14,15). Recent data point to the direction that primary tumor size does not predict nodal involvement, which is contrary to an earlier paradigm (16,17). However, when the disease has metastasized, there is currently no established curative treatment (11).
The median time to recurrence in MCC patients was approximately eight months, with 90% of the recurrences occurring within 24 months (5,18,19). Subcutaneous metastases in this series had the shortest mean latency from the MCC diagnosis with a time span of only 12 months, a further 66% of the patients were diagnosed with metastases within 24 months. All patients in this study died a mean of just ten months (range, 14 days–7.4 years) after distant metastases were confirmed. This falls well within the range reported in previous literature, where survivals were just nine to 12 months after metastatic disease was recognized, depending on the study (5,20–22).
MCC was once regarded as an indolent skin tumor (23–25), but it has since proven to be one of the deadliest of skin cancers. Although rare in incidence, in Europe with an annual incidence rate of 1.3/1,000,000 (26), MCC is the second most common cause of skin cancer deaths after melanoma, with an estimated cause-specific death rate of 0.43 per 100,000 persons (27). Most of the MCC patients die with non-localized, i.e. metastatic disease (28), which accords with the findings in other cancers (29). Most of the patients present with localized disease (4). Nevertheless, MCC grows rapidly within just few months (2) and tumor doubling times are five to 12 days, or even as rapid as one to five days in the most aggressive tumor subtypes (30).
This study has several limitations that should be acknowledged. One inherent limitation lies in the retrospective design and relatively small number of patients. Further, most of our imaging studies were performed as clinically indicated. The archiving of images is only 20 years in Finland; therefore, we were not able to get access to all the images of MCC patients with metastatic disease. Although MCC has been recognized and characterized since 1972 (31), it was not until the discovery of the Merkel cell polyoma virus in 2008 (1) that an enormous interest in MCC arose, both in research and reporting clinical experience. The rapidly expanding body of knowledge regarding MCC has just recently generated treatment recommendations (11,13). Apart from studies in the 1980s and 1990s, there has been little interest in reporting the metastatic disease due to the fact that there is no curative treatment for metastatic MCC.
In conclusion, this current study showed that systemic metastasis in MCC has no predilection site or organ, as basically every organ system was involved in our study. Most of the systemic metastases were recognized during the first two years after the MCC diagnosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding from Cancer Foundation grant.