
Abstract
Background
The relationship between the signal from retrograde venous flow on magnetic resonance angiography (MRA) and retrograde upward flow from the left brachiocephalic vein has not been explored.
Purpose
To reveal the frequency of jugular venous reflux using MRA and nuclear venography in patients being evaluated for cerebral volume and blood flow.
Material and Methods
A total of 229 patients with cognitive disturbance who had undergone brain magnetic resonance imaging (MRI) and single-photon emission computed tomography (SPECT) on the same day to evaluate cerebral blood flow were evaluated. Jugular venous reflux was measured on MRA and nuclear venography, which was conducted just after injection of N-isopropyl-123I-p-iodoamphetamine for the SPECT study.
Results
MRA showed jugular reflux in seven patients on the right side, and in 22 on the left. Nuclear venography showed jugular reflux in six patients on the right side, and in 20 on the left.
Conclusion
Jugular venous reflux was observed mostly on the left side. Retrograde flow was observed on both MRA and nuclear venography in half of the cases, with the rest only on one of the modalities.
Keywords
Introduction
Three-dimensional (3D) brain time-of-flight (TOF) magnetic resonance angiography (MRA) shows caudocephalad blood flow as high signal intensity in vessels. High signal intensity is clearly seen in cerebral arteries, but high signal intensity is also observed in 1–6% of venous structures (1–3). High signal intensity, when present predominantly in the lower dural sinuses, suggests the diagnosis of dural arteriovenous fistula and necessitates differentiation from retrograde venous reflux. MR imaging (MRI) is performed in the supine position, in which flow velocity in the left brachiocephalic vein is slow owing to the anatomical relationship between the aortic arch and sternum. In some patients, the left brachiocephalic vein is compressed by these structures, resulting in severe narrowing (4). This narrowing and compression can result in retrograde flow in the left internal jugular vein (1,4,5). Such retrograde flow is reportedly seen more frequently in older patients (2,3).
Radioisotope (nuclear [RI]) venography is a convenient and minimally invasive technique that has been described in several reports, including a case report of a dynamic brain flow study with injection of RI into the left arm (6), and a report of superior vena cava (SVC) syndrome (7). Brain single-photon emission computed tomography (SPECT) is frequently used for cerebral blood flow (CBF) evaluation in patients with cerebral ischemic disease and cognitive disorders (8,9). Statistical analysis using volumetric data from 3D MRI has also been applied in patients with cognitive disorders (10) and might be useful for monitoring cognitive disturbance due to intracranial pathogenic processes, including vascular dementia (11,12). The graph plot method, a technique that uses N-isopropyl-123I-p-iodoamphetamine (IMP) and SPECT for non-invasive measurement of regional CBF, has been developed and applied in the clinical setting (13,14). Nuclear venography data are used for calculation of the graph plot method during injection of the radionuclide.
It might be useful to use nuclear venography as the gold standard for jugular venous reflux when we see high signal intensity in venous structures; however, no reports have evaluated the relationship between the signal assumed to be generated by retrograde jugular venous flow on MRA and retrograde upward flow from the left brachiocephalic vein on nuclear venography findings. The purpose of this study was to reveal the frequency and the pattern of retrograde venous flow with the two modalities by assessing MRA and nuclear venography results in elderly patients.
Material and Methods
Participants in this study were patients with mild-to-moderate cognitive disturbance who had been referred for screening for intrinsic brain lesions and brain perfusion abnormalities by MRI and nuclear angiography. Local institutional review board approval was obtained for this retrospective study and the need for written informed consent was waived. Patients underwent MRI and nuclear venography on the same day. Both exams were performed within 1.5 h. The order of MR and nuclear imaging was allocated randomly. No patients had an arteriovenous shunt for hemodialysis. Patients who were unable to complete either MR or nuclear examination were excluded.
MRI
MR was performed using a 1.5-T system (Excelart Vantage; Toshiba Medical Systems, Otawara, Japan) with a 4-channel head coil. 3D TOF MRA was performed with other diagnostic sequences, including 3D volumetric T1-weighted (T1W) imaging, T2-weighted (T2W) imaging, and T2*-weighted (T2*W) imaging as part of routine brain screening. Imaging parameters for 3D TOF MRA were as follows: repetition time, 30.0 ms; echo time, 2.5 ms; flip angle, 20°; field of view, 210 × 200 mm; matrix, 256 × 192; section thickness, 1 mm; 180 sections.
Radionuclide imaging
SPECT studies were performed using a rotating dual-headed gamma camera (Symbia E; Siemens Healthcare GmbH, Erlangen, Germany) with a low–medium-energy, general-purpose collimator. Nuclear venography targeting the upper mediastinum and neck was performed before SPECT imaging of the brain. The patients were kept supine with their arms by their sides and the neck held in a neutral position with a holder. A bolus of 2 mL of fluid containing 123I IMP (222 MBq/kg) was injected and flushed with 20 mL of normal saline via the left median antecubital vein. The patients were asked to continue normal tidal breathing, avoiding Valsalva’s maneuver. The gamma camera was placed anteriorly over the neck and upper chest. Normal nuclear venography is shown in Fig. 1. Data were stored in frame mode at 1 frame/s for 2 min using 64 × 64 matrices.
Sequential frontal images of normal nuclear venography (early phase, left upper row to late phase, right lower row) injected via the left antecubital vein are shown. Most of the RI moved rapidly from the left subclavian vein (large arrowhead) to the brachiocephalic vein (small arrow) and superior vena cava (small arrowheads). Isotope then moved to the pulmonary arteries, then to the lungs (large arrow, late phase).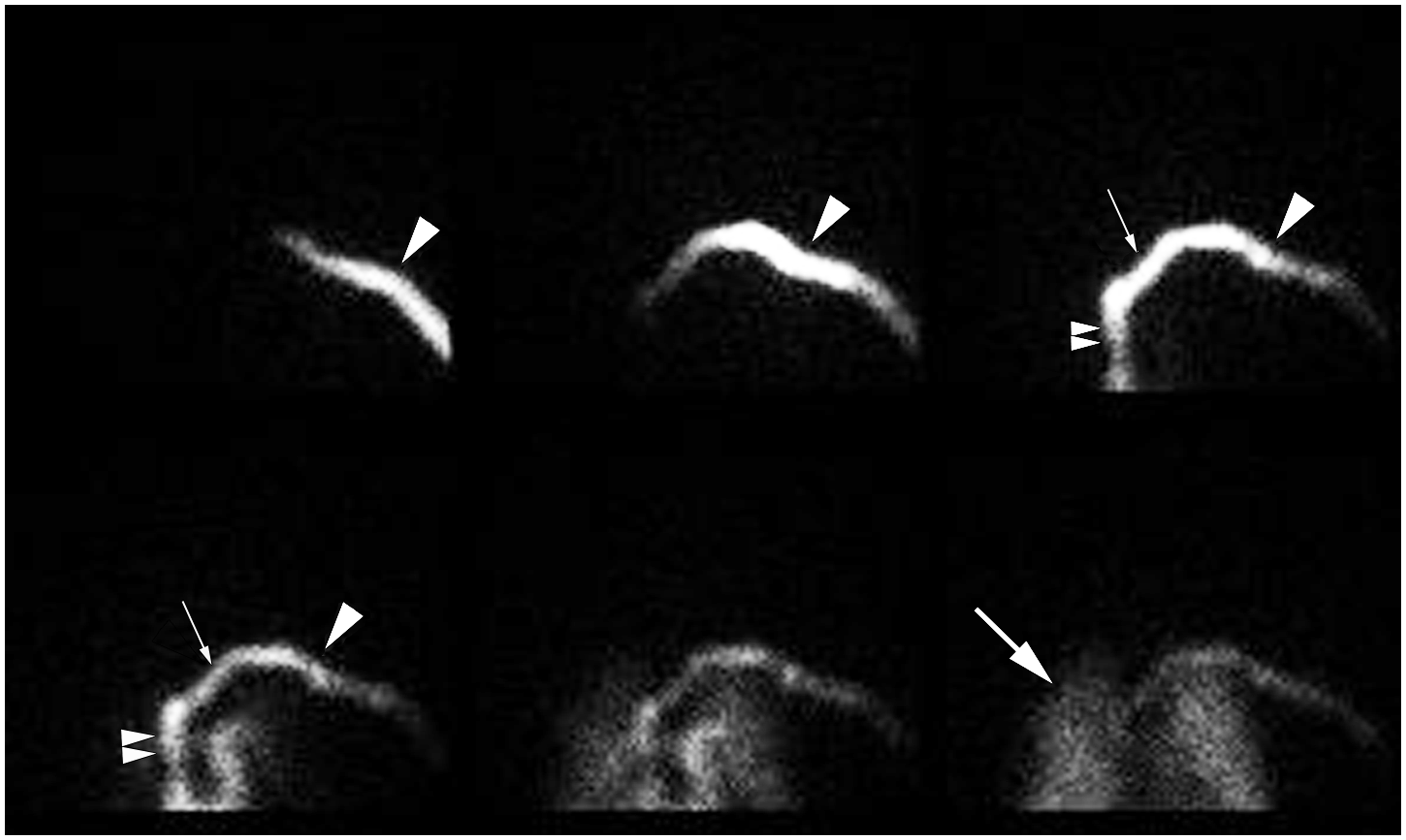
Data analysis
DICOM data from MRA and nuclear venography were transferred to the workstation (ZIO workstation; Ziosoft, Tokyo, Japan) and anonymized. The data were then transferred to an offline workstation-type PC. Two board-certified neuroradiologists, SO and YF, with 8 and 15 years of experience, respectively, independently reviewed the data (zioTerm2009 software, Ziosoft, Tokyo, Japan) (15).
Upward venous jugular reflux flow in the sigmoid/transverse sinus (SS/TS) and inferior petrosal sinus was measured using each modality. In MRA, the inferior 5 mm of the imaging slab was excluded from analysis to avoid artifacts. Since upward venous flow is not usually observed, the length of bright continuous signal in the sigmoid/transverse sinus and inferior petrosal sinus were measured on brain TOF MRA and the longest venous signals were recorded and judged as positive venous reflux into the right jugular vein (RJV) or left jugular vein (LJV). No other venous structures were included for analysis. In nuclear venography, upward retrograde flow into the left jugular vein from the left brachiocephalic vein was evaluated and the length of maximum retrograde flow was measured. The distance of retrograde upward flow into the SVC was also measured in the right jugular vein. This means a roundabout return to the SVC was counted as retrograde flow.
Statistical analysis
The measured data between the two readers were averaged. Interrater concordance regarding the extent of retrograde flow on both MRA and nuclear venography was performed between raters (MedCalc version 12.2.1 software, MedCalc Software, Ostend, Belgium). Kappa scores were calculated.
Results
Number of patients with positive and negative venous reflux and extent of venous reflux.


An 86-year-old woman. Maximum intensity projection (MIP) image of MRA showed positive jugular flow at the left dural sinus (white arrows). Brain SPECT was performed for this patient on the same day as MRI. Nuclear venography was conducted via the left antecubital vein and most of the isotope moved from the left subclavian vein to the brachiocephalic vein, although a small amount of cephalad jugular flow was detected in the continuous frames of frontal view of early phase nuclear venography (white arrowheads).
A 78-year-old woman. MIP image from MRA shows positive jugular flow at the left dural sinus (white arrows). Brain SPECT was performed for this patient on the same day as MRI. Nuclear venography was conducted via left antecubital vein injection and a 140-mm length of cephalad jugular flow was seen in the continuous frames of frontal view of early phase nuclear venography (white arrowheads).

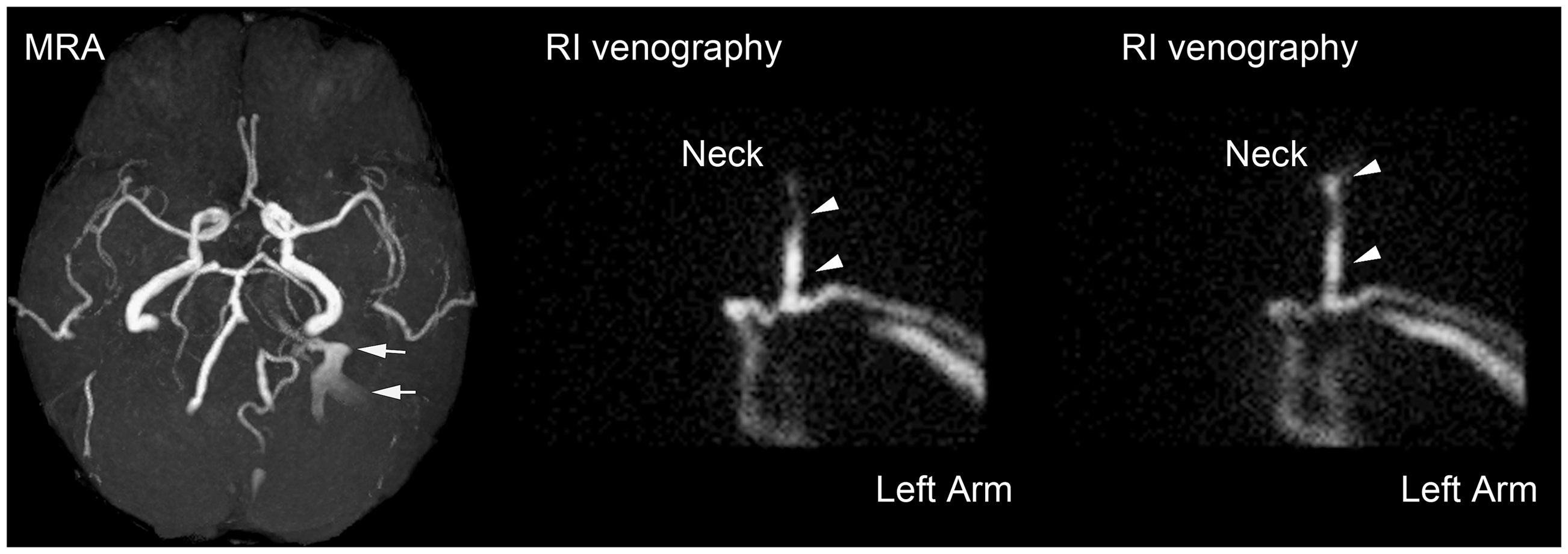
An 85-year-old woman. MIP image from MRA shows slight positive jugular flow at the right dural sinus (white arrow). Brain SPECT was performed on the same day as MRI for this patient. RI venography was conducted via a left antecubital vein injection. Stenotic change at the terminal portion of the left brachiocephalic vein (white arrowheads) and return to the SVC via collateral venous channels (small white arrows) were revealed in the frontal view frames from the early-to-middle phase nuclear venography, which probably hindered return of right jugular flow to the SVC. The difference in height between the collateral venous channels and SVC was measured as 65 mm.
MRA
Positive reflux was seen in seven patients on the right side and in 22 on the left side. The mean extent of jugular reflux was 10.7 ± 3.5 mm on the right side and 17.5 ± 9.6 mm on the left side. Kappa values were 0.956 for RJV and 0.964 for LJV.
Nuclear venography
Positive reflux was seen in six patients on the right side and in 20 patients on the left side. Kappa values were 0.928 for RJV and 0.980 for LJV. The mean extent of jugular reflux was 41.5 ± 22.7 mm on the right side and 42.1 ± 29.3 mm on the left side.
Jugular reflux in four patients on the right side and ten patients on the left side was revealed on both modalities (Table 1). For the rest of sides of the patients with positive jugular reflux, jugular venous reflux was revealed only with one modality: MRA, n = 3 on the right side, n = 12 on the left side; nuclear venography, n = 2 on the right side, n = 10 on the left side.
Discussion
This study offers the first comparison of the signals from the venous system that are assumed to be derived from jugular reflux on MRA and nuclear venography, which were conducted on a single day. Most previous studies were single-modality studies and have focused on patients with high signals in the venous system on 3D TOF MRA. Several large studies have featured retrograde venous flow on MRA (13). Of 1078 study patients (mean age, 63 years), 67 (6.2%) showed high signals in dural sinuses on source images from 3D TOF MRA, indicating the presence of retrograde flow. Retrograde flow was identified mainly in middle-aged and elderly patients in the supine position in the left inferior petrosal sinus or left sigmoid sinus. This phenomenon should not be misdiagnosed as a dural arteriovenous fistula, which might require further investigation (1). Other large series have shown ten (1.3%) of 732 healthy participants (mean age, 56.7 years) (2) and 55 (1.6%) of 3453 patients (3) with high signal intensity in the left dural sinus. Our study revealed higher rates of venous reflux (8.7–9.6%), probably because elderly patients with cognitive disorders were targeted for our study.
The cause of venous reflux has been speculated on in the literature. Tanaka et al. concluded that the left brachiocephalic vein was compressed to the point of occlusion between the aortic arch and sternum during tidal ventilation, which could be the major cause of the frequently increased signal intensity in the left sigmoid sinus and jugular vein on MR images (4). Unlike the right brachiocephalic vein, which runs parallel to the ascending aorta, the left brachiocephalic vein is susceptible to compression between the sternum and elongated and tortuous aorta as a consequence of systemic hypertension or aging (5,16,17). Internal jugular valvular insufficiency or absence has also been considered a cause (18). Retrograde jugular flow has been confirmed by duplex ultrasonography and left-arm injection of contrast media on CT (19), but few studies have featured comparisons between findings on MRA and demonstration of jugular vein reflux among many participants. The supine position under which MRA and SPECT imaging were performed would affect the cause of jugular reflux flow, since the venous drainage system varies with postural changes (20,21). We assume that nuclear venography shows direct jugular reflux flow in the neck; meanwhile, brain MRA represents jugular venous flow fluctuations in the skull base propagating from cervical jugular reflux flow.
The RJV is often larger compared with the left jugular vein, so a siphoning effect might allow venous blood to drain into the right internal jugular vein through the transverse sinus and various anastomoses in the head (22,23). However, jugular venous reflux was observed on the right side in our study, probably as a result of differences in the side of predominant jugular outflow.
Several limitations must be considered when interpreting the results of this study. First, the frequency of right jugular venous reflux might be biased in this study, since injection was not performed via the right forearm on nuclear venography. Injection via both forearms would make the procedure unnecessarily invasive and at least some association of LJV reflux on MRA and nuclear venography has been demonstrated. Second, our initial motivation was to check the validity of nuclear venography as the gold standard for jugular venous reflux diagnosis; however, about half of the cases of jugular reflux were observed on a single modality only, partly because slight differences in the physical conditions of patients might exist, even though both MR and nuclear were performed within 1.5 h. The rate of injection of radionuclide and the position of head may also affect the appearance of jugular vein reflux. In addition, MRA and nuclear venography did not cover the same field of view, therefore, the comparison of the length of jugular vein reflux may be inadequate for diagnosis of reflux. However, continuous jugular venous reflux may occur in patients with jugular reflux on both imaging modalities. Third, positive jugular reflux on nuclear venography never reached the intracranial region, partly because the injected volume was relatively small (around 22 mL) and reflux might have been pulsatile. Lastly, the clinical significance of jugular vein reflux is debatable. Jugular venous reflux has been associated with transient global amnesia (TGA) (24,25) and transient monocular blindness (TMB) (23). Increased venous pressure leading to hippocampal venous congestion and ischemia may contribute to the etiology of TGA, as shown by a Valsalva maneuver preceding TGA in a substantial number of patients. However, recent reports suggest no relationship between jugular vein reflux and TGA, which may support that there are no patients with TGA in this study (26). Patients with TMB showed an increased incidence of venous reflux in the jugular and superior ophthalmic veins compared with control participants. Disturbance of cerebral venous outflow could be involved in TMB attacks or could at least render retinal perfusion more vulnerable to systemic hemodynamic challenges (23).
In conclusion, jugular venous reflux was observed mostly on the left side and half of the cases of retrograde flow were observed on both MRA and nuclear venography, with the rest apparent only on one modality.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI Grant Number 25461815.