
Abstract
Background
As the choice of treatment in patients with cervical carcinoma depends on cancer stage at diagnosis, accurate staging is essential.
Purpose
To compare three different combinations of magnetic resonance (MR) sequences for preoperative staging.
Material and Methods
Fifty-seven consecutive patients with biopsy proven cervical carcinoma underwent MR imaging (MRI) staging followed by primary surgical treatment. Thirty-two of 57 patients had had a cone biopsy prior to MRI. Three MR pulse sequence combinations were retrospectively reviewed by two experienced radiologists. The first imaging protocol consisted of pre-contrast sagittal and transverse images (protocol A), the second protocol included additionally oblique high-resolution T2-weighted (T2W) MR images of the cervix (protocol A+B), and the third included also contrast-enhanced sequences (protocol A+B+C). The imaging findings in the three steps (A, A+B, A+B+C) were recorded. The TNM stage was used for comparison between preoperative imaging and histopathology. Histopathology, together with surgical findings, served as gold standard.
Results
In 4/57 (7%) patients, the MR assessment of tumor stage (mrT) was altered when oblique sequences were added to the standard two plane imaging protocol (A+B). The mrT stage was altered in 1/57 (2%) patient when contrast-enhanced sequences were added to standard and oblique sequences (protocol A+B+C). The correlation between visible tumor on MRI and presence of tumor in the resected specimen did not change by adding oblique or contrast-enhanced images.
Conclusion
It is not necessary to perform oblique and contrast-enhanced sequences in small cervical carcinomas, i.e. without parametrial invasion. To avoid erroneous interpretation, information on previous cone biopsy is essential.
Introduction
Cervical carcinoma (CC) is the third most common malignancy in women globally (1). Approximately 450 new cases are diagnosed in Sweden every year and the disease often affects the young (2). The choice of treatment depends on the cancer stage at diagnosis. Consequently, accurate staging is essential for optimal treatment. In developing countries, surgery is not common as almost 80% of the patients are diagnosed at an advanced stage (3). Only tumors confined to the cervix, i.e. International Federation of Gynecology and Obstetrics (FIGO) stage IB1 or less, are treated surgically. Because CC is common in countries with limited radiological resources, staging is still performed by clinical examination in order to compare results globally, rather than based on scientific rationale (4,5). The clinical staging is assessed according to the FIGO staging system (5). Despite this, clinical staging in CC has several integral limitations. It does not take into account the cranio-caudal length of the tumor, which is one important prognostic factor (6), and also disregards the most important prognostic factor—the lymph node status (7,8). Clinical staging underestimates the spread of CC in up to 32% of cases with stage IB disease and in 44–67% of those with stage II–IV (9). The accuracy of clinical staging was shown to decrease from 79% to 53% when only patients with surgical stage above IIA were included (10).
The FIGO staging system was revised in 2009 (11) with only minor amendments for CC. Thus, the use of diagnostic imaging techniques to assess the size of the primary tumor is currently encouraged, but is not mandatory (11). Where magnetic resonance imaging (MRI) is available, tumor volume and parametrial invasion (PMI) should be recorded. Already in 2005 there was a substantial body of evidence establishing the role of MRI in the management of CC, both as an integral part in staging the primary tumor, monitoring response to treatment, detecting recurrence, and in radiotherapy planning (12). With MRI, 86% staging accuracy has been reported for CC stage IIB or higher compared to 47–66% for clinical staging, decreasing from 78% (stage I) to 23% (stage III) (13,14). The sensitivity for detecting PMI on MRI is reported to be 74% (range, 68–79%) (13). When an intact stromal ring around the cervix is appreciated on MRI, a 94–100% negative predictive value of PMI can be achieved (7,12,15,16).
The female imaging subcommittee of the European Society of Urogenital Radiology (ESUR) has published a consensus document on how to perform MRI in CC (17). The ESUR group states that the essential pretreatment protocol must include a combination of at least two T2-weighted (T2W) sequences obtained in the sagittal and oblique planes (perpendicular to the cervical canal) and T1-weighted (T1W) sequences of the upper abdomen and pelvis. Besides this consensus, there are few investigations on how MRI should be performed and, in particular, which MR pulse sequences should be used in the initial staging. In this study, our aim was to assess the diagnostic value of three different combinations of MR sequences in the pretreatment imaging protocol, in a selected group of patients intended for primary surgical treatment of CC. Our hypothesis was that in this group of patients, a more dedicated protocol may be used, possibly obviating the need for oblique and/or contrast-enhanced sequences.
Material and Methods
Approval for this study was obtained by the Ethical Review Board at the Karolinska Institute, Stockholm, Sweden.
Study population
Three hundred and forty-five consecutive patients with biopsy verified CC diagnosed during a 4-year period (2003–2006) at the Department of Gynecological Oncology, Karolinska University Hospital, Stockholm, were retrospectively identified. Among these patients, 251 had undergone MRI at our department prior to treatment. Patients with non-surgical treatment (n = 135), brachytherapy prior to surgery (n = 52), insufficient imaging (n = 5, including both motion/bowel artifacts and deviating imaging protocol) were excluded. One patient received chemotherapy 10 days prior to surgery because of a rapidly growing tumor (n = 1) and one patient had external radiation therapy without effect on the tumor (n = 1) and were hence also excluded (Fig. 1).
Flow chart resulting in the final study group comprising 57 patients (hysterectomy n = 51, trachelectomy n = 6). The gray boxes represent the excluded patients and reasons for exclusion. RT, radiotherapy.
The remaining study group comprised 57 patients with a median age of 39 years (age range, 27–63 years). There were two subgroups; 32 patients who had undergone cone biopsy prior to MRI and 25 women who had not.
Clinical FIGO staging
Staging of CC included gynecological examination during anesthesia for assessment of local spread, cystoscopy for bladder involvement, MRI of the pelvis and abdomen and chest X-ray. Stage IA1 and IA2 tumors were diagnosed only by microscopy. Depending on clinical logistics, the examination during anesthesia was performed before or after MRI.
Magnetic resonance imaging
MRI was performed median 20 days (range, 1–97 days) prior to surgery using a 1.5 T system (Philips Intera, Medical Systems, Best, The Netherlands). Examination of the pelvis was performed with a phased array body coil and the upper abdomen with the body coil (Table 1). T2W sagittal, trans-axial, and T1W trans-axial sequences of the pelvis, together with trans-axial T2W and fat-suppressed T1W sequences from the diaphragm to the promontory defined the first part of the MRI, protocol A (Fig. 2). The second part of the protocol included T2W sequences of the pelvis in an oblique axial plane perpendicular to the tumor/cervix, and in an oblique coronal plane along the longitudinal axis of the tumor/cervix, protocol B (Fig. 3). The third part of the protocol included fat-suppressed T1W trans-axial images of the pelvis and the upper abdomen, protocol C (Fig. 4), both with intravenous gadolinium-chelate contrast agent, either Gadopentetic acid (Magnevist 469 mg/mL, 0.2 mL/kg bodyweight, Bayer AB, Solna, Sweden) or Gadoteric acid (Dotarem 279.3 mg/mL, 0.2 mL/kg bodyweight, Gothia Medical AB, Billdal, Sweden) (Table 1).
MR protocol A: T2W sagittal (a) and axial (b) images of the pelvis, T1W axial images of pelvis (c) and axial T2W images of the upper abdomen (d) and T1W images of the upper abdomen (e). A cervical tumor bulging into the left fornix is marked with “X.” MR protocol B: T2W axial oblique images perpendicular to the cervical canal (a) and coronal oblique images parallel to the cervical canal (b). A cervical tumor bulging into the left fornix is marked with “X.” MR protocol C: T1W contrast-enhanced axial images of the pelvis (a) and the upper abdomen (b). A cervical tumor bulging into the left fornix is marked with “X.” MR pulse sequence parameters.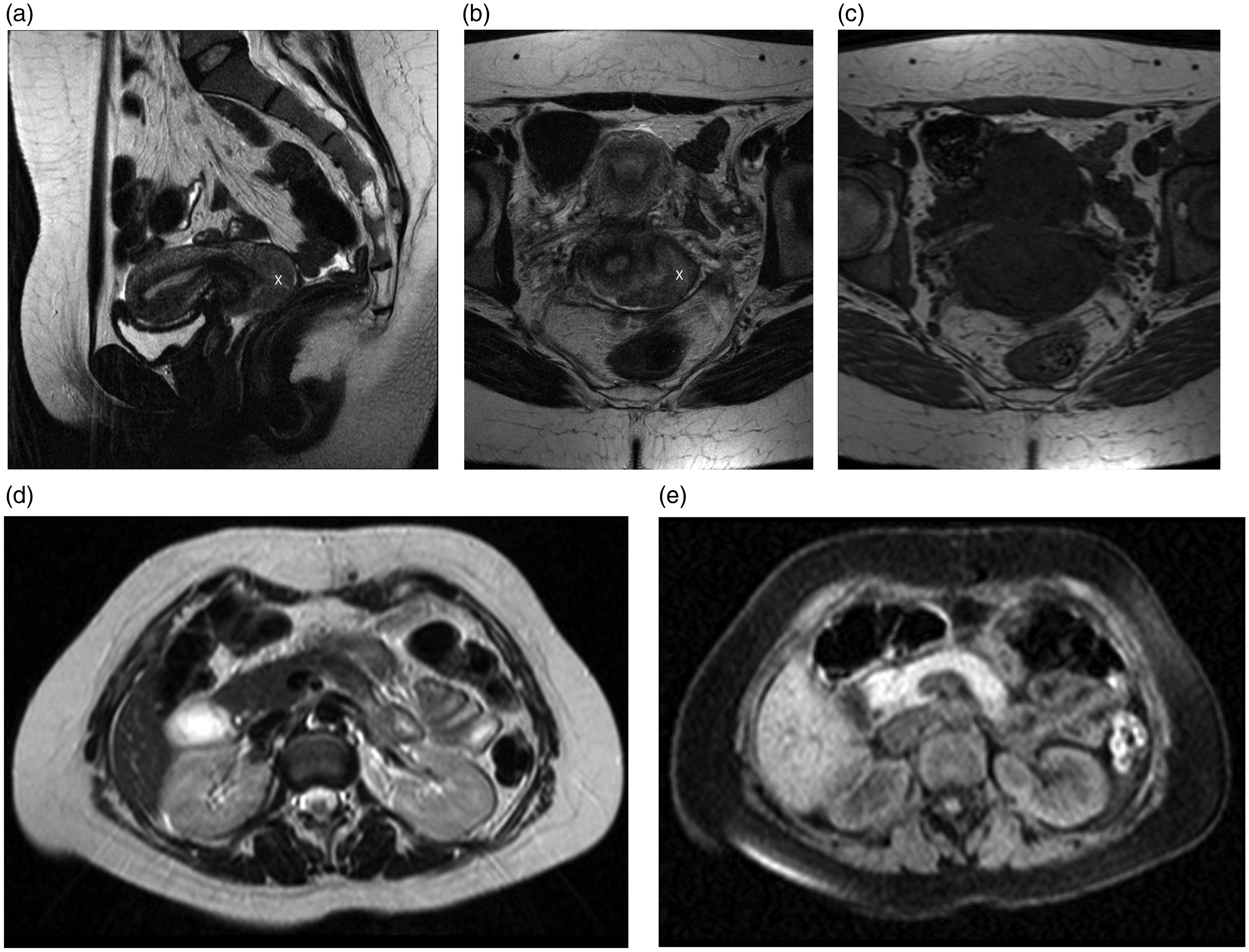



Surgery
All patients had surgery performed by experienced gynecological surgeons who were aware of the MRI findings prior to surgery. All patients received prophylactic antibiotics and underwent surgery with the same technique. Pelvic lymphadenectomy was performed systematically with dissection of six regions (both common iliac arteries, both external iliac arteries, and both internal iliac/obturator arteries). Hysterectomy was performed in 51 patients and six underwent trachelectomy, one of the latter patients refused to undergo surgical removal of pelvic lymph nodes.
Pathology
Thin sections from the surgical specimen were stained with hematoxylin and eosin (H&E) and were examined by an experienced pathologist. The original histopathology report, together with surgical findings, served as gold standard and was compared to the results of MRI and the clinically assessed FIGO stage.
Retrospective image analysis
Two radiologists (LB and BS) with 15 and 8 years of experience, respectively, in pelvic MRI, individually and then in consensus retrospectively reviewed the MR examinations according to a standardized protocol. The radiologists were blinded for all clinical information except the CC diagnosis.
According to this MR reviewing protocol, the radiologists were first presented with pre-contrast sagittal and transverse images (protocol A) and recorded presence of tumor, size in three orthogonal planes, involvement of cervical stroma (none, partially, or complete), distance to internal cervical os, presence of parametrial invasion, suspicious malignant lymph nodes including site (common iliac sin or dx, external iliac sin or dx, internal iliac/obturator sin or dx), presence of hydronephrosis, and defined a radiologic TNM and MR-FIGO stage. Presence of inhomogeneous signal on T2W images, as well as irregular contour of the lymph nodes, was considered as criteria for metastatic involvement. The size of any suspected metastatic lymph nodes was also recorded. The TNM stage was used for comparison between the preoperative imaging and histopathology, both regarding the primary tumor (T) and lymph node metastases (N).
Second, the radiologists were presented with the oblique high-resolution T2W MR images of the cervix (protocol A+B) and repeated the evaluation. The third step included reading of the contrast-enhanced sequences (protocol A+B+C). Changes in the assessment between the three evaluation steps (A, A+B, A+B+C) were recorded.
Statistical analysis
Descriptive statistics, including sensitivity and specificity, were calculated for the presence of tumor (T) and for the detection of lymph node metastases (N) as identified by MRI versus surgery and histopathology. The analysis was described separately for patients having performed cone biopsy prior to imaging and for those who had not. Inter-observer variation between readers, with respect to T and N staging, was assessed with Cohen's Kappa (Ƙ). Ƙ measurements were as follows: < 0 (no agreement), 0–0.2 (poor), 0.2–0.4 fair, 0.4–0.6 (moderate), 0.6–0.8 (good), > 0.8 (very good agreement).
Results
Patient characteristics
According to the clinical FIGO staging, the stage distribution was IA1 (n = 1), IA2 (n = 5), IB1 (n = 50), IB2 (n = 1). Adenocarcinoma was present in 22/57 patients (38.5%), squamous cell carcinoma in 31/57 (54%), small cell carcinoma in 2/57 patients (3.5%), glassy cell carcinoma in 1/57 (2%), and mucoepidermoid carcinoma in 1/57 patients (2%).
Staging by histopathology, clinical examination, and MRI according to the three pulse sequence combinations A, A+B, and A+B + C.

MR assessment of tumor stage (mrT)
Staging according to consensus by the two radiologists with the three different protocols (A, A+B, A+B+C) is presented in Table 2.
In 4/57 (7%) patients, the mrT stage was altered when oblique sequences were added to the standard two plane imaging protocol. Three patients were upstaged (T1b1 to T2b [n = 2], no visible tumor; T0 to T1b1 [n = 1]) and one was downstaged (T1b1 to T0 [n = 1]).
When contrast-enhanced sequences were added to standard and oblique sequences, 1/57 (2%) patient was upstaged (T0–T1B1). There were no changes in N or M stages among the three protocols, neither in consensus, nor in the individual evaluations.
The agreement between mrT stage with pathology (p)T stage was 37/57 (65%) for protocol A and protocol A+B+C. For protocol A+B, the agreement was 36/57 (63%).
MR assessment of lymph node metastases (mrN)
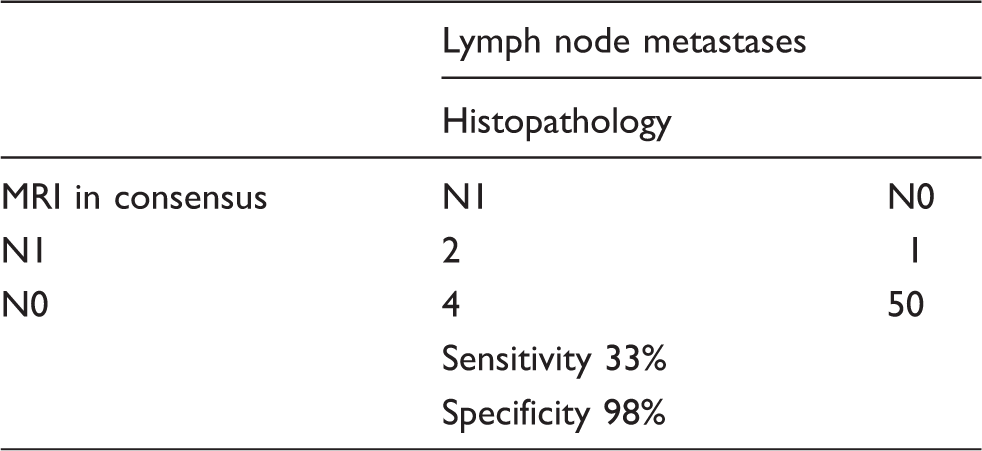
Lymph node staging: MRI versus surgical/histopathological findings.
Tumor visualization
Tumor detection by MRI in non-conizised versus conizised patients.

Non-conizised patients: In the subgroup of patients who did not undergo cone biopsy before MRI, the corresponding sensitivity and specificity in consensus read were 43% (9/21) and 100% (4/4), respectively (Table 4). Adding oblique images did not improve tumor detection. However, one more tumor was diagnosed by adding contrast-enhanced sequences.
Inter-observer agreement between MR readers: The Kappa agreement between the two readers for assessment of mrT stage with protocol A was 0.65, protocol A+B 0.62, and protocol A+B+C 0.65, respectively, corresponding to a good agreement using all three pulse sequence combinations.
For patients having performed cone biopsy prior to MRI, kappa for the inter-observer agreement for mrT stage, for protocol A, was 0.58 (moderate agreement), adding B gave Ƙ 0.61 (good agreement), and adding also C resulted in Ƙ 0.62 (good agreement).
Among those who had not undergone cone biopsy prior to surgery, inter-observer agreement for mrT stage was 0.69 (good agreement) for protocol A, 0.77 (good agreement) when adding B, and 0.78 (good agreement) when additionally adding C.
The Kappa values for agreement of N stage were 0.55 (moderate agreement) for all MR protocols.
Discussion
In the present study, we assessed the diagnostic value of three different combinations of MR sequences in order to see if it is possible to obviate oblique and/or contrast-enhanced sequences in patients intended for primary surgical treatment of CC.
The sensitivity or specificity for tumor visualization did not change by adding oblique or contrast-enhanced images. Nor was overall staging improved by adding oblique and contrast-enhanced sequences to a standard MR protocol comprising T2W and T1W sagittal and trans-axial pulse sequences. There were no changes in N or M stages among the three protocols, neither in consensus, nor in the individual evaluations.
To our knowledge, this is the first study assessing different combinations of MR pulse sequences for CC staging, and specifically the added value of oblique and contrast-enhanced sequences, respectively. All patients underwent MRI and surgery at the same center. MRI was evaluated by two experienced radiologists and the image findings were correlated to those of the original histopathology report and the surgical findings that served as the gold standard.
Despite the overall results, inter-observer agreement improved by adding oblique images to the standard protocol in patients not having performed cone biopsies prior to imaging. The agreement increased by adding oblique and contrast enhanced images. It was also the overall impression during the evaluations, that the additional pulse sequences increased the readers' diagnostic confidence. However, the contrast-enhanced sequences did not add information to justify its use, which is in agreement with the ESUR consensus group recommendations (17,18).
The sensitivity and specificity for detecting metastatic lymph nodes (N) was 33% and 98%, compared to previously published studies showing a sensitivity range of 27–60% and specificity approaching 95% (7,13,17–20). Although we found a high specificity for detection of lymph node metastases in consensus, the inter-observer agreement on N-stage was merely 0.55 (moderate agreement). Adding protocol B and/or C did not alter the mrN stage.
For patients without prior cone biopsy to MRI, the inter-observer agreement on tumor stage was generally good (K = 0.68–0.78). In patients having performed cone biopsies prior to MRI, agreement was moderate or close to good (K = 0.58–0.62). The sensitivity for detecting presence of tumor was higher among the conizised versus non-conizised patients (57% versus 43%), while the specificity was 94% versus 100%. This could be explained by falsely interpreting post-biopsy changes as small tumors. It has earlier been reported that it is not possible to differ small cervical tumors from artifacts appearing on MRI from post-biopsy changes (21).
There are some limitations with this study. The first is that only surgical patients were eligible in order to be able to compare the results with histopathology. Therefore, the study group is selected, comprising patients with small tumors, i.e. stages < IB2, since those with higher FIGO stage underwent non-surgical treatment. The added value of oblique sequences would be expected to increase in larger tumors with possible PMI. Another weakness is that the histopathological analysis was not reevaluated.
The ESUR recommendations on MR staging of cervical carcinoma state that two T2W sequences should be performed, one of which should be perpendicular to the cervical canal. This mostly corresponds to our protocol A+B, which also included a T2W sequence parallel to the uterine cervix. Diffusion-weighted imaging (DWI) sequences were not a part of our imaging protocol at the time when MRI was performed in the present patients. DWI is not regarded as mandatory by the ESUR consensus panel (17). However, the growing body of evidence regarding DWI for tumor imaging has increased considerably during the last few years, since the ESUR report was published, and currently DWI is included in most oncological MR protocols. Similarly, the contrast-enhanced dynamic MRI protocols have been developed since the present study patients were examined.
In conclusion, the above results suggest that it is not necessary to perform oblique and contrast-enhanced sequences when the tumor is small, i.e. unequivocally no PMI. Therefore, it would be possible to start every MR examination with protocol A and then evaluate if further examination with oblique and/or contrast-enhanced sequences are really necessary. When interpreting MRI, information on previous cone biopsy is essential in order to avoid erroneous interpretation.
Footnotes
Acknowledgments
We are grateful to Kristina Stenstedt for providing necessary clinical information through medical record review. We are also grateful to Elisabeth Berg for statistical consultation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was provided through the regional agreement on medical training and clinical research (ALF) between the Stockholm county council and the Karolinska Institutet.