
Abstract
Background
With the wider application of nephron-sparing surgery, there has been an increase in the occurrence of postoperative hemorrhage. However, despite such an increase, there are only a limited number of reports regarding renal artery embolization (RAE) for the management of postoperative bleeding after nephron-sparing surgery, especially after robot-assisted laparoscopic partial nephrectomy (RALPN).
Purpose
To evaluate the safety and clinical efficacy of transcatheter RAE for postoperative hemorrhage after open partial nephrectomy (OPN) and RALPN.
Material and Methods
A total of 29 patients (17 men, 12 women; age range, 31–70 years) who were referred to our hospital for postoperative hemorrhage after partial nephrectomy, between December 2003 and December 2014, were selected. We retrospectively reviewed patients’ clinical data, angiographic findings, embolization details, and clinical outcomes.
Results
Embolization was performed in patients who underwent OPN (25/29) and RALPN (4/29). The angiographic findings were as follows: renal artery pseudoaneurysm (n = 18), contrast extravasation (n = 8), and arteriovenous fistula (n = 3). Fiber-coated microcoil and n-butyl-2-cyanoacrylate (NBCA) was administered to the targeted bleeding renal arteries in 12 and 11 patients, respectively. In six patients, fiber-coated microcoil and NBCA were used concurrently. Technical and clinical successes were achieved in all patients (100%). Bleeding cessation was achieved in all patients, and no further relevant surgeries or interventions were required for hemorrhage control. There were no episodes of hemorrhagic recurrence during the follow-up period (median, 20 days; range, 7–108 days).
Conclusion
Angiography and RAE identified the origin of bleeding and could successfully preserve the residual renal function.
Introduction
Nephron-sparing surgery, also known as partial nephrectomy (PN), has been established as the standard treatment for renal masses as it preserves renal function (1–3). Recently, robot-assisted laparoscopic partial nephrectomy (RALPN) has been proposed as a viable alternative to open partial nephrectomy (OPN) as it offers a less invasive approach while providing comparable oncological outcomes and morbidity (4).
The benefit of PN, however, may be hampered by its newly discovered complications; PN is associated with serious vascular complications owing to the difficulty recognizing the vascular border and abundant renal vascularity (5). In particular, post-PN hematuria, such as renal artery pseudoaneurysm or arteriovenous fistula (AVF) formation, can lead to clinically significant blood loss (5–12). With the wider application of nephron-sparing surgery, i.e. OPN, conventional laparoscopic partial nephrectomy (LPN), and RALPN, there has been an increase in the occurrence of postoperative hemorrhage.
Renal artery embolization (RAE) has been reported to be an effective, minimally invasive treatment option for controlling post-PN hemorrhage (7,12–14). However, there are only a limited number of reports regarding the safety and efficacy of RAE for the management of postoperative bleeding after laparoscopic PN, especially RALPN. Hence, the purpose of this study was to investigate the incidence of postoperative hemorrhage that require RAE and to evaluate the clinical feasibility of embolization after OPN and RALPN.
Material and Methods
Patient characteristics
This study was approved by the institutional review board of Seoul National University Bundang Hospital (IRB No.: B-1501-284-112), and informed consent was waived due to the retrospective nature of this study. An electronic medical record (EMR) review was performed on 29 consecutive patients (17 men: mean age, 50.3 years ± 12.8; age range, 31–70 years; 12 women: mean age, 49.0 years ± 12.4; age range, 31–69 years). These patients were referred to our hospital for post-PN hemorrhage and required RAE between December 2003 and December 2014. EMR and computed tomography (CT) images were reviewed to determine the underlying etiology, clinical presentation, and outcome after embolization.
Interventional procedures
All angiographic procedures were performed by one of three board-certified radiologists with 6, 9, and 11 years of clinical experience performing endovascular therapy. Transarterial catheterization, using a trans-femoral approach in accordance with the Seldinger technique (15), was employed in all cases. Digital subtraction angiography covering the abdominal aorta was performed using a 5-Fr pigtail catheter; the tip was located at the suprarenal aorta, and a flow rate of 15 mL/s was maintained during a 2-s injection and a frame rate of three frames/s was sustained at the anteroposterior position in order to outline the renal arterial anatomy and to show the bleeding sites. Selective cannulation of the renal arteries, renal capsular arteries, or lumbar arteries was subsequently performed to identify the bleeding sites via a uniplanar angio suite (Philips Allura FD 20, Best, The Netherlands) using 5-Fr angiographic catheters (Cobra catheter and RH catheter). The following findings were pathologic indicators: pseudoaneurysm, AVF, and extravasation of the contrast agent. All pathologic renal arterial branches or renal capsular or lumbar arteries were embolized. Microcatheters with a tip of 2.0-Fr (Progreat; Terumo, Tokyo, Japan) or 2.4-Fr (Renegade; Boston Scientific, Natick, MA, USA) were introduced coaxially and advanced as distal as possible in efforts to preserve renal function. The choice between two routinely used embolic materials, n-butyl-2-cyanoacrylate (NBCA) (Histoacryl; B. Braun, Melsungen, Germany) and fiber-coated microcoils (Tornado; Cook Medical Technologies, Bloomington, IN, USA), was at the discretion of the attending interventional radiologists.
In the case of NBCA embolization, NBCA was mixed with iodized oil (Lipiodol Ultra Fluide; Guerbet, Roissy, France) at a ratio of 1:2 to 1:4. After flushing the microcatheter with 5% dextrose solution in efforts to avoid gluing and occlusion of the lumen during injection of NBCA, 0.5–2 mL of the mixture was carefully injected under fluoroscopic monitoring. The ratio, volume, and injection rate were based on the size and flow of the targeted vessel. To avoid adhesion of the catheter tip to the vessel wall, the microcatheter was quickly retracted after injection. Thereafter, a new microcatheter was used for subsequent embolization of the remaining pathologic arteries. In patients with fiber-coated microcoils embolization, pathologic arteries were approached by 0.018-in. microguidewires and 2.4-Fr microcatheters. The size of fiber-coated microcoils was selected to match the diameter of the embolized segment. Then, by using deployed fiber-coated microcoils, the vessel was trapped until occlusion. Completion renal arteriography and abdominal aortography were performed in all patients after embolization to ensure hemorrhage cessation and total occlusion of the target arteries.
Technical and clinical success assessment
Technical success was defined as complete occlusion of the target vessel. The main renal artery was stated as the first-order renal artery and its branches were ordered in a sequential manner. The order of an accessory or early branching renal artery was considered compatible to the same sized renal artery. If the order of renal artery cannot be determined, the three interventional radiologists came to a consensus based on the diameter of the renal artery and the area of perfusion territory.
Clinical success was defined as complete resolution of symptoms without the need for further intervention or surgical procedure within 7 days from RAE. Patients visited the outpatient clinic after 1 week from discharge, and every 1–3 months thereafter for follow-up of the underlying condition and recurrent hematuria. Patients were encouraged to visit the emergency department if hematuria or flank pain recurred; and in such event, a treatment option—repeated embolization or surgery—was determined via a multidisciplinary approach between the emergency physician, interventional radiologist, and urologist. The follow-up period was defined as the duration until the last hospital visit or date of death.
Complications
EMRs were reviewed to identify immediate complications after RAE. Delayed complication was defined as hemorrhage, as confirmed by CT scan, in the retroperitoneal or peritoneal cavity occurring more than 1 week after RAE with new symptoms, such as pain, syncope, marked hematuria, decreased blood pressure, and decreased hemoglobin concentration, which indicated blood transfusion and readmission to the ward. Delayed complications were assessed during the outpatient or emergency department visits. Furthermore, follow-up CT scans and EMRs were reviewed by three interventional radiologists to identify any signs of renal segmental parenchymal atrophy, renal ischemia or infarction, and abnormal fluid collection or abscess in the perirenal space. Complications that required extended hospitalization, advanced level of care, or one that resulted in permanent adverse sequelae or death were classified as major complications (16); other complications were considered minor.
Results
Patient baseline characteristics
Patient characteristics.
Data are number of patients and data in parenthesis are percentages except where indicated.
Data are mean ± standard deviation and data in parenthesis are range.
Postoperative RAE was performed based on the following indications: persistent hematuria (n = 16), bleeding via surgical drain tube (n = 6), sudden abdominal or flank pain (n = 4), or hemodynamic instability refractory to conservative treatment (n = 3). All patients had signs of hypotension (<100/60 mmHg) and tachycardia (>100 bpm). The hemoglobin level at the time of RAE was in the range of 6.5–12.9 g/dL, with the mean of 10.0 g/dL (normal range [M: 14.0–17.5 g/dL; F: 12.3–15.3 g/dL]). Transfusion of blood products before and after the procedure was performed in all patients, which varied from two to five packs of red blood cells.
In 21 cases, patients underwent CT scan prior to embolization, in which 19 cases were with the use of contrast agents. Among these 19 cases, 16 cases revealed culprit lesions: pseudoaneurysm (Fig. 1a) in 12 cases and contrast leakage in four cases. The remaining three cases failed to show the source of bleeding: perirenal hematoma without evidence of active bleeding (Figs. 2a and 3a) in two cases and unremarkable findings in one case. Two patients without contrast enhancement indicated perirenal hematoma, but it was unclear whether it represented active bleeding or postoperative finding.
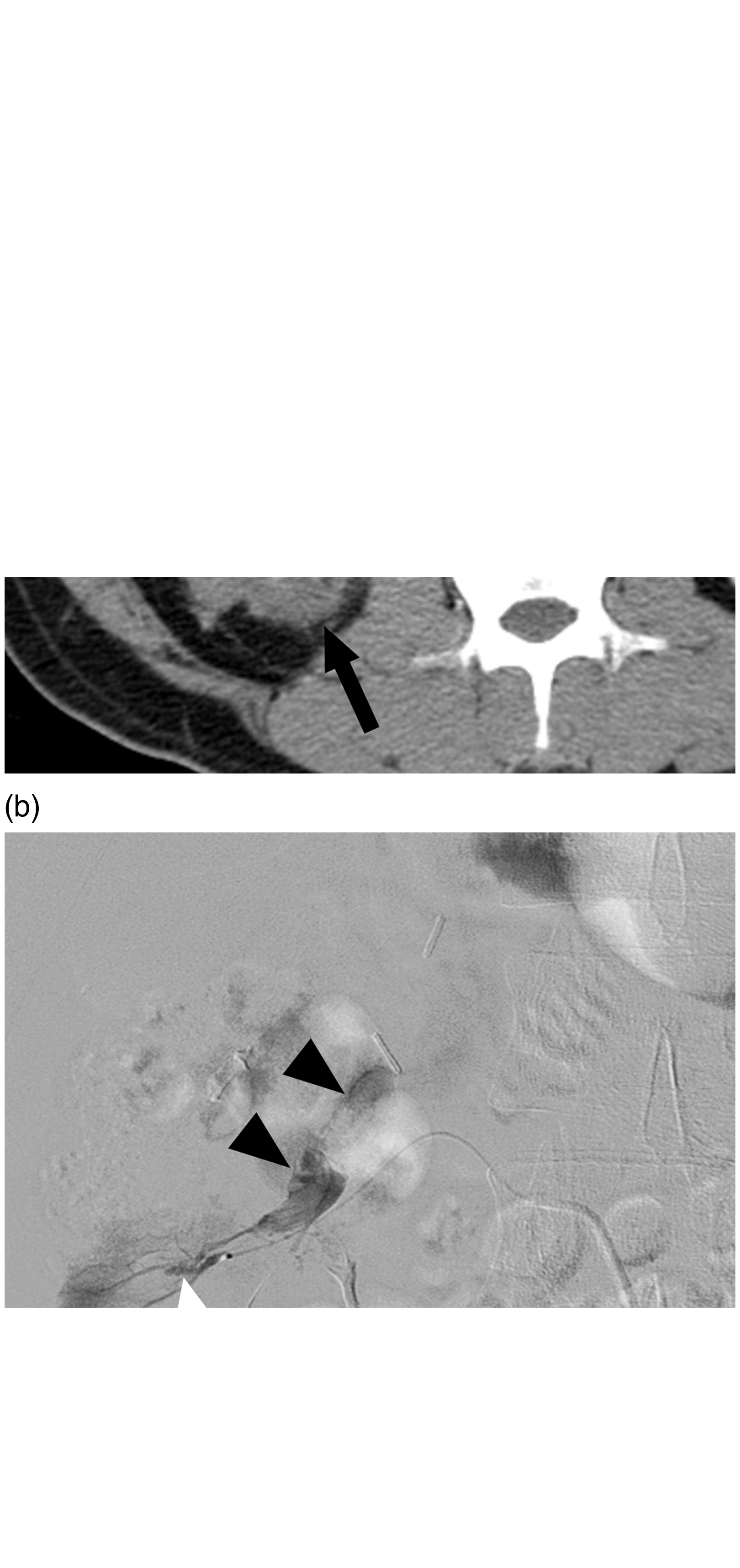
A 69-year-old male patient (5 days after OPN for RCC) presented with abrupt flank pain, fresh bloody surgical drains, and decrease of hemoglobin from 10.2 to 8.7 g/dL. (a) Contrast-enhanced CT scan coronal image: pseudoaneurysm (arrow) in the upper part of the right kidney with perirenal hematoma. (b) Selective angiography of the right renal artery: two pseudoaneurysms (arrowheads) from different renal segmental arteries. (c) Successful embolization of a small size pseudoaneurysm using pushable microcoil (3 mm × 1 ea), and a larger pseudoaneurysm using NBCA mixed with iodized oil was performed. Completion renal arteriography showed successful embolization with patent residual renal perfusion. A 38-year-old male patient (10 days after RALPN for RCC) presented with gross hematuria. (a) Contrast-enhanced CT scan axial image: no active arterial bleeding focus such as contrast leakage or pseudoaneurysm, but a minor adjacent hematoma (arrow). (b) Selective angiography of the right renal segmental artery via microcatheter with a tip of 2.0-Fr: direct visualization of the renal vein (arrowhead) via AVF (white arrow), and selective embolization with microcoil (3 mm × 1 ea) was performed. A 43-year-old male patient (20 h after OPN for RCC) presented with sudden flank pain and abrupt decrease of hemoglobin from 13.3 g/dL to 10.7 g/dL for 5 h. (a) Contrast-enhanced CT scan axial image: a minor perirenal hematoma (black arrow) and a moderate pararenal hematoma (white arrow) without any active arterial bleeding focus. (b) Selective angiography of the left renal capsular artery (arrow head) via microcatheter with a tip of 2.0-Fr: contrast leakage from renal capsular artery, and embolization with microcoil (3 mm × 1 ea) was performed.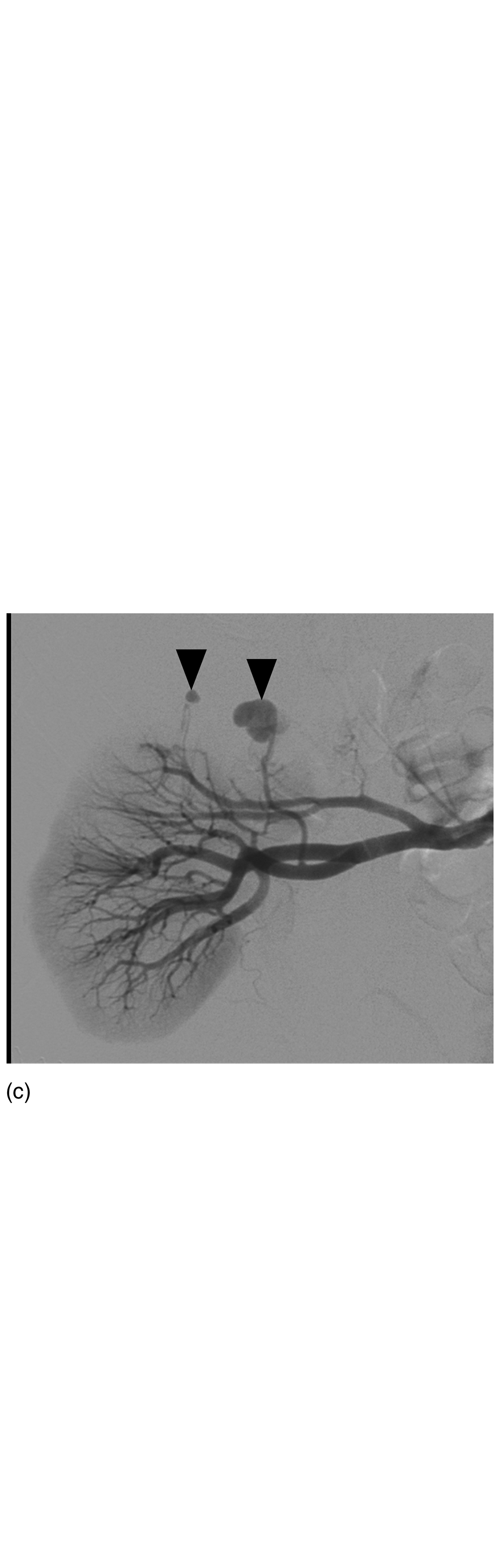

Characteristics of embolization and technical outcomes
Details of angiographic findings and embolization techniques.

Data are number of patients and data in parenthesis are percentages except where indicated.
Data are mean ± standard deviation and data in parenthesis are range.
Excluded one patient who underwent embolization of renal capsular artery.
Technical success was achieved in all patients (100%), as confirmed by completion renal arteriography and abdominal aortography, which showed total occlusion of the target bleeding arteries. A total of 40 arteries in 29 patients were embolized: 39 renal arteries (25 right, 14 left) and one renal capsular artery. Embolized renal arteries consisted of 12 third-order renal arteries (31%), 23 fourth-order renal arteries (59%), and four fifth-order renal arteries (10%); there were no main or second-order renal arteries involved in vascular complications. Either fiber-coated microcoils (n = 12) or NBCA mixed with iodized oil (n = 11) was administered to the targeted bleeding renal arteries with pseudoaneurysm formation, contrast extravasation, or feeders of AVF. In six patients, fiber-coated microcoils and NBCA mixed with iodized oil were used concurrently (Fig. 1c).
Clinical outcome
Clinical success was achieved in all patients (100%) with successful bleeding control and symptomatic improvement of hematuria, abdominal pain, and hemodynamic instability. No patient underwent repeated sessions of RAE or an operation for uncontrolled hematuria. Anemia in all patients was relieved with a significant rise of hemoglobin level after embolization. The median follow-up was 20 days (range, 7–108 days) without any episodes of hemorrhage or flank pain in any patient.
Complications
There were no procedure-related deaths or major procedure-related complications in accordance with the Society for Interventional Radiology complication category (16). Early minor complications were observed in 55% (16 of 29) of patients: 28% with abdominal or flank discomfort (8 of 29), 14% with nausea and vomiting (4 of 29), 7% with urticaria (2 of 29), 3% with fever (1 of 29), and another 3% with puncture site hematoma (1 of 29). Abdominal or flank symptoms and urticaria were resolved spontaneously or with analgesics and antihistamines. Blood culture was negative for microorganisms in the patient with fever, who improved after taking both antipyretics and empirical antibiotics. Puncture site hematoma was resolved within 1–2 hours with manual compression. No delayed complications were identified.
Discussion
In this retrospective study, transcatheter RAE as a treatment for postoperative hemorrhage after OPN and RALPN was both technically and clinically successful in all patients. No further relevant surgical interventions or repetitive embolization procedures were necessary. These results are in line with previous studies (13,14,17,18) and demonstrate RAE to be a safe and effective procedure by showing its high rate of efficacy (95%) and lack of embolization-related complications (19). Hence, transcatheter RAE should be considered as a treatment option for postoperative hemorrhage after PN. Furthermore, RAE is also associated with minimal morbidity, lower hospital costs, and nephron preservation, while avoiding further re-operative surgical intervention, with a risk of completion radical nephrectomy; additionally, it usually provides definitive therapy (20,21).
Inci et al. reported that of the 25 patients who underwent conventional LPN, one patient developed a loss of kidney function after two sessions of embolization (22). Accordingly, highly selective embolization of the renal artery branches in patients with postoperative bleeding is very important to preserve residual renal function. Catheterization of the third–fifth order renal artery and selective embolization is possible, allowing improved precision in accessing the bleeding locations; thus, avoiding surrounding parenchymal damage (23). Although the exact evaluation of the embolized volume was not possible, this could be estimated based on the order of embolized branch of the renal artery. A highly selective (third–fifth order) renal arterial embolization in this study preserve residual renal volume and minimize damage to the surrounding normal parenchyma (theoretically, less than 1/25–1/23 of the total renal volume).
The occurrence of postoperative vascular complications has been reported in 0.4% of patients after OPN and up to 4.9% after conventional LPN (10,18,20,21). Benway et al. reported that 1.7% (3 of 173) of patients after RALPN had renal artery pseudoaneurysms that required embolization (4). In our study, 4% of patients (29 of 775) had postoperative hemorrhage, following either OPN (25/452, 6%) or RALPN (4/323, 1%). Interestingly, hemorrhagic complication rates were lower in RALPN compared with the previously published data on conventional LPN (10,22,24–26).
A few studies have suggested a contrast-enhanced CT angiography for an accurate diagnosis of vascular pathology after invasive kidney surgery (8,10,27). In this study, however, active bleeding foci, such as contrast leakage or pseudoaneurysm formation in the PN site on the catheter-directed angiography, was not demonstrated by contrast-enhanced CT angiography in three patients (3/19, 16%). Therefore, catheter-directed angiography is indicated in patients with persistent need of transfusions or hemodynamic instability in spite of false-negative CT images. A catheter-directed renal angiography provides accurate identification of the specific bleeding source and successful treatment.
In this study, one patient who had a perirenal hematoma was subsequently treated by embolization for pseudoaneurysm of the renal capsular artery (Fig. 3b). Therefore, when a retroperitoneal hematoma or any other bleeding focus is observed at the extrarenal site in patients who undergo PN, an angiographic evaluation of extrarenal arteries as well as renal arteries, i.e. renal capsular arteries, lumbar arteries, or intercostal arteries, should be considered.
There are some limitations to this study. It was conducted retrospectively in a single institution, limiting the generalizability of the results. Further prospective randomized studies are warranted.
In conclusion, RAE is recommended to patients with post-OPN or post-RALPN hemorrhage because catheter-directed angiography can identify the origin of the bleeding and successfully provide minimally invasive treatment, preserving the residual renal function without the need for re-operation.
Footnotes
Acknowledgements
The authors thank the Medical Research Collaborating Center at Seoul National University Bundang Hospital for statistical analyses.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by a grant of the Korean Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (HI14C2175), Seoul National University Bundang Hospital Research Fund (No. 14-2014-018).