
Abstract
Background
Atrial fibrillation (AF) may be the cause or sequela of left atrial abnormalities and variants.
Purpose
To determine the prevalence of left atrial (LA) abnormalities in AF patients compared to normal sinus rhythm (NSR) patients.
Material and Methods
We retrospectively reviewed 281 cardiac CT examinations from 2010 to 2012, excluding patients with prior pulmonary vein ablation, known coronary artery disease, prior coronary stent placement, or coronary artery bypass grafts. The first group consisted of 159 AF patients undergoing cardiac CT prior to pulmonary vein ablation and the second group consisted of 122 NSR patients evaluated with coronary CT angiography. Demographic data were collected. LA abnormalities were analyzed. Left atrial diameter was measured on an axial view.
Results
A total of 281 patients were included. The male gender has significantly higher prevalence of AF than female gender, P value <0.001. Patients with AF were significantly older (mean age, 57.4 years; standard deviation [SD], 11.8 years) than NSR patients (mean age, 53.4 years; SD, 13.6 years), P value, 0.01. The left atrial diameter was greater in the AF patients (mean diameter, 4.3 cm; SD, 0.82 cm) versus the NSR patients (3.4 cm; SD, 0.58 cm), P value, <0.0001. LA diverticulum was the most prevalent variant, occurring in 28.4% of the entire patient population followed by LA pouch, occurring in 24%. There was no significant between group differences in the prevalence of these or the remainder of the LA variants.
Conclusion
AF patients differed significantly from NSR patients in LA size, gender, and mean age. There was no statistical significance between the two groups with regard to the LA morphologic abnormalities other than size.
Introduction
Atrial fibrillation (AF) is a common arrhythmic condition involving the left atrium that can result in or be caused by left atrial (LA) remodeling. This remodeling is associated with LA wall fibrosis and myocyte hypertrophy at microscopic level and in LA dilatation at the macroscopic level (1). The left atrium may also demonstrate a broad array of normal anatomic variants and minor anomalies. Our hypothesis is that due to atrial remodeling, patients with AF may have a higher prevalence of LA abnormalities than those with normal sinus rhythm. The purpose of this study was to determine the prevalence of LA abnormalities in AF patients compared to normal sinus rhythm (NSR) patients.
Material and Methods
Patient population
We retrospectively reviewed 281 cardiac CT examinations performed at a large university hospital. The patients were divided into two groups with the first group consisting of 169 patients prior to pulmonary vein ablation for AF between January 2010 and June 2012. The second group was composed of 122 patients evaluated for chest pain and did not have documented AF from October 2009 to June 2012. We excluded from the AF group patients with known prior pulmonary vein ablation. In total, 159 AF patients were included. We excluded from the NSR group patients with known coronary artery disease, prior coronary artery stent placement, or coronary artery bypass grafts in order to identify a cohort expected to have normal LA anatomy. A total of 122 NSR patients were included. In both groups, cases were excluded with suboptimal or incomplete examination techniques or known congenital heart disease. Informed consent was waived by the IRB.
CT techniques
Cardiac computed tomography (CT) was performed using the departmental standard protocols. For CT of the pulmonary vein, a retrospective technique was applied on a Philips Brilliance 64 Multidetector CT Scanner (Philips Medical Systems, Cleveland, OH, USA). We performed retrospective or prospective techniques on a Philips iCT 256 Multidetector CT Scanner (Philips Medical Systems) based on rhythm, when possible, for pulmonary vein evaluation. No premedication was given for heart rate control in this group. Intravenous contrast bolus track and trigger protocol was applied to optimize contrast enhancement in the pulmonary veins and left atrium. The region of interest (ROI) tracker was placed in the left atrium. Scan was performed from just above the aortic arch to the diaphragms. Images were reconstructed at 78% of the R-R interval. Three-dimensional (3D) images were created and stored on PACS for later evaluation.
Coronary CT angiography (CTA) protocol was tailored to each patient’s cardiac history. In all cases, the target heart rate was less than 60 bpm. Retrospective ECG gating technique was utilized on a Philips 64 Brilliance. Retrospective or prospective ECG gating technique was utilized on a Philips iCT 256 Multidetector CT Scanner (Philips Medical Systems) depending on indication and heart rate. A total of 5–25 mg intravenous Metoprolol was administered for heart rate control and two tablets (0.4 mg) sublingual Nitroglycerine for coronary artery vasodilation (if not contraindicated). ECG gated tube modulation was used to reduce radiation exposure when using retrospective ECG technique. The images were acquired 5–6 min after sublingual Nitroglycerine. Scanning technique, premedication, and the amount and rate of contrast injection were under radiologists’ supervision. For both groups, Isovue 370 was administered intravenously at a rate of 5 mL/s followed by saline flush also at 5 mL/s. The amount of contrast was calculated based on the scan time, post threshold trigger delay, and location of tracker trigger ROI. Image acquisition extended from the carina to the diaphragms.
The CT parameters were adjusted according to the patient’s conditions (heart rate, age, BMI), clinical indications, available CT scanners (64 - or 256-detector CT scanners), ECG gating technique, and reconstruction techniques. We used 100–150 kV, 100–1050 mAs, 0.9 mm thickness with 0.45 increment, and the fastest available rotation time (0.4 s on 64-detector scanners and 0.27 s on 256-detector scanners).
Parameters analyzed
Two radiologists reviewed the images retrospectively on a PACS workstation (Fuji Medical, Stamford, CT, USA) using the MPR software and reported by consensus (ST, SMR). The LA diameter and any anatomic variants were documented. LA variants included left atrial appendage (LAA) diverticulum, LA diverticulum, patent foramen ovale (PFO), interatrial septal aneurysm (IASA), lipomatous hypertrophy of interatrial septum (LHIS), left atrial pouch, atrial wall calcification, unroofed coronary sinus, and LA diameter. LA diameter was measured in its maximum anteroposterior (AP) dimension on the axial images.
Dichotomous variables such as gender, LAA diverticulum, LA diverticulum, LHIS, and LA pouch were analyzed by Pearson Chi-Square test, or when numbers of positive findings was small (PFO and atrial wall calcification) by Fisher’s exact test. Differences in patient age and LA size between the two groups were analyzed using ANOVA table.
Results
Results and details of statistical analysis of patients’ demographic data and LA abnormalities.
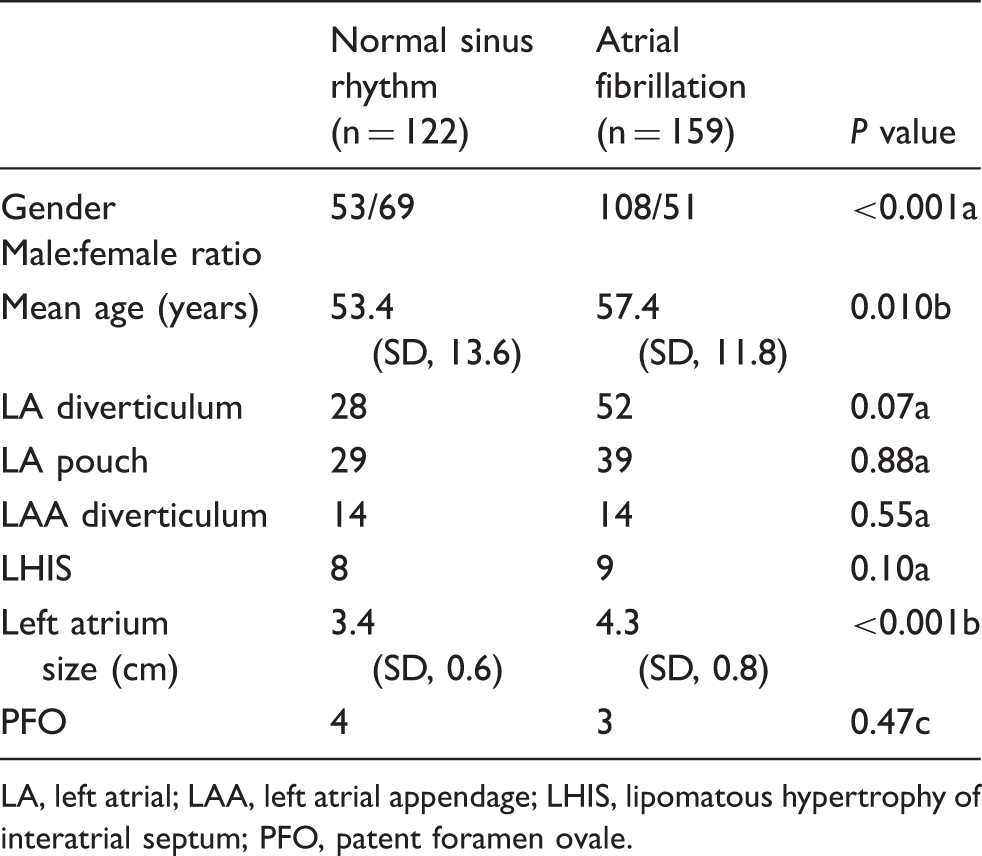
LA, left atrial; LAA, left atrial appendage; LHIS, lipomatous hypertrophy of interatrial septum; PFO, patent foramen ovale.
As expected, LA diameter was greater in the AF patients (mean diameter, 4.3 cm; SD, 0.8) versus in the NSR patients (mean diameter, 3.4 cm; SD, 0.6), P value <0.0001.
The prevalence of AF was significantly higher in our group of men compared to the group of women, P value <0.001.
No atrial septal aneurysm or unroofed coronary sinus was found in our series and LA wall calcification was seen in only a single patient. Other LA morphologic abnormalities were more common, the most prevalent being the LA diverticulum, present in 28.4% of the patients, followed by LA pouch (24%), and LAA diverticulum (10%).
There were no significant differences in the prevalence of LAA diverticulum, LA diverticulum, LHIS, LA pouch, PFO, or LA wall calcification between the AF and NSR groups. Post hoc power analysis showed a power of >0.8 for the detection of between group differences ≥15% for these relatively low prevalence anomalies.
Discussion
The only three factors found to be statistically significant between the two groups were mean age, gender, and LA diameter. Other than the expected greater LA diameter among AF patients, the comprehensive evaluation of the LA did not reveal the association of AF with other LA variants.
Although the AF patient group was older than the NSR group, our AF patients were still relatively younger than recently reported by Lloyd-Jones et al., with a mean age of 66.8 years for men and 74.6 years for women (2). This may be related to increasingly reported “Lone AF” in young adults in the past several years (3).
The mean age of patients in the NSR group was also lower than the age at which coronary artery disease commonly manifests, with men clinically manifesting at 50–65 years and women at 60–75 years (4), This was likely due to our group’s (radiology and cardiology service) active use of coronary CTA as a part of acute chest pain investigation. We encounter a considerable number of young patients who come to the hospital (clinic and emergency department) with chest pain, likely resulting in a selection bias towards younger patients in the NSR group.
Selection bias may explain the higher prevalence of AF in our male population compared our female population, possibly due to a greater number of male referrals for ablation therapy (n = 161 versus 120).
The remainder of LA variants in AF and NSR groups did not differ significantly. Overall prevalence of LA variants in our series was similar or relatively higher than previously published literature. Differences may reflect the variability among the study groups due to inhomogeneity of the imaging approaches, different patients’ conditions and sample sizes.
The correlation of LA diameter, volume, and function in heart disease and its impact on prognosis is receiving increased attention (5). The increased LA size among the AF patients is expected, over 25% of patients with AF having an AP LA diameter of greater than 4.5 cm (6). Although LA evaluation has been based primarily on echocardiogram, cardiac CT and magnetic resonance imaging technology have evolved, providing better anatomic details along with excellent spatial and temporal resolution and post-processing assessment of LA function. Cross-sectional and functional cardiac imaging is gaining more acceptance in evaluating LA anatomy and function.
CT measurement of LA diameter in turn, correlates well with other measures of LA size. LA AP diameter and axial LA area were well correlated with LA volume on non-ECG gated contrast-enhanced chest CT according to Mahabadi et al. (7). LA axial diameter was also well correlated with transthoracic echocardiogram (TTE) (8).
Based on the above studies, LA measurement was performed in the maximal AP diameter on axial plan (Fig. 1).
A 57-year-old-man with AF. Pulmonary vein CT from pre-ablation mapping shows measurement of the left atrium in AP diameter. The largest diameter in the AP dimension was chosen.
Although LA volume, function, and diameter can be normalized to body surface area (BSA), we did not include these factors in our calculations because BSA data were not available.
LAA and LA diverticulum have nearly an identical appearance. They appear as an outpouching of contrast from the left atrium or LA appendage. LAA diverticula are subdivided into neck and body and contain pectinate muscles which result in an irregular appearance (Fig. 2). The LA diverticulum is defined as a saclike structure with broad-based ostium and smooth body contour (9) (Fig. 3a and 3b).
A 56-year-old woman with AF. Pulmonary vein CT for pre-ablation mapping shows a small LA diverticulum with a pecinate muscle (arrow) continuing with the extension of LAA. A 46-year-old man with AF. Pulmonary vein CT for pre-ablation mapping shows a small LA diverticulum from the posterior wall of the left atrium (arrows) demonstrated on (a) coronal and (b) volume-rendered images.

The reported prevalence of LAA and LA diverticulum varies considerably among studies. The prevalence of LA diverticulum is in the range of 20–36% (9,10) and prevalence of LAA diverticulum is in the range of 8–23% (9,11).
The prevalence of LA diverticulum in our patients, 33% in AF patients and 23% in NSR patients, was similar to the recent studies by Troupis (12) and Lazaura (13) (23.5–40% in AF patients and 20.5–36% in NSR patients) but the prevalence of LAA diverticulum in our study (8.8% in AF group and 11% in NSR group) was slightly higher than reported by Lazoura (13) (6.5% in both AF and NSR groups). Although with a slight difference in the prevalence, no statistical significance of prevalence of LA and LAA diverticulum was demonstrated between AF and NSR patients in our series.
LA septal pouch is a recently reported entity and occurs from an incomplete closure of the foramen ovale, resulting in a pouch. The pouch may communicate with the right or left atrium. Overall prevalence of LA pouch in the autopsy series recently reported was 44% (14), compared to 24% in our study (Fig. 4a–c). Up to 90% of incompletely fused LA septal pouch showed communication with the left atrium while only 10% demonstrated continuation with the right atrium (14). LA communication is considered as a potential site of thrombus formation and subsequently thromboembolic events (15). There was no significant difference in prevalence of LA pouch between AF and NSR patients in our series.
A 66-year-old woman with AF. Pulmonary vein CT for pre-ablation mapping demonstrates a LA septal pouch at the fossa ovalis, a typical location (double arrows) in (a) axial, (b) coronal, and (c) sagittal views.
PFO is characterized by lack of fusion of the septum primum and septum secundum and presents as a potential right to left shunt (16) (Fig. 5a and 5b). This entity is commonly encountered in healthy individuals. The current gold standard to diagnose PFO is transesophageal echocardiogram (TEE) with air bubbles while the patient is preforming a Valsava maneuver (17). The prevalence varies among studies depending on the imaging modalities and patient population. The prevalence is as high as 25% on TEE (18) and 22.6% on cardiac CT (18,19). Investigators have used different imaging criteria to diagnose PFO. Williamson et al. created three CT criteria to establish PFO: (i) presence of LA septal pouch at the location of septum primum; (ii) visualization of the contrast column between septum primum and septum secundum; and (iii) visualization of the contrast jet from left atrium into the right atrium (20). By using visualization of contrast jet across the two atria (from the left atrium to the right atrium) as a stringent criterion, the prevalence is relatively low. Kim et al. found 2.1% in his series (21) while Purvis et al. found 4.6% (22).
A 45-year-old man with chest pain. Coronary CTA was performed to rule out coronary artery disease. A small jet of contrast from left atrium to right atrium, compatible with PFO, is seen on the axial plane (arrow in (a)) and on the sagittal plane (black dot in (b)). Note a slit-like opening of PFO on the sagittal plane (black arrow in (b)).
Our definition of PFO is similar to Kim et al. and we found that the prevalence of PFO in our series was relatively low, 2.5%. Since our diagnostic criteria are highly specific but moderately sensitive, some PFOs could have been missed.
We did not find a significant difference in prevalence of PFO between AF and NSR patients.
Normal septal fat thickness is in the range of 0.9–9.9 mm (23). The most common abnormality of the interatrial septum is lipomatous hypertrophy of the interatrial septum (LHIS), which is a fatty deposition within the interatrial septum more than 2 cm in thickness (24). The characteristic features include a smoothly marginated, non-enhancing dumbbell-shaped fatty mass that spares the fossa ovalis (25,26). The prevalence of LHIS varies from series to series, in the range of 1–8% (27,28). The prevalence in our study was 6% (Fig. 6). There was no significant difference in prevalence of LHIS between AF and NSR patients in our series.
A 59-year-old man with AF. Pulmonary vein CT for pre-ablation mapping shows a prominent fat deposition in the interatrial septum (arrow), corresponding to LHIS.
LA calcification or porcelain atrium is one of the rare cardiac conditions that is usually found as an incidental finding on imaging studies and related to longstanding rheumatic valve disease (29). LA calcification may have clinical implications for mitral valve surgery and is found in 2.1 % in patients undergoing valvular surgery. The sole LA calcification seen in our study may not have been caused directly by rheumatic valve disease. The patient with LA calcification had a history of mitral valve surgery 5 years before developing AF that required radiofrequency ablation. CT demonstrated a focal punctate calcification in the posterior wall that may have been related to the ablation sites.
Atrial septal aneurysm (ASA) is a rare entity and can be mistaken as a pseudo-mass on cardiac CT (30). It is defined as a redundant and mobile interatrial septum with significant bulging from the center greater than 10 mm (31). The prevalence of ASA reported in patients who underwent routine echocardiogram is 1.2% (32) and 6.1% on routine coronary CTA (22). We found no ASA cases in our population.
The coronary sinus (CS) receives deoxygenated blood from the anterior and posterior interventricular veins, the great cardiac vein, and the left marginal and posterior veins draining into the right atrium. Absence of a coronary sinus roof, unroofed coronary sinus, is a rare cardiac abnormality defined as a communication between the CS and the left atrium. This condition is considered an intracardiac shunt and may be associated with congenital cardiac anomalies, specifically, a persistent left superior vena cave (LSVC) (33). We found no unroofed CS in our population.
Although we did not specifically assess pulmonary venous anatomy in our study, prior literature suggests that pulmonary venous anatomy does not differ between the AF and NSR patients. In normal participants, the most common PV anatomy is two right and two left pulmonary vein ostia (60–70%) followed by two right ostia and a left common trunk (15%) (34).
According to Thorning et al., AF patients more commonly have variant right anatomy (82% with two ostia and 17% with three ostia) than variant left anatomy (91% with two ostia and 8.5% with three ostia). Overall, however, the most common pulmonary venous configuration was two right and two left venous ostia, similar to NSR patients (35).
Two radiologists worked in parallel to review the CT examinations, such that each image set was reviewed by only one radiologist therefore we are not able to provide the inter-rater variability.
Selection bias is an additional limitation of this study. Both AF and NSR patients in our population were younger than previously reported.
In conclusion, patients with AF demonstrated atrial remodeling, having larger LA diameters than patients with NSR, but did not demonstrate increased prevalence of other atrial abnormalities detectable on cardiac CT. Although the group size was not sufficiently sensitive to detect intergroup differences <15%, our data suggest that none of the LA abnormalities are strongly associated with AF. As a group, these abnormalities are unlikely to be caused by AF and are unlikely to have a clinically significant role in the initiation of AF.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.