
Abstract
Background
Iterative reconstruction can reduce image noise and thereby facilitate dose reduction.
Purpose
To evaluate qualitative and quantitative image quality for full dose and dose reduced head computed tomography (CT) protocols reconstructed using filtered back projection (FBP) and adaptive statistical iterative reconstruction (ASIR).
Material and Methods
Fourteen patients undergoing follow-up head CT were included. All patients underwent full dose (FD) exam and subsequent 15% dose reduced (DR) exam, reconstructed using FBP and 30% ASIR. Qualitative image quality was assessed using visual grading characteristics. Quantitative image quality was assessed using ROI measurements in cerebrospinal fluid (CSF), white matter, peripheral and central gray matter. Additionally, quantitative image quality was measured in Catphan and vendor’s water phantom.
Results
There was no significant difference in qualitative image quality between FD FBP and DR ASIR. Comparing same scan FBP versus ASIR, a noise reduction of 28.6% in CSF and between −3.7 and 3.5% in brain parenchyma was observed. Comparing FD FBP versus DR ASIR, a noise reduction of 25.7% in CSF, and −7.5 and 6.3% in brain parenchyma was observed. Image contrast increased in ASIR reconstructions. Contrast-to-noise ratio was improved in DR ASIR compared to FD FBP. In phantoms, noise reduction was in the range of 3 to 28% with image content.
Conclusion
There was no significant difference in qualitative image quality between full dose FBP and dose reduced ASIR. CNR improved in DR ASIR compared to FD FBP mostly due to increased contrast, not reduced noise. Therefore, we recommend using caution if reducing dose and applying ASIR to maintain image quality.
Keywords
Introduction
In computed tomography (CT), image quantum noise is inversely proportional to the square root of the radiation dose (1). Consequently, reconstruction techniques that yield less image noise could facilitate dose reduction. Adaptive statistical iterative reconstruction (ASIR) is a reconstruction technique that aims to reduce image noise compared to filtered back projection (FBP). It is accomplished by minimizing the sum of two terms: one cost function, which penalizes poor statistics due to image noise, and one regularization term (2). New research has indicated a much higher potential for radiation induced cataracts than previously assumed (3), thus dose reduction would be beneficial for head CT scans. Many studies have investigated implementation of ASIR in head CT using both phantoms (4–6) and patients (4,6–12), which show promising results.
A recent study has warned of a reduction in low contrast detectability in hypoattenuated regions of the brain after a stroke when using dose reduced protocols reconstructed using iterative reconstruction (13). Missing such subtle lesions could have serious consequences for the patients; therefore, dose reduction in head CT by applying iterative reconstruction needs thorough validation prior to implementation in the clinic.
The aim of this study was to evaluate quantitative and qualitative image quality for full dose (FD) and dose reduced (DR) head CT protocols reconstructed using FBP and ASIR in a patient population.
Material and Methods
Study population and imaging
This study was approved by the regional ethical committee and all participants gave written consent. A flowchart describing the patient inclusion is shown in Fig. 1. The median age was 73.5 years with an interquartile range (IQR) of 21.3 years (age range, 26–86 years). Fourteen patients (11 men, 3 women) undergoing a follow-up unenhanced CT examination were included: 11 patients received scans due to subdural hematoma, two due to control after ventricular shunt operation, and one due to re-implant of bone. All patients were their own controls and underwent an examination identical to the previous unenhanced head CT examination, except for a 15% decrease in mAs (335 to 285). The CT protocols used are shown in Table 1. This 15% dose reduction should theoretically result in an increase in quantum noise by 8.4%. The FD and DR protocols lead to average dose length products of 878 mGy∙cm, with a standard deviation (sd) of 34 (range, 771–900) and 748 mGy∙cm, with a sd of 39 (range, 656–765). The respective estimates of effective dose using a conversion factor of 0.0019 mSv/mGy∙cm (14) were 1.7 and 1.4 mSv. The average dose reduction was 14.8%, with a sd of 3.3 (range, 11.0–25.5) (P < 0.001). The median time between the standard and low dose examination was 47.5 days, with an IQR of 65.5 (range, 9–157).
Flowchart of patient inclusion criteria. Unenhanced CT protocols used.

Measurement of quantitative image quality
Quantitative image quality was evaluated in all four series: FD FBP and 30% ASIR (henceforth referred to as ASIR), and DR FBP and ASIR. Three slices in each series were evaluated, at the level of the thalamus, the corona radiate, and the centrum semiovale. The slices from the DR acquisitions, which visually best resembled the respective FD acquisitions were selected. The FBP and ASIR reconstructions of the same dose level were reconstructed from the same raw data.
In order to measure in comparable regions of interest (ROIs), the corresponding FD and DR slices were registered using Matlab (Mathworks, Natick, MA, USA). The registration allowed for translation, rotation, and scaling, and was verified visually.
The four images of the same slice were displayed side by side and a technician with 12 years of experience in neuroradiology (KLH) placed the ROIs. A Matlab script synchronized the position of the ROIs in all four series, thus all measurements had the same pixel coordinates. The ROIs were not placed in positions with obvious pathology and visual inspection verified that the ROIs were located in the same tissue in all four images. The area of each ROI was approximately 34 mm2. Mean CT number and noise (standard deviation) was measured for all ROIs. To avoid bias, all results were hidden from the technician.
For each series, a total of 34 ROIs were evaluated: 14 at the level of the thalamus, two ROIs in cerebrospinal fluid (CSF), four in white matter, four in peripheral gray matter, and four in central gray matter (Fig. 2a); 12 at the level of the corona radiata: four ROIs in each tissue (Fig. 2b), and eight at the level of the centrum semiovale: four ROIs in white matter and four in gray matter (Fig. 2c). The total number of ROIs was 1904.
Example of ROI positioning in the slice at the level of (a) thalamus, (b) centrum semiovale, (c) corona radiata.
Statistical analysis of quantitative image quality
In order to investigate ASIR’s effect on image quality without the confounders related to multiple acquisitions, we compared noise, CT numbers, and contrast-to-noise ratio (CNR) in FBP and ASIR reconstructions from the same raw data. CNR was calculated by subtracting the average CT number for each tissue and dividing by the mean noise for both tissues according to the equation in Fig. 3. FD and DR scan series with the same reconstruction technique were compared to investigate the presence of confounders related to multiple acquisitions. Finally, FD FBP and DR ASIR images were compared to evaluate the potential for dose reduction using ASIR. 95% confidence intervals (CI) for noise, CT numbers, and CNR were estimated by bootstrapping the respective ROIs 10,000 times using Matlab.
Formula for computing contrast to noise ratio between two tissues. n is the number of ROIs for the respective tissue. 
Phantom measurements
To compare phantom measurements to clinical results, the low contrast module (CTP515) of a Catphan 600 phantom (The Phantom Laboratory, Greenwich, NY, USA) and the vendors’ water phantom were scanned using the DR protocol (Table 1) and reconstructed using FBP and ASIR. Noise measurements for both reconstruction techniques were performed. In Catphan, noise was measured in each of the three largest Supra-slice objects with 1.0%, 0.5%, and 0.5% contrast, respectively (15), with a ROI of approximately 83 mm2. Additionally, background noise was measured in the center of Catphan with a ROI of approximately 400 mm2. In the water phantom, noise was measured in a ROI covering 40% of the phantom area.
Visualization of noise and contrast changes
To visualize changes in noise and contrast between FBP and ASIR reconstructions, the ASIR reconstruction for a clinical, Catphan, and water phantom image were subtracted from the corresponding FBP reconstruction (Fig. 4). The resulting image shows visually where the reconstruction techniques differ. Noisy appearance of certain tissues in the difference image indicates noise difference between reconstructions. In areas where the subtraction image is dark, the CT numbers in the ASIR reconstruction are higher than the FBP reconstruction and vice versa, which shows the changes in contrast visually.
Montage of clinical, Catphan, and vendors’ water phantom images reconstructed using FBP and 30% ASIR, along with a difference image between the two reconstruction types. For the FBP and ASIR reconstructions, the window level was 40 for the head CT and Catphan phantom, and 0 for the water phantom. The window width was 80. For all difference images the window level was 0 and the window width 10.
Qualitative image quality
Quality assessment and scoring scale.
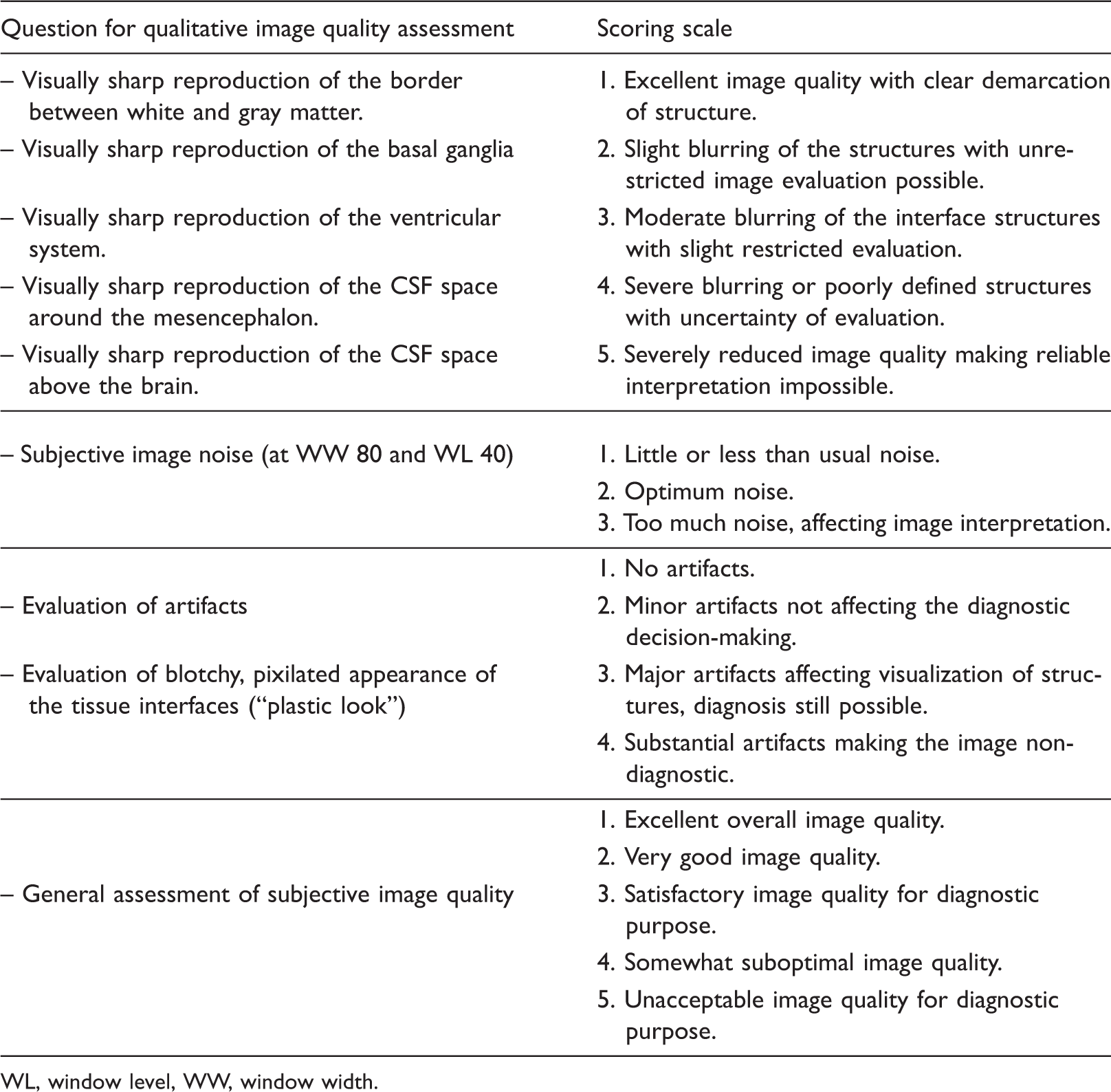
WL, window level, WW, window width.
Results
Same scan comparison of FBP and ASIR
Mean noise reduction and CT number difference between FBP and ASIR reconstructions of the same scan.


Quantitative image analysis of noise and CT numbers. (a) Comparison of image noise in identically positioned ROIs between FBP and ASIR for image reconstructions based on the same raw data. (b) Comparison CT numbers in identically positioned ROIs between FBP and ASIR for image reconstruction based on the same raw data. (c) Comparison of image noise in co-registered ROIs between FD FBP and DR ASIR reconstructions. (d) Comparison of CT numbers in co-registered ROIs between FD FBP and DR ASIR reconstructions.

Quantitative image analysis of CNR. (a) Comparison of same scan reconstruction of FBP and adaptive statistical iterative reconstruction (ASIR) for FD and DR scans. (b) Comparison of FD FBP to DR ASIR.
Noise reduction, contrast, and CNR measured in the Catphan 600 CTP 515 (low contrast) module in 15 mm diameter supra-slice objects and noise reduction measured in the vendor’s water phantom.

Ø – Diameter.
Fig. 4 shows a montage of clinical, Catphan, and water phantom images reconstructed using FBP and ASIR in addition to a subtraction image between the two reconstructions. In the clinical images, the noisy appearance of the difference image was confined to the CSF, indicating the location of the noise reduction. There was no apparent speckled appearance in the brain parenchyma, indicating little or no noise reduction. White matter appeared light and gray matter dark in the subtraction image reflecting the changes in contrast within the brain parenchyma, also shown in Fig. 5b. The subtraction image of Catphan 600 shows that the noise reduction is primarily confined to the low contrast objects with the largest contrast to the background. The subtraction image of the water phantom shows an even noise reduction across the image plane.
Same reconstruction comparison of FD and DR scans
Mean noise reduction and CT number difference between FD and DR scans. Comparison between FBP reconstructions, ASIR reconstructions, and FBP versus ASIR reconstructions.

Comparison of FD FBP and DR ASIR
Comparison of FD FBP reconstructed images to DR scans reconstructed with ASIR (Table 5, last column, Fig. 5c) showed a substantial decrease in noise of in CSF, a smaller noise reduction in white matter, and a noise increase in peripheral and central gray matter. There was also a change in image contrast similar to the results derived from same scan comparison, although with more variation (Fig. 5d). The CNR analysis showed better CNR for the dose reduced ASIR reconstruction (Fig. 6b), however for the central gray matter, white matter CNR the confidence intervals overlapped the equal CNR diagonal.
Subjective image quality evaluation
None of the results showed significant difference between the FD FBP and the DR ASIR reconstruction (Fig. 7). Relatively wide confidence intervals of the AUC estimates were observed.
Results of the qualitative image analysis. The area under the visual grading characteristics curve (AUC) for comparison of FD FBP and DR ASIR. The error bars show the extent of the 95% CI of the AUC for each criterion for qualitative image quality analysis.
Discussion
This study showed no significant difference between the FD FBP and DR ASIR scans for qualitative image quality. This can be interpreted as an indication that the scan techniques are approximately equally good, but caution is warranted as confidence intervals are wide. As Ahn et al. (23) note, proving one technique is not worse than another should pass a non-inferiority analysis. Other studies have reported no significant difference in diagnostic acceptability when using an ASIR level in the range of 20–40% when used to maintain image quality with decrease radiation dose (4,6–11). Readers should note that the P values used for this assessment vary from P = 0.06 (with DR ASIR tending towards worse image quality) (7) to P = 0.07 (with DR ASIR tending towards better image quality) (9). Another study also showed significantly worse overall diagnosability for DR scans reconstructed with ASIR, although the DR protocol was of sufficient quality and consequently recommended for routine use (12).
For quantitative image quality, 30% ASIR reconstructions resulted in substantial noise reduction in CSF in clinical images. In the brain parenchyma, the noise reduction was about 3% in white matter and potentially absent in gray matter (about 4% and 1% based on the same raw data analysis). Thus, ASIR does not appear to reduce noise substantially in the brain parenchyma. Other studies have measured similar results and attributed this effect to detail preservation in the brain parenchyma (4,7). The apparent slight increase in noise in gray matter is unexpected and might be explained by the increased contrast in the brain parenchyma. As gray matter is a thin structure, some white matter could have been included in the gray matter ROIs. As the contrast between white matter and gray matter is increased in the ASIR reconstruction, the noise measurements in the gray matter ROIs could have been artificially increased.
The CNR increased when using ASIR compared to FBP. In the brain parenchyma, the main reason for this increase was improved contrast, not reduced noise. The conservative dose reduction of 15%, was sufficient to reduce the CNR in ASIR reconstructions between central gray matter and white matter to a comparable level (as the confidence intervals overlapped the equal image quality diagonal) to the corresponding full dose FBP reconstruction. Therefore, we recommend using caution when reducing radiation dose while applying ASIR to counter the noise increase, as this potentially could lead to increased image noise in the brain parenchyma. As ASIR is proprietary software, the reason for more noise reduction in some areas compared to others is not known to the authors. However, statistical iterative reconstruction algorithms use cost functions with regularization and a priori information to control the reconstruction algorithm (24), which could be the reason for reduced noise suppression in the brain parenchyma.
In the vendors’ water phantom, the noise reduction due to ASIR is comparable to the noise reduction in CSF in clinical images. In Catphan the noise reduction varies with the objects present in the image. This result is relevant for researchers using phantom experiments to estimate dose reduction potential for iterative reconstruction. It highlights the importance of verifying that the iterative reconstruction’s effect on phantoms is similar to clinical images.
As the visualization of subtle pathology such as acute stroke in an inherently low contrast organ like the brain, unenhanced head CT demands images with relatively low noise (25). As ASIR claims to facilitate dose reduction due to decreased image noise (2), this uneven noise reduction is of concern. Especially, if noise measurements in CSF or in the vendor’s water phantom is used as a reference for the dose reduction potential. Thus, the uneven noise reduction could potentially lead to a decline in image quality in the brain parenchyma, thereby potentially increasing the likelihood of the radiologist missing an important finding.
This study had some limitations. There was 3% higher noise in white matter in FD compared to DR scans using the same reconstruction algorithm (Table 5). These results indicate the presence of a confounding factor, likely related to the cohort. The DR scans were always performed after the FD series, due to ethical considerations. Therefore, the FD scans might represent a patient population with more disease which may introduce more anatomical noise in white matter. This could have been avoided by acquiring both dose levels in the same scan session. However, this would imply increase radiation dose to the patients. Fourteen patients were included. Although this number is relatively low, we consider it to be sufficient to secure our conclusions. We especially point at the large confidence intervals in the qualitative analysis.
In conclusion, there was no significant difference in qualitative image quality between FD FBP and DR ASIR head CT images. ASIR reduced image noise in the CSF in clinical images and in the vendors’ water phantom, but this noise reduction was not reflected in the brain parenchyma. The observed CNR increase in the brain parenchyma was mostly due to increased image contrast. Thus, radiation dose reduction in head CT should be done with caution, due to the inhomogeneous noise reduction properties of ASIR.
Footnotes
Acknowledgements
The authors gratefully acknowledge image interpretation and valuable input to the manuscript from Thomas Alexander Skog, Pål Bache Martinsen, Mehran Rezai, and Till Schellhorn.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.