
Abstract
Trichobezoars are hairballs or hair-like fibers formed by chewing and swallowing hair or any other indigestible materials. Trichobezoars usually form in the gastric body and are thus prepyloric. However, trichobezoars may rarely pass through the pylorus into the duodenum, jejunum, ileum, and even the colon, in a condition referred to as Rapunzel syndrome. Here, we present a case of a 13-year-old girl with this rare syndrome and discuss the diagnosis and treatment of the disease.
Introduction
Bezoars are concretions of foreign and intrinsic material in the gastrointestinal tract. The term is thought to be derived from the Arabic word “Badzehr” or the Persian word “Padzhar,” which mean “antidote” (1). Bezoars can be classified into six types: phytobezoars, trichobezoars, lithobezoars, pharmacobezoars, plasticobezoars, and lactobezoars (2). Trichobezoars consist of hairballs or hair-like fibers caused by chewing and swallowing hair or any other indigestible materials. Trichobezoars usually form in the gastric body and are found prepylorically. However, some trichobezoars may pass through the pylorus into the duodenum, jejunum, ileum, and even into the colon in a condition termed Rapunzel syndrome (3), named after the German princess in Grimm’s Fairy Tales who let her long golden hair down from her tower to facilitate a tryst with her lover (4). The first report of Rapunzel syndrome dates back to 1968, when Vaughan described a patient with this disease (3). Approximately 30 cases only have been described in the literature since then (5).
Case report
A 13-year-old girl of normal intelligence presented with a 7-year history with hair in the feces and 3 months of upper abdominal pain with intermittent vomiting that worsened after meals.
The girl was 165 cm tall and weighed only 37 kg. She looked pale and a little depressed. She had no patchy alopecia or halitosis. Physical examination revealed a flat abdominal wall, normal bowel sounds, and a large solid palpable mass from the epigastrium to the periumbilical region; however, there were no signs of peritonitis.
The white blood cell count was 4.84 × 10^9/L, but a complete blood workup revealed slight hypochromic microcytic anemia, with a hemoglobin content of 138 g/L and a mean corpuscular volume (MCV) of 82.3 fL. The rest of the routine blood examination and blood biochemistry examination results were within normal limits. A computed tomography (CT) scan demonstrated a markedly expanded gastric cavity. Within the cavity was a heterogeneous, hypodense cast-like mass with scattered air bubbles that clearly oppressed the surrounding intestines. A similar agglomerate of mixed density was observed in the duodenum, while the colon was distended with gas (Fig. 1). No significant thickening of the gastrointestinal wall or any other signs of necrosis were observed.
CT scan of the abdominal region before operation demonstrated a trichobezoar in the stomach that extended into the duodenum.
An upper gastrointestinal endoscopy revealed a giant gastric trichobezoars (Fig. 2). An attempt was made to remove the bezoar by endoscopy using detritus pockets and grasping forceps, but these attempts were unsuccessful.
An endoscopic view of the trichobezoar.
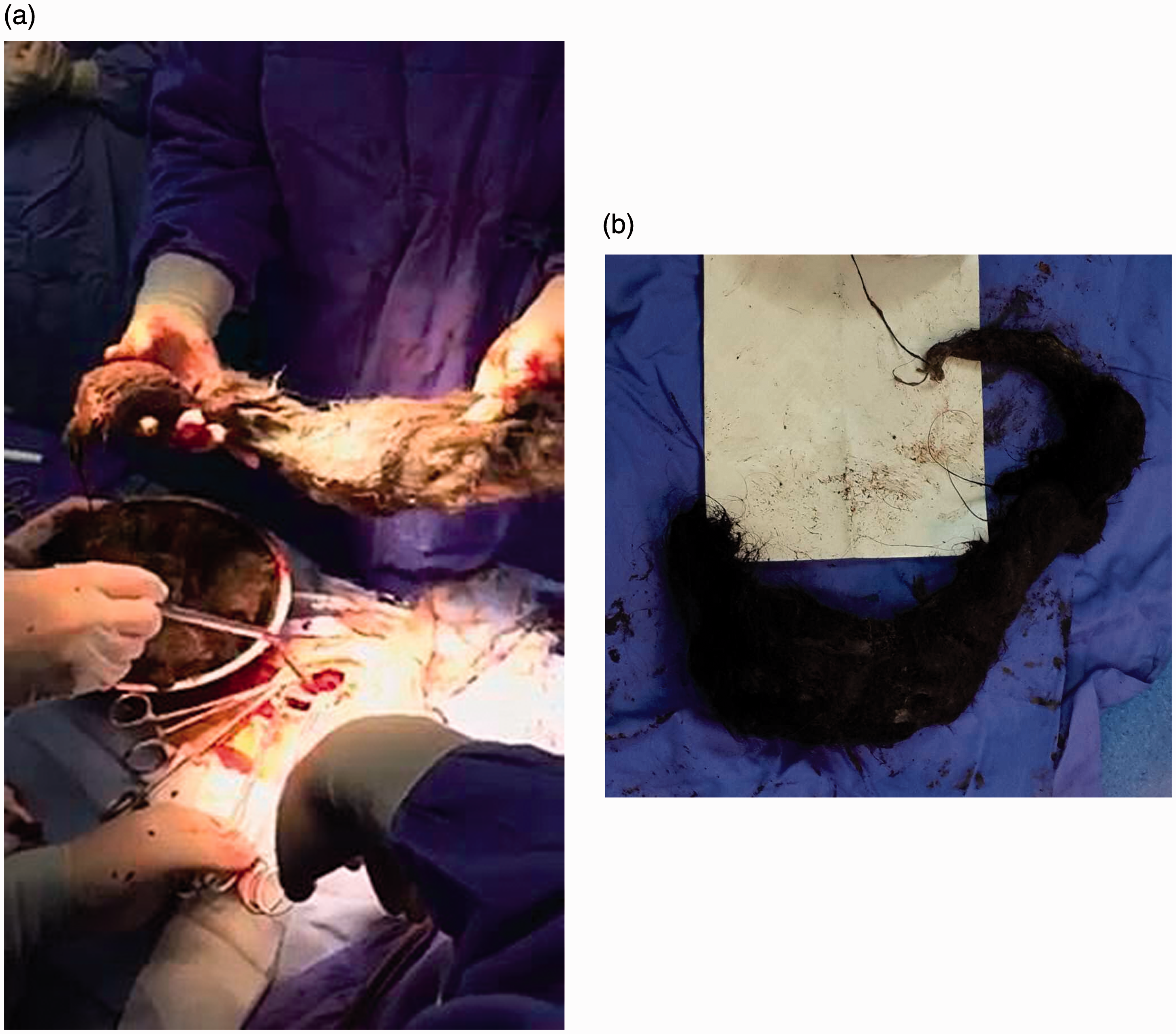
Due to the bulky size of the trichobezoar, the patient underwent exploratory laparotomy. An incision was made beginning from the center of the upper abdomen and extended vertically along the anterior wall of the stomach. The stomach was completely filled by the large trichobezoar, and a long tail extended through the pylorus and the duodenum into the upper parts of the jejunum. There was no evidence of gastric necrosis or intraperitoneal infection. Thus, the diagnosis of Rapunzel syndrome was confirmed. In order to remove the trichobezoar in the least invasive manner, pieces from the bulk of the bezoar were removed until the trichobezoar was fully removed (Fig. 3). The total length of the trichobezoar was approximately 25 cm, with a weight of 3250 g (Fig. 4a and b). During the operation, an endoscope was used and a single large wide-based polyp was found in the gastric body. The polyp was believed to be an inflammatory polyp and no attempt to remove the polyp was done.
The trichobezoar was removed in small pieces during gastrotomy. (a, b) The trichobezoar specimen.
The postoperative course was uneventful. The patient was discharged on day 9 after surgery and was advised to visit a psychiatrist (Fig. 5).
The surgical incision.
Discussion
Rapunzel syndrome is a rare variety of gastrointestinal trichobezoar. Although for most patients trichobezoar is easily diagnosed preoperatively, the diagnosis of Rapunzel syndrome should be considered from several aspects. First, a history of eating hair is essential in the diagnosis of Rapunzel syndrome. Patients who have this disease usually exhibit trichotillomania and trichophagia. These disorders are often the result of psychological problems or mental retardation (6). In this case, the parents of the patient indicated that the patient had exhibited a habit of playing with hair since childhood, and she would sometimes pick up hair and chew, which likely lead to swallowing.
The symptoms and physical signs that characterize Rapunzel syndrome depend on the size of the trichobezoar and the presence of complications. Current case reports show that the most common symptoms and signs are abdominal pain (37%), nausea and vomiting (33.3%), obstruction (25.9%), and peritonitis (18.3%). Uncommonly, patients have also presented with weight loss (7.4%), anorexia, hematemesis, and intussusceptions (7.4%) (5). In our case, the patient presented with trichophagia since the age of 6 years, while the main symptoms leading to the patient’s hospitalization were abdominal pain and intermittent vomiting. Finally, although a history of hair eating and patchy alopecia are often helpful in diagnosing Rapunzel syndrome, vague abdominal symptoms and signs make abdominal imaging examinations very important.
Abdominal imaging examinations include plain film, ultrasound, upper gastrointestinal series, and CT scan, while the final diagnosis should be made via upper gastrointestinal endoscopy (7). Plain film often denotes the presence of a non-specific mass, while ultrasound may demonstrate a band of increased echogenicity caused by the intermixed hair, air, and food in the trichobezoar. An upper gastrointestinal series can demonstrate a filling defect in the stomach, while CT scan demonstrates heterogeneous masses containing trapped air. Upper gastrointestinal endoscopy is considered to be the gold standard for the diagnosis of trichobezoar, but it may not prove the presence of a co-existing Rapunzel syndrome (8). The diagnosis of Rapunzel syndrome relies on the use of both CT scans and endoscopy prior to surgery. Clearly, it is important to differentiate Rapunzel syndrome from other diseases such as chronic gastritis, peptic ulcer, and gastric carcinoma. Abdominal ultrasound and barium meal (indicating the characteristic honeycomb appearance) may be useful. However, if Rapunzel syndrome is considered a possibility, a barium meal is not recommended because it may lead to obstruction or perforation. Furthermore, for most patients, an accurate preoperative diagnosis of trichobezoar can be achieved with definitive confirmation by endoscopy.
Treatment depends on the size of the trichobezoars and their location. Small trichobezoars can be removed endoscopically; successful endoscopic removals of gastric trichobezoars have been reported (9). However, a recent study by Gorter et al. showed that endoscopic removal of trichobezoars was successful in only approximately 5% of patients (10). Thus, large acutely symptomatic trichobezoars, especially when accompanied by Rapunzel syndrome, must be removed surgically preferably by a minimally invasive approach when possible. In a recent review of all case reports concerning trichobezoars, 100 of 108 patients (92.5%) were treated by laparotomy, with a 99% success rate and a 12% complication rate (10). In addition, it must be emphasized that the successful removal of large trichobezoars by laparotomy combined with anterior gastrotomy was confirmed by a retrospective analysis of 34 cases published in 2005 (11). Moreover, three reports have indicated the successful laparoscopic removal of trichobezoars in pediatric patients, of which two had Rapunzel syndrome (12–14). However, we still advocate the use of a laparoscopic approach only for appropriate patients due to increased operating time, the added risk of intra-abdominal spillage of the trichobezoar contents, and the necessity of extended incisions. In our case, considering the large size of the trichobezoar, the most effective and least invasive method was regional laparotomy, wherein the trichobezoar was removed in small pieces.
Although the recurrence of Rapunzel syndrome is extremely rare, there is no doubt that the prevention of recurrence is critical. The most common reason for recurrence is patients lost in follow-up and therefore did not complete psychological treatment. There has been research showing that long-term follow-up and professional psychotherapy are critical after the surgical removal of trichobezoars (15).
In conclusion, although Rapunzel syndrome is a rare disease, it should be considered when diagnosing young women, especially those with a history of trichophagia or trichotillomania. The diagnosis of Rapunzel syndrome is possible via imaging, and endoscopy is a direct and accurate diagnostic method. In terms of treatment, laparotomy remains superior to laparoscopic surgery. After the surgical removal of trichobezoars, long-term follow-up combined with psychiatric consultation is recommended.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.