
Abstract
Background
Synthetic magnetic resonance imaging (MRI), a technique that enables creation of various contrast-weighted images from a single MRI quantification scan, is a useful clinical tool. However, there are currently no reports examining the use of contrast-enhanced synthetic MRI for detecting brain metastases.
Purpose
To assess whether contrast-enhanced synthetic MRI is suitable for detecting brain metastases.
Material and Methods
Ten patients with a combined total of 167 brain metastases who underwent quantitative MRI and conventional T1-weighted inversion recovery fast spin-echo (conventional T1IR) MRI before and after administration of a contrast agent were included in the study. Synthetic T1IR and T1-weighted (synthetic T1W) images were produced after parameter quantification. Lesion-to-white matter contrast and contrast-to-noise ratio were calculated for each image. The number of visible lesions in each image was determined by two neuroradiologists.
Results
The mean lesion-to-white matter contrast and mean contrast-to-noise ratio of the synthetic T1IR images were significantly higher than those of the synthetic T1W (P < 0.001 and P < 0.001, respectively) and conventional T1IR (P = 0.04 and P = 0.002, respectively) images. Totals of 130 and 124 metastases were detected in the synthetic T1IR images by the first and second radiologists, respectively. The corresponding numbers were 91 and 85 in the synthetic T1W images and 119 and 119 in the conventional T1IR images. Statistical significance was not found among detected numbers of lesions.
Conclusion
Synthetic T1IR imaging created better contrast compared with synthetic T1W or conventional T1IR imaging. The ability to detect brain metastases was comparable among these imaging.
Keywords
Introduction
Brain metastases are the most common tumor of the central nervous system (1). It is estimated that more than 21,000 patients per year develop brain metastases in the United States (2). In cancer patients, the incidence of brain metastases is 9–17%, although the exact incidence is likely to be higher (3). The incidence of brain metastases is increasing (1), partly because of increase in the incidence of primary cancers and partly because improvements in treatment options have prolonged survival of patients with cancer, which increases the chance of primary tumors metastasizing.
Contrast-enhanced magnetic resonance imaging (MRI) is useful for detecting brain metastases. Early detection of brain metastases is crucial because the management strategies available after early diagnosis result in a better patient quality of life (4). T1-weighted (T1W) imaging is the most commonly used MRI sequence for evaluating brain metastases. T1-weighted inversion recovery (T1IR) is a newer pulse sequence that offers better contrast between gray and white matter of the brain than does a typical T1W sequence (5). However, there are contradictory reports regarding the sensitivity of contrast-enhanced T1IR and T1W images for detecting brain lesions (6–8).
Synthetic MRI is a technique that can produce images with almost any contrast weighting by virtually changing repetition time (TR), echo time (TE), and inversion time (TI) after quantification of longitudinal T1 and transverse T2 relaxation times and proton density (PD) (9,10). A recently developed MRI quantification pulse sequence, QRAPMASTER, is now in clinical use and has dramatically shortened the time needed for parameter quantification (11). The QRAPMASTER method assumes the process of T1 and T2 relaxation times to be monoexponential, whereas it may be multiexponential for many tissues. However, a phantom study has revealed good accuracy and reproducibility for T1, T2, and PD measurements by the QRAPMASTER method (12). Synthetic MRI is particularly useful when many different contrast settings are required. Synthetic MRI of the brain without the use of a contrast agent has been reported to produce images that have inferior image quality but diagnostic power comparable to that of images obtained via conventional MRI sequences (13). Therefore, if the diagnostic power of images obtained via synthetic MRI after administration of a contrast agent is also proved to be comparable to that of conventional MRI, synthetic MRI would be a useful means of screening for brain metastases. However, there are currently no reports in the literature of studies examining the use of contrast-enhanced synthetic MRI for detecting brain metastases.
In the present study, we assessed the use of synthetic MRI to detect brain metastases by comparing lesion-to-white matter contrast, contrast-to-noise ratio, and number of brain metastases detected in images obtained with synthetic and conventional MRI sequences.
Material and Methods
The present study was approved by the institutional review board of Juntendo University Hospital, Japan. Written informed consent was not required for this study because of its retrospective nature. All the patient information was anonymized and de-identified prior to analysis.
Data from 19 consecutive cancer patients (11 men, 8 women; mean age, 63.1 years; age range, 44–75 years) suspected of having brain metastases who underwent quantitative MRI and conventional T1-weighted inversion recovery fast spin-echo MRI (conventional T1IR) before and after administration of a gadolinium-based contrast agent from April 2015 through July 2015 were retrospectively reviewed. Ten patients (6 men, 4 women; mean age, 62.3 years; age range, 44–75 years) had at least one brain metastasis and were included in the study. The primary lesions of these metastases were lung cancer (n = 6), breast cancer (n = 2), and esophageal cancer (n = 2). Diagnoses were made on the basis of clinical history, presentation, or follow-up imaging studies.
MRI
In all patients, MRI was performed on a 3.0-T MRI system (Discovery MR750w, GE Healthcare, Milwaukee, WI, USA) with a 12-channel head coil. All patients underwent conventional T1IR imaging and quantitative imaging before and after intravenous administration of a gadolinium-based contrast agent. The dose of contrast medium was 0.1 mmol/kg and the contrast agent used was one of the followings: Omniscan (Daiichi-Sankyo, Tokyo, Japan), ProHance (Bracco-Eisai, Tokyo, Japan), Magnevist (Bayer Vital, Leverkusen, Germany). Contrast-enhanced conventional T1IR imaging and quantitative MRI were performed before administration of a contrast agent and approximately 1 and 7 min after administration of a contrast agent, respectively. Axial, sagittal, and coronal images were obtained, in that order, for conventional T1IR imaging, and only axial images were obtained for quantitative MRI.
Quantitative MRI was performed by using the two-dimensional QRAPMASTER pulse sequence (11). The QRAPMASTER pulse sequence is a multi-slice, multi-echo, and multi-saturation delay saturation recovery turbo spin-echo acquisition method with which images are collected for different combinations of TE and saturation delay time (TD). In our institution, two sets of TE values and four sets of TD values are used to make eight real images and eight imaginary images for quantification of longitudinal T1 and transverse T2 relaxation times and PD. The TE values used were 16.9 and 84.5 ms, and TD was set as defined by the manufacturer (SyntheticMR AB, Linköping, Sweden). The parameters used for quantitative MRI were: field of view (FOV), 240 mm × 240 mm; matrix, 320 × 320; ETL, 10; bandwidth, 31.25 kHz; slice thickness/gap, 4.0 mm/1.0 mm; slices, 30. The acquired data were used to calculate T1, T2, and PD maps at each slice position, which were then used to calculate the synthetic MR images. Quantification map acquisition and raw data processing were performed with SyMRI software (v. 7.2 RC2, SyntheticMR AB) on a commercial personal computer in less than 1 min and synthetic images were created in real-time.
Two experienced neuroradiologists (AH and MH) reviewed the synthetic images of 19 original patients and determined the most appropriate parameters for detecting brain metastases visually while maintaining the T1-weighting contrast. Synthetic T1-weighted inversion recovery (synthetic T1IR) images were produced by using the following parameters: TR, 500 ms; TE, 5 ms; TI, 440 ms. Synthetic T1-weighted (synthetic T1W) images were produced for comparison by using the following parameters: TR, 390 ms; TE, 15 ms. Conventional T1IR images before and after administration of a gadolinium-based contrast agent were obtained by using the following parameters: TR, 3294 ms; TE, 18 ms; TI, 908 ms; FOV, 240 × 216 mm; matrix, 352 × 256; ETL, 8; slice thickness/gap, 4 mm/1 mm; slices, 30. Acquisition time was 1 min 50 s for conventional T1IR and 7 min 12 s for quantitative MRI before and after administration of a contrast agent. Images were saved as DICOM files (Digital Imaging and Communications in Medicine) and analyzed by using OsiriX MD software (v. 6.5.2, Pixmeo, Geneva, Switzerland).
Image analysis
Two neuroradiologists (MH and AH) reviewed all the MRI sequences and agreed that a total of 167 nodules were included in the study. The image quality of the contrast-enhanced synthetic T1IR images was compared with that of the contrast-enhanced synthetic T1W and contrast-enhanced conventional T1IR images by using two quantitative and one qualitative criteria. Only axial images were used for the quantitative and qualitative analyses. Sagittal and coronal conventional T1IR images were used only for counting the total number of brain metastases with axial images (as “Gold Standards”) by MH and AH.
Quantitative analysis
The quantitative criteria were lesion-to-white matter contrast and contrast-to-noise ratio. Region-of-interest (ROI) analyses were performed on the contrast-enhanced synthetic T1IR, contrast-enhanced synthetic T1W, and contrast-enhanced conventional T1IR images by a single investigator (MN). For the quantitative analysis, the signal intensity of the tumors and corresponding white matter were measured by means of ROI analyses and mean values were recorded. Tumors that were found on both the contrast-enhanced synthetic images and the contrast-enhanced conventional T1IR images were included in the analysis. In most cases, an ROI of approximately 3 mm2 that covered the lesion and corresponding white matter was used, but its size was adjusted for lesions smaller than 3 mm2. The corresponding white matter for supratentorial lesions was defined as the white matter adjacent to lesions that showed no edema. The corresponding white matter for infratentorial lesions was defined as the white matter in the brainstem in the same slice that showed no edema.
In synthetic MRI, the signal intensity of the surrounding air is set at zero. Hence, the median standard deviation of the signal intensities of the following 12 ROIs, all of which were approximately 3 mm2 in size, was defined as the noise for each patient: ROIs in the cerebrospinal fluid (bilaterally in the anterior horns of the lateral ventricles), in the gray matter (bilaterally in the thalamus, occipital cortex, and frontal cortex), and in the white matter (bilaterally in the centrum semiovale and in the corpus callosum—one in the genu and one in the splenium). This method was modified from the technique used by Blystad et al. (13).
Lesion-to-white matter contrast was defined as the difference between the mean signal intensities of a lesion and the corresponding white matter divided by the signal intensity of the corresponding white matter. Contrast-to-noise ratio was defined as the difference between the signal intensities of a lesion and the corresponding white matter divided by the noise of each sequence.
Qualitative analysis
For the qualitative analysis, two experienced neuroradiologists (MS and MY) counted the number of lesions in the axial contrast-enhanced synthetic T1IR, contrast-enhanced synthetic T1W, and contrast-enhanced conventional T1IR images from the 10 patients with brain metastases, which were shown in a random order. Radiologists were blinded to different types of images. Each contrast-enhanced image was shown with the corresponding non-contrast-enhanced image for reference. Counted lesions that were not included in the 167 lesions determined by MH and AH were categorized as false positive.
Statistical analysis
Statistical computing was performed with the free software R Ver. 3.2.1 (R Foundation for Statistical Computing, Vienna, Austria. URL http://www.R-project.org/). Because all of the datasets were not normally distributed, we used the Friedman test, which is a non-parametric test, to compare the lesion-to-white matter contrast, contrast-to-noise ratio, and number of lesions detected in the synthetic T1IR, synthetic T1W, and conventional T1IR images. Post-hoc pairwise tests with Holm correction were performed to determine statistical significance. A two-sided P value of less than 0.05 was considered significant.
Results
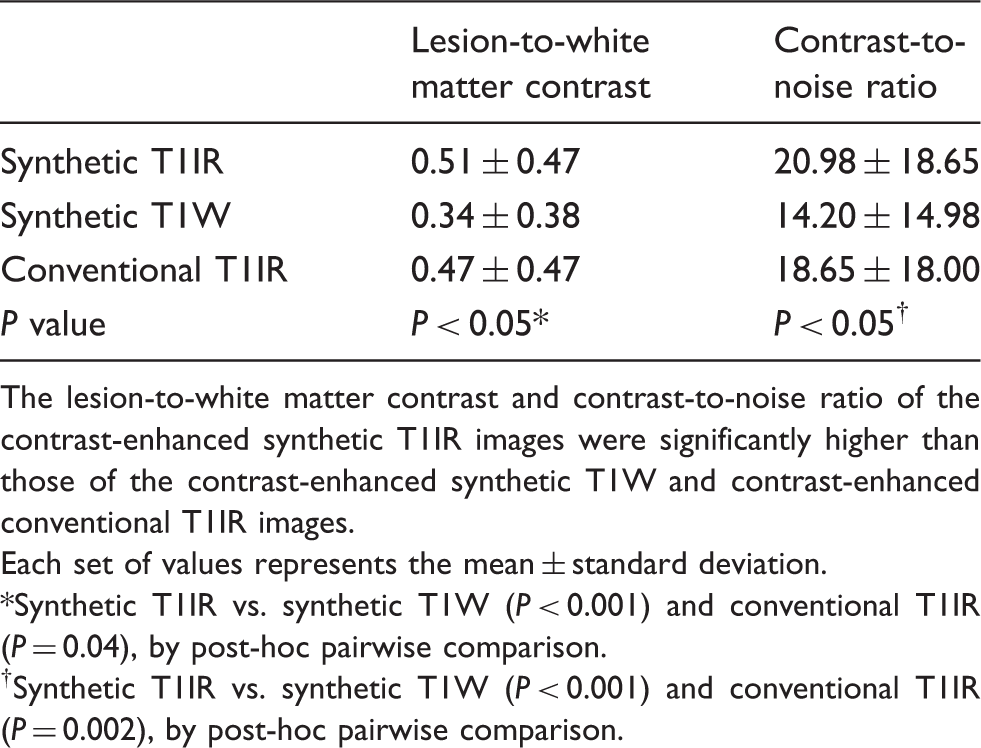
The lesion-to-white matter contrast and contrast-to-noise ratio of the contrast-enhanced synthetic T1IR images were significantly higher than those of the contrast-enhanced synthetic T1W and contrast-enhanced conventional T1IR images (Table 1). The number of lesions detected by two neuroradiologists in the synthetic T1IR images was higher than those in the synthetic T1W and conventional T1IR images without statistical significance (Table 2, Fig. 1).
Example MR images showing metastases that could not be identified with contrast-enhanced synthetic T1-weighted (T1W) imaging. (a) Contrast-enhanced synthetic T1-weighted inversion recovery (T1IR) image. (b) Contrast-enhanced conventional T1IR image. (c) Contrast-enhanced synthetic T1W image. Four small metastases can be identified in both (a) and (b) (arrows) but only one can be identified in (c) (arrow). These metastases were missed on synthetic T1W image by the two neuroradiologists in the qualitative analysis. Lesion-to-white matter contrast and contrast-to-noise ratio of contrast-enhanced synthetic T1-weighted inversion-recovery (T1IR), contrast-enhanced synthetic T1-weighted (T1W), and contrast-enhanced conventional T1IR images. The lesion-to-white matter contrast and contrast-to-noise ratio of the contrast-enhanced synthetic T1IR images were significantly higher than those of the contrast-enhanced synthetic T1W and contrast-enhanced conventional T1IR images. Each set of values represents the mean ± standard deviation. Synthetic T1IR vs. synthetic T1W (P < 0.001) and conventional T1IR (P = 0.04), by post-hoc pairwise comparison. Synthetic T1IR vs. synthetic T1W (P < 0.001) and conventional T1IR (P = 0.002), by post-hoc pairwise comparison. Numbers of lesions detected by two neuroradiologists in contrast-enhanced synthetic T1-weighted inversion recovery (T1IR), contrast-enhanced synthetic T1-weighted (T1W), and contrast-enhanced conventional T1IR images. The number of lesions detected by two neuroradiologists in the synthetic T1IR images was higher than those in the synthetic T1W and conventional T1IR images without statistical significance. Each value represents the total number of detected lesions with the number of false-positive lesions in parentheses. Synthetic T1IR vs. synthetic T1W (P = 0.11) and conventional T1IR (P = 0.30), by post-hoc pairwise comparison. Synthetic T1IR vs. synthetic T1W (P = 0.065) and conventional T1IR (P = 0.525), by post-hoc pairwise comparison.

In the present study, contrast-enhanced synthetic T1IR produced the best quality contrast for detecting brain metastases. Although the numbers of lesions detected did not differ statistically, contrast-enhanced synthetic T1IR images enabled detection of more metastases than contrast-enhanced conventional T1IR and synthetic T1W images.
In the qualitative analysis, several metastases were detected in the synthetic T1IR and synthetic T1W images but not in the conventional T1IR images. These included metastases that were hidden by flow-related artifacts from the sigmoid sinus (Fig. 2). In the present study, the transverse and sigmoid sinuses tended to cause signal voids on contrast-enhanced synthetic images and flow-related artifacts were less pronounced in the contrast-enhanced synthetic images than in the contrast-enhanced conventional T1IR images. Indeed, some small cortical metastases were identifiable only in the contrast-enhanced synthetic T1IR and synthetic T1W images because they resembled blood vessels in the contrast-enhanced conventional T1IR images, especially when they were adjacent to superficial vessels (Fig. 3). These results demonstrate the potential advantages of synthetic MRI compared with conventional MRI, although further investigation is needed.
Less flow-related artifacts from the sigmoid sinus were observed with contrast-enhanced synthetic T1-weighted inversion recovery (T1IR) and contrast-enhanced synthetic T1-weighted (T1W) imaging compared with contrast-enhanced conventional T1IR imaging. (a) Contrast-enhanced synthetic T1IR image. (b) Contrast-enhanced synthetic T1W image. (c) Contrast-enhanced conventional T1IR image. A metastasis (arrows) located next to the left sigmoid sinus is obvious in (a) and (b) but is obscured by flow-related artifacts from the sigmoid sinus in (c). Cortical metastases resembled blood vessels in contrast-enhanced conventional T1-weighted inversion recovery (T1IR) images. (a) Contrast-enhanced synthetic T1IR image. (b) Contrast-enhanced synthetic T1-weighted image. (c) Contrast-enhanced conventional T1IR image. A small cortical metastasis (arrow) is obvious in (a) and (b) but resembles a blood vessel in (c) because of its small size and clear demarcation.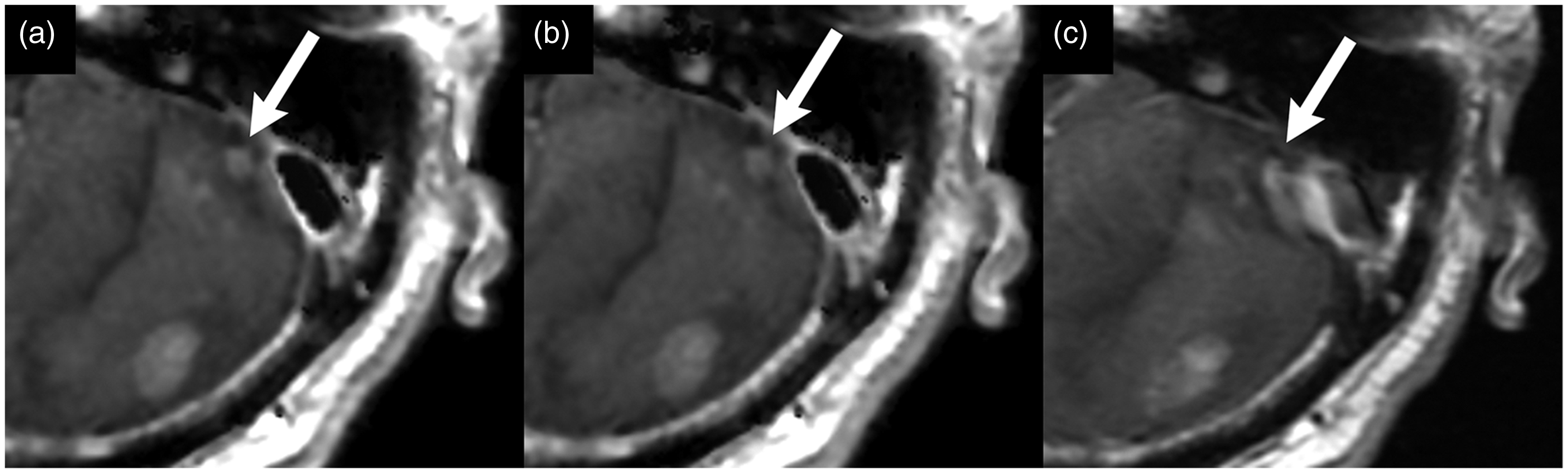

Discussion
A potential advantage of synthetic MRI over conventional MRI is the creation of any contrast weighting after image acquisition. Although in the present study we used identical parameters for all 10 patients, it would also have been possible to synthesize images with parameters tailored to each individual to maximize the potential to detect brain metastases. Further optimization of contrast weighting is needed to maximize the ability to detect brain metastases by using synthetic MRI. Although the scan time for quantitative MRI (7 min 12 s) was longer than that of conventional T1IR sequence (1 min 50 s) after administration of a contrast agent, the ability to synthesize images optimized for each individual and the potential to avoid multiple scans needed for conventional T1W, T1IR, or FLAIR imaging are clear advantages of synthetic MRI. In addition, contrast-enhanced synthetic double inversion recovery imaging, which suppresses signals from the cerebrospinal fluid and bone marrow fat, may also be useful for evaluating dural enhancement (14).
There are some limitations in the present study. First, the number of patients was small. Second, since quantitative MRI was performed after conventional T1IR imaging after administration of a contrast agent, differences in the timing of image acquisition may have affected the degree of lesion enhancement. Acquiring spin-echo T1W images with delays of up to 30 min after administration of a contrast agent increased the rate of detection of cerebral metastases compared with acquiring the images immediately after administration of contrast agent (15,16). However, a delay of only 1 min after administration of a contrast agent offered better contrast between brain metastases and white matter than did a delay of 10 min (17).
In conclusion, contrast-enhanced synthetic T1IR imaging produced images with better lesion-to-white matter contrast and contrast-to-noise ratio than did contrast-enhanced synthetic T1W and contrast-enhanced conventional T1IR imaging. More brain metastases were detected with contrast-enhanced synthetic T1IR than with the other sequences, but this result was not statistically significant.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from MEXT-Supported Program for the Strategic Research Foundation at Private Universities (2011–2015) and funded by ImPACT Program of Council for Science, Technology and Innovation (Cabinet Office, Government of Japan).