
Abstract
In spite of the growing efforts oriented towards revealing different aspects of emphysema, the persistence of the emphysematous or emphysema-like changes (ELCs) is not explored yet in the open literature. In this study we demonstrate the persistence of an ELC for 22 years in a spontaneous pneumothorax (SP) patient which indicates a hitherto unknown gas supply to the ELC. For this purpose we used high resolution computed tomography (HRCT) images processed into three-dimensional (3D) geometry. By the same token, not only a long persistence but also the volume increase of this ELC between 2002 and 2010 was demonstrated. The 3D geometry visualized an aerated interstitial structure between the sites of supposed gas leakage at the wall of the third generation airways and the ELC. This potential gas conducting interstitial pathway is not a continuation and has neither the form nor the structure of a bronchus. The finding suggests that in this patient the intrabronchial gas passes through the bronchial wall and via a gas conducting interstitial pathway reaches the ELC. Despite the availability of the presently employed techniques for at least 15 years, such case and phenomenon have not been described previously. The retrieval of the patient suggests that the findings could be relevant for a considerable proportion of the population.
Keywords
Introduction
Clinical and physiological investigations have demonstrated the irreversible progress of emphysema even after cessation of smoking (1). Emphysematous changes develop at the distal parts of the respiratory system (1). They appear on high resolution computed tomography (HRCT) as localized areas of low attenuation with thin or imperceptible walls in the pulmonary tissue of smokers. Identical radiological findings in patients who suffered from spontaneous pneumothorax (SP) but never smoked are called emphysema-like changes (ELCs) (2). Their number is strongly correlated to the number of SP events (2,3). An ELC (similarly to a SP), will be absorbed within weeks without gas supply. However, no study is available on the development and persistence of ELCs. The objective of this work was to present a case with ELC persisting for at least 22 years, being supplied with gas through an interstitial pathway.
Case report
Parameters of HRCT investigations from 2002, 2007, 2009, and 2010 (2010/a with GE 64 row HRCT and 2010/b with Philips Brilliant 40 row HRCT).

Total volumes of ELCs and their tails (aerated interstitial structure) and the volume of non-gas fraction of ELCs.

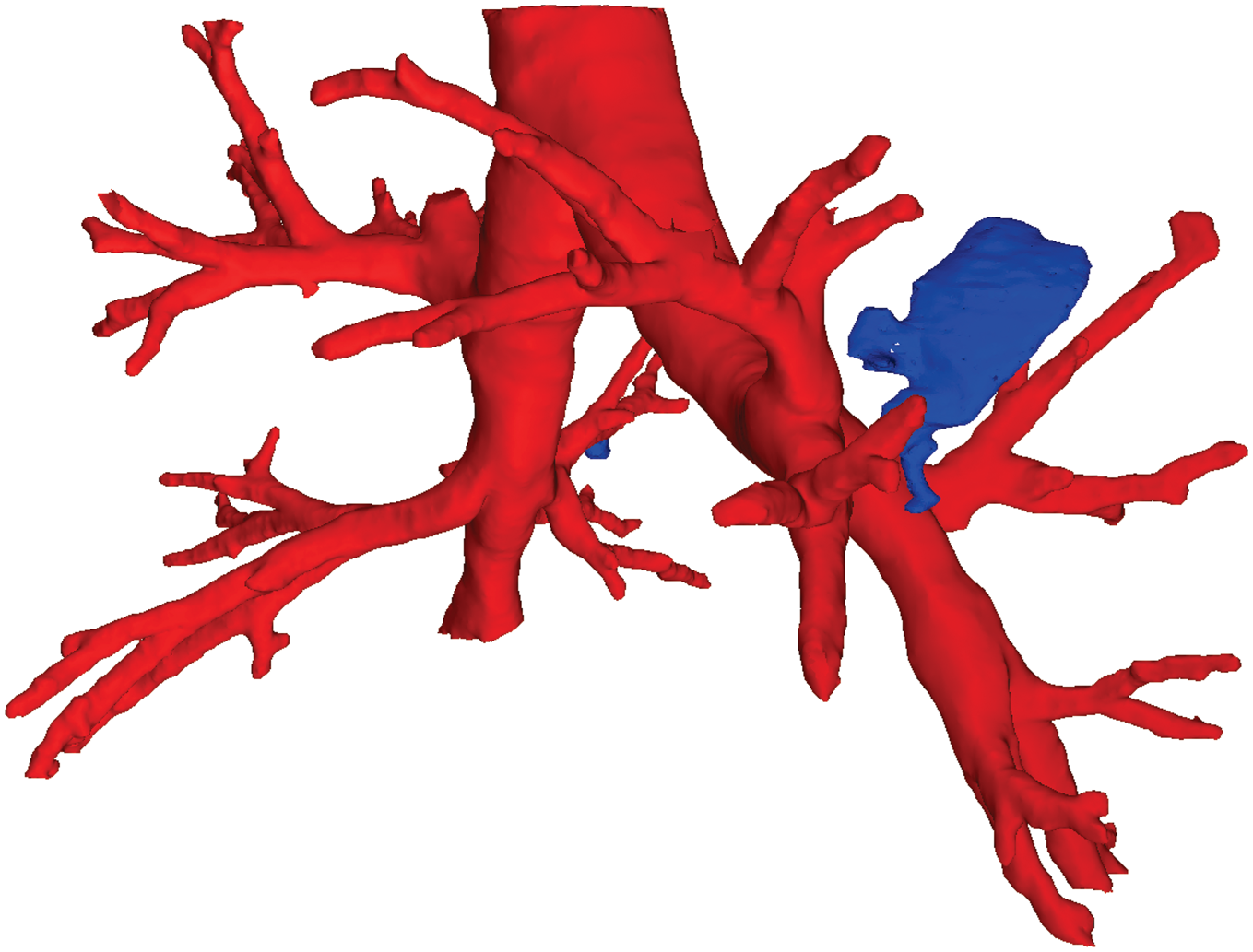
The persistence of the ELC for 22 years indicates a gas supply to the ELC in this patient. Since HRCT images alone did not demonstrate any bronchial gas supply to the ELC, we applied a more sensitive technique. The HRCT images were processed mathematically for 3D geometry reconstruction (5,6) purposes to find the hypothesized gas refilling “interstitial pathway”. The reconstructed geometry is shown in Figs. 1 and 2. Fig. 2 is a 3D figure and has got “rotate” and “enlarge” functions as well. As the figures demonstrate, the 3D method visualized an aerated interstitial structure (blue) with no perceptible border or form like a bronchial wall in the left lung between the third generation airway and the approximately 20 mm in diameter ELC. The two proximal tails of the aerated interstitial structure approached the visualized intrabronchial gas (2.4 and 4.4 mm distance) and were attached to the ELC. The 2.4 and 4.4 mm wide gaps between the intrabronchial gas (pink) and the aerated interstitial structure (blue) correspond to the non-visualized bronchial wall with its protuberances. Therefore, the distance between the external surface of the bronchial wall and the proximal tails of the aerated interstitial structure was virtually zero. The tails merged into a less than 2 mm wide part and then broadened until the approximately 20 mm large ELC. The measurements demonstrated the enlargement of the ELC (blue) and the aerated interstitial structure (blue) between 2002 and 2010 (Table 2).
The posterior view of the reconstructed geometry of the tracheobronchial tree, ELCs, and the pulmonary gas conducting “interstitial pathway” connecting the left third presegmental bronchus with the left-sided ELC. The right-to-left diameter of the trachea is 21 mm. The bronchial walls are not visualized. The right-sided ELC (4–6 mm in diameter) was not detected in the 8 mm interval between the 2 mm thick HRCT sections in 1988, but detected in every HRCT examination between 2002 and 2010. Please see the link to 3D image Figure 2. The 3D image with zoom and rotate functions shows the left-sided ELC approximately 20 mm in diameter with the “gas conducting interstitial pathway” leading to the ELC (with blue). This figure shows the 3D bronchial geometry. The intrabronchial gas is visualized with pink color. The size of the right–left diameter of the trachea is 21 mm. The 3D bronchial geometry may be enlarged/decreased and rotated to any direction with the help of the mouse/cursor. The carina is at –140 mm and the left ELC is between –133 and –163 mm of the vertical height of the axial sections. The bronchial walls are not visualized. The ELC and the pulmonary gas conducting “interstitial pathway” with tails are marked with blue color. The proximal tails of the “gas conducting interstitial pathway” are approximately 2.5–4.5 mm to the inner surface of the left third AGs. The “gas conducting interstitial pathway” is connected to the ELC by a conical intersection. This pathway is rather narrow and allows only limited streaming of gas which may explain the limited change of the volume. The second ELC (4–6 mm large, blue colored) in the right middle region remained undetected in 1988, but it was demonstrated in 2002, 2007, 2009, and 2010.
Discussion
The gas from an ELC or SP would be absorbed within weeks unless the supplied gas replaced the absorbed one. The persistence of an ELC for 22 years proves a balance between the amounts of the supplied and the absorbed gas to/from the ELC. The volume increase of the ELC and the aerated interstitial structure even points to a ventil effect. In order to explain the origin of the supplied gas, we hypothesize that the intrabronchial gas passes through the bronchial wall of the left third generation airway and the pulmonary parenchyma to the ELC (7).
The transparietal leakage suggests hitherto non-visualized discontinuation(s) of the layers of the anomalous bronchial wall, which may be given more consideration in the future. It may be surmised that the two point-like sites where the tails are attached to the third generation airway are “loci minoris resistentiae” of the bronchial wall where the intrabronchial gas leaks. The persistence of the ELC and the volume increase in both the ELC and the aerated interstitial structure suggest that the demonstrated aerated interstitial structure is a pulmonary gas conducting interstitial pathway to the ELC.
The discreet form of the interstitial gas conducting pathway indicates that the interstitial gas does not diffuse freely throughout a homogenous pulmonary tissue. Instead, the migration of gas in the pulmonary tissue/interstitium is determined by a balance of density differences of the pulmonary tissue/interstitium and a pressure gradient (7) in that. The patient’s history of SP demonstrated bronchial anomalies (4), and a bronchial perforation (5) due to the rupture of a proptos (6). This may suggest that his airways are weak due to both anomalous branching and structure.
The demonstration of the left-sided interstitial gas conducting pathway years prior to the contralateral right main bronchus perforation excludes a causal relationship between them. The continuousness of bronchial pathway in emphysema is proved by morphological studies and the therapeutic efforts are based on the bronchodilating effect on the small airways. Due to the radiological limitations in visualizing the continuousness of a bronchial pathway in emphysema and to discern that from the pulmonary gas conducting interstitial pathway, we stated that gas conducting interstitial pathway has no structure, form or size of a bronchus. The central location of the ELC was an advantage for the detection of the interstitial gas conducting pathway and its contact points to the third generation airway and ELC. A small gas supplying bronchus would have been more difficult to exclude/visualize at the periphery.
No other study has dealt with the development, central/peripheral distribution, and persistence of ELC in those who never smoked, neither with emphysematous bullae or blebs in smoker patients regarding secondary/COPD related SP. Even though the methods used in this investigation have been available for at least 15 years, no similar connection between an ELC and a presegmental airway has been shown. There are more than 100 papers in the available literature which state that they deal with ELC. Several of these papers describe animal studies. Some human studies are restricted to subjects who contracted different diseases. However, the denomination of ELC in these studies is deviating from our definition of ELC (2), which is not considered as a rule not even in the studies on SP. Another confusing fact is that gas filled emphysematous or ELCs are called cyst in Birt-Hogg-Dube syndrome (8) – like they were containing fluid, and no one objects this impossibility. There is no information on the smoking habits of the patients as a rule. Therefore it is impossible to discern emphysematous or emphysema-like changes (ELCs). Another item of information that is absent is the central or peripheral distribution of emphysema or ELC, which is available only in our paper on ELC (2). Only the necessary combination of persistence of the ELC, migration theory of interstitial gas, and the radiological and numerical reconstruction of the HRCT to 3D, could demonstrate the existence of the gas conducting interstitial pathway. The results imply the possibility to find the entrance of the intrabronchial gas into the anomalous bronchial wall and seal that passage to large ELCs. That may reduce both their size and adverse effect on pulmonary structure and function. This report on the 22-year-long persistence of a central ELC and its connection to a presegmental airway via a pulmonary gas conducting interstitial pathway is the first of its kind and there is no predecessor of it to refer to.
In conclusion, we have demonstrated a persistent pulmonary gas conducting interstitial pathway between the side of a presegmental airway and a persistent ELC. This suggests the escape of the intrabronchial gas across the anomalous presegmental bronchial wall. The migration of the gas in the pulmonary tissue ought to be determined by the locally lower density of the interstitial tissue than elsewhere and the pressure gradients during inhalation. Current findings could be relevant for a considerable proportion of the population.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.