
Abstract
Background
High mammographic density might mask breast tumors, resulting in delayed diagnosis or missed cancers.
Purpose
To investigate the association between mammographic density and histopathologic tumor characteristics (histologic type, size, grade, and lymph node status) among women screened in the Norwegian Breast Cancer Screening Program.
Material and Methods
Information about 1760 screen-detected ductal carcinoma in situ (DCIS) and 7366 invasive breast cancers diagnosed among women aged 50–69 years, 1996–2010, was analyzed. The screening mammograms were classified subjectively according to the amount of fibroglandular tissue into fatty, medium dense, and dense by breast radiologists. Chi-square test was used to compare the distribution of tumor characteristics by mammographic density. Odds ratio (OR) of tumor characteristics by density was estimated by means of logistic regression, adjusting for screening mode (screen-film and full-field digital mammography), and age.
Results
Mean and median tumor size of invasive breast cancers was 13.8 and 12 mm, respectively, for women with fatty breasts, and 16.2 and 14 mm for those with dense breasts. Lymph node positive tumors were identified among 20.6% of women with fatty breasts compared with 27.2% of those with dense breasts (P < 0.001). The proportion of DCIS was significantly lower for women with fatty (15.8%) compared with dense breasts (22.0%). Women with dense breasts had an increased risk of large (OR, 1.44; 95% CI, 1.18–1.73) and lymph node positive tumors (OR, 1.26; 95% CI, 1.05–1.51) compared with women with fatty and medium dense breasts.
Conclusion
High mammographic density was positively associated with tumor size and lymph node positive tumors.
Introduction
High mammographic density is known to mask breast tumors, leading to delayed diagnosis and reducing the effectiveness of mammographic screening (1,2). Tumors masked by high mammographic density are often characterized by a less favorable prognosis (3–7). This is reflected by larger tumor size (3–7), higher histologic grade (6), and lymph node involvement (4,5,7). However, a recent study reported that very low density predicted poorer outcome in women with invasive breast cancer (8). To better understand potential impact of mammographic density on prognosis among women participating in the Norwegian Breast Cancer Screening Program (NBCSP), we investigated the association between mammographic density and histopathologic characteristics of screen-detected tumors.
Material and Methods
The NBCSP is a population-based program inviting women aged 50–69 years to two-view mammography every second year. About 75% of the invited women participate. The program is administered by the Cancer Registry of Norway (9). A nationwide screening database contains information about all screening and recall examinations. This study was approved by the Regional Committee for Medical and Health Research Ethics.
In this case-only study, we included information about 1760 screen-detected ductal carcinoma in situ (DCIS) and 7366 invasive breast cancers diagnosed among women aged 50–69 years at diagnosis in the period 1996–2010. Mammographic density was subjectively classified according to the percentage of fibroglandular tissue on the screening mammogram as fatty (<30% of fibroglandular tissue), medium dense (30–70% of fibroglandular tissue), and dense (>70% of fibroglandular tissue) by the trained breast radiologists who performed the diagnostic workup. To start working as breast radiologists in the NBCSP, radiologists have to undergo special training (10). In addition, to continue reading mammograms in the program, breast radiologists are recommended to read a minimum of 5000 screening examinations annually and to conduct diagnostic mammography (10).
Chi-square test was used to compare the distribution of histologic type (DCIS, invasive ductal carcinoma [IDC], invasive lobular carcinoma [ILC], and other invasive cancers) and to compare the distribution of tumor size (≤15 mm vs. >15 mm), histologic grade (I vs. II and III), and lymph node status (positive or negative) of invasive cancers between fatty and medium dense breasts and between fatty and dense breasts. DCIS was included in analyses solely to study the distribution of histologic type. The distribution of tumor size, histologic grade, and lymph node status by mammographic density categories was studied for invasive cancers only. We used logistic regression to estimate the odds ratio (OR) of tumor characteristics of invasive cancers associated with mammographic density categories. Information about DCIS was not included in regression analysis. Tumor characteristics were the outcome variables. For regression analyses, mammographic density was dichotomized into fatty and medium dense versus dense. We adjusted for age groups (50–54, 55–59, 60–64, and 65–69 years) and screening mode, defined as screen-film mammography (SFM) and full-field digital mammography (FFDM). A total of 5170 invasive breast cancers were diagnosed using SFM, while 2196 were diagnosed with FFDM. All tests were two-sided with a 5% significance level. Statistical analyses were conducted using STATA® software, Version 13.0 (StataMP, StataCorp; College Station, TX, USA).
Results
Histopathologic characteristics of screen-detected breast cancers in the Norwegian Breast Cancer Screening Program, 1996–2010, by mammographic density (fatty, medium dense, and dense breasts).
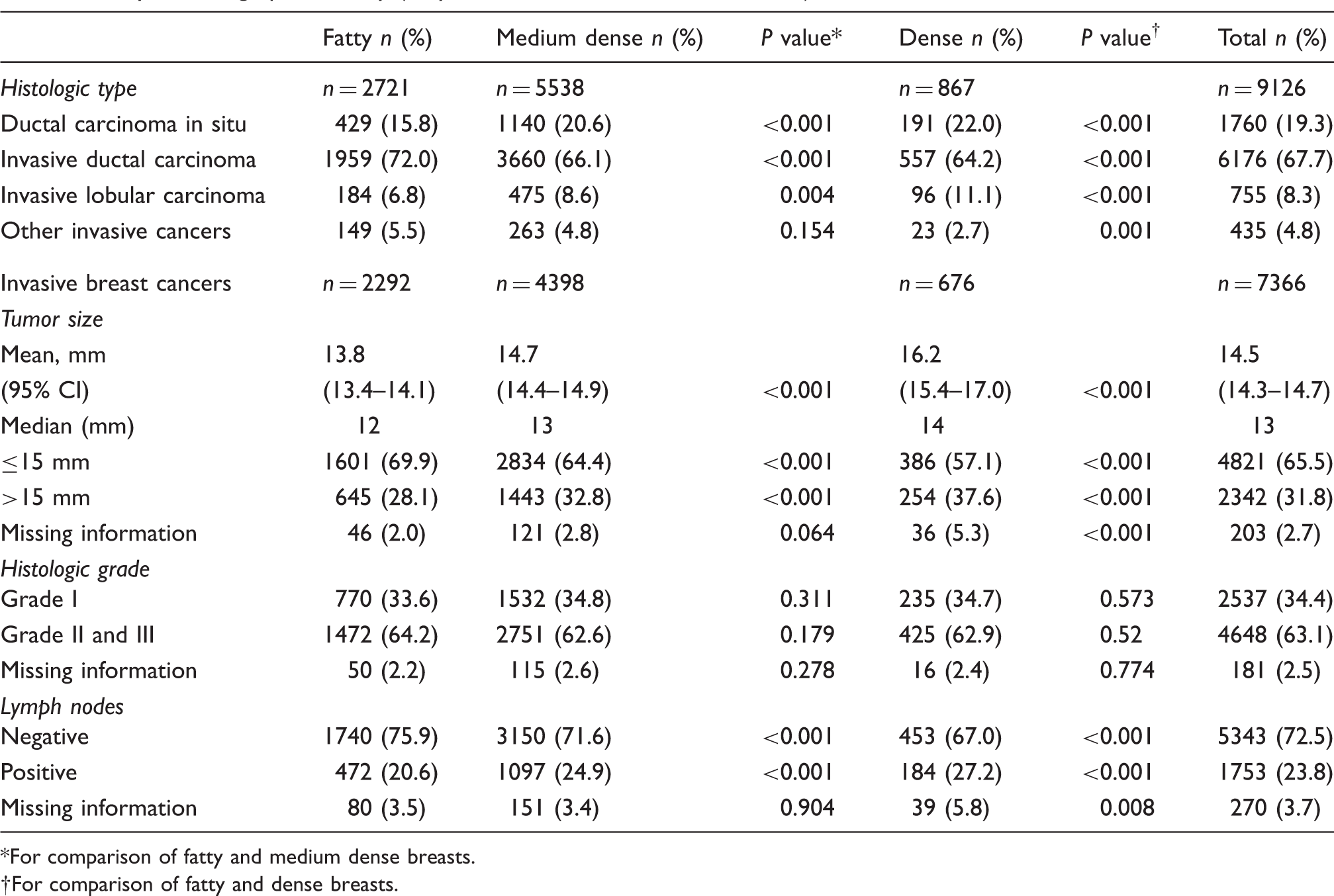
For comparison of fatty and medium dense breasts.
For comparison of fatty and dense breasts.
Discussion
Our study identified an association between mammographic density, tumor size, and lymph node status. The results support the findings from other studies, where various methods were used to classify density (3–7).
Several studies have reported a larger tumor size in dense compared with fatty breasts (3–7). The larger tumor size is associated with masking, which is also related to missed tumors, and thus missed tumors of large size (3,4). Masking decreases the sensitivity of screening programs (1,2). Stratifying women for breast cancer screening by mammographic density and consequently offering additional screening tools for those with dense breasts might be beneficial for those with dense breasts (1,2).
We did not identify any association between mammographic density and histologic grade of the screen-detected tumors. Similar results were reported in a recent study from Sweden (7). However, other studies have reported mammographic density to be either positively (6) or negatively (4,8) associated with histologic grade. A positive association between mammographic density and grade was assumed to reflect a biological relationship between a high amount of breast glandular tissue and a low degree of tumor differentiation (or high histologic grade) (6). A negative association between mammographic density and histopathologic grade was suggested to be related to the tissue microenvironment in fatty breasts, which might be more promoting towards high-grade tumors (7).
Our findings are in contrast with the results from a recent study by Masarwah et al., which reported unfavorable prognostic outcomes among women with very low density when compared with those with mixed or low density (8). The study by Masarwah et al. included a relatively small number of women (n = 270) aged 32–86 years, who were diagnosed with symptomatic breast cancer (8). The results are thus considered not comparable.
This registry-based study included a large number of screen-detected breast cancers with high completeness of data on histopathologic tumor characteristics (less than 5% missing). A limitation of the study is lack of information about body mass index, use of hormonal therapy, and other breast cancer risk factors that could have confounded the association between mammographic density and the outcome variables (11). Another limitation of the study is the subjective three-category classification of mammographic density used in the NBCSP. This classification is different from the commonly used BI-RADS (12). In addition, mammographic density was classified solely in the women recalled for further assessment due to abnormal mammographic findings, non-satisfactory images or clinical symptoms. Thus, we did not have information about the distribution of mammographic density in the screened population.
In conclusion, our findings indicate that high mammographic density among women with screen-detected cancers is positively associated with larger tumor size (>15 mm) and positive lymph node status. Masking by mammographic density might result in less favorable prognosis for the women and a decreased sensitivity of the screening program. Stratifying women for breast cancer screening by mammographic density is a possible approach to reduce the described limitation of mammography as a screening tool.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The study was supported by a grant from the Norwegian Breast Cancer Society, funded by Extrastiftelsen (2013-2-0280).