
Abstract
Background
Only 20% of iliac veins will recanalize on anticoagulation (AC) treatment alone and may, therefore, develop venous obstruction after iliofemoral deep venous thrombosis (DVT). A considerable number of these patients will suffer from post-thrombotic syndrome (PTS) leading to impaired quality of life in more than 50%. Endovascular treatment for iliac vein obstruction using stents is known to alleviate PTS symptoms in selected patients.
Purpose
To report the Danish long-term results of endovascular treatment with iliac stenting.
Material and Methods
From 2000 to 2013 consecutive patients were evaluated and 19 patients with severe venous claudication were identified and subsequently underwent angioplasty and stenting. AC treatment was prescribed for 6 months, and knee-high class II compression stocking recommended for 1 year. Scheduled follow-up was done in the outpatient clinic at 6 weeks, 3 months, and annually thereafter.
Results
Nineteen patients, all women, all with left-sided iliac vein obstruction, and all with severe PTS symptoms were included. The median follow-up time was 81 months (range, 1–146 months; mean, 69 months). Primary patency rate of the inserted iliac stent was 89% (17/19) and 16 patients (84 %) had almost or total symptom relief at follow-up.
Conclusion
Endovascular stenting of iliac obstruction in local anesthesia is minimally invasive and shows excellent long-term outcomes for patients suffering from PTS.
Introduction
The most feared long-term complication of deep venous thrombosis (DVT) is the post-thrombotic syndrome (PTS), which varies widely from 20% to 80% depending on diagnostic criteria, study population, and time from initial deep venous thrombosis (DVT) to assessment of outcome (1,2). Risk factors include location of the DVT and DVT recurrence, gender (1.5 times greater risk for women), obesity, and genetic factors (thrombophilia) (1,2). Only 20% of iliac veins will recanalize on anticoagulation (AC) treatment alone after an iliofemoral DVT leading to PTS for a considerable number of patients (3). PTS symptoms include venous claudication, leg swelling, and venous ulcerations and leads to impaired quality of life in more than 50% of the patients (2,4).
Endovascular treatment with iliac stenting is known to alleviate PTS symptoms in selected groups of patients with partial or complete obstruction of the venous outflow tract. This study reports the Danish long-term results of endovascular treatment with iliac stenting done in local anesthesia.
Material and Methods
The outpatient clinic at Gentofte University Hospital in Copenhagen is a tertiary center that receives referrals of patients with PTS from other Danish venous centers. All patients are evaluated for possible endovascular treatment based on symptoms and clinical and ultrasonic findings. The ultrasound duplex scan is performed with the patient in the standing position (examining the common femoral vein, the femoral vein, the popliteal vein, the great and the small saphenous veins) and in the supine position (examining the iliac veins and the inferior vena cava). Venous computed tomography (CTV) is not done routinely in our set-up, but due to diagnostic challenges in the referring department, two patients had it done.
During 2000–2013 consecutive patients were evaluated and 19 were identified as candidates to subsequently undergo angioplasty and stenting. The patients were checked for coagulation disorders (Factor V Leiden, Protein S and C, Lupus anticoagulans, Homocystein, Antithrombin, and Anti-Cardiolipin) and if found positive, referred to anticoagulation specialists for further treatment.
After ultrasound-guided puncture of the ipsilateral common femoral or popliteal vein, the occluded or stenotic part of the iliac vein was passed with a Terumo guidewire, which was further advanced into the inferior vena cava. An obstruction of more than 50% led to angioplasty and stenting, no pressure gradients were measured. Predilatation of the vein using 6–10 mm balloons and postdilatation using 10–12 mm balloons was done before and after placement of 4–9 cm self-expandable stents. Most procedures were done under local anesthesia alone, but in a few cases intravenous pain medication was needed. Intravenous Heparin (5000 IU) was given during the procedure. The patients were discharged the same day or on the first postoperative day. AC treatment with Warfarin targeting INR in the range of 2.5–3 with bridging of low molecular weight heparin (LMWH) was prescribed for 6 months, and knee-high class II compression stocking was recommended for 1 year. Patients with severe thrombophilia were kept on lifelong AC. Scheduled follow-up was done in the outpatient clinic at 6 weeks, 3 months, and annually thereafter.
To evaluate the patients after the intervention, the Villalta scale was used. The Villalta scale is a validated and reliable clinical classification measuring PTS incorporating the assessment of five subjective (patient-rated) venous symptoms (pain, cramps, heaviness, paresthesia, and pruritus) and six objective (clinical-rated) venous signs (pretibial edema, skin induration, hyperpigmentation, redness, venous ectasia, and pain on calf compression), as well as the presence or absence of ulcer in the DVT-affected leg (5,6). No other classifications were used, but clinical symptoms were noted in the patient charts.
Descriptive statistics on patency and success rates are given. Observation time, age, and follow-up period are reported as mean, median, and ranges.
Results
Patient demographics.
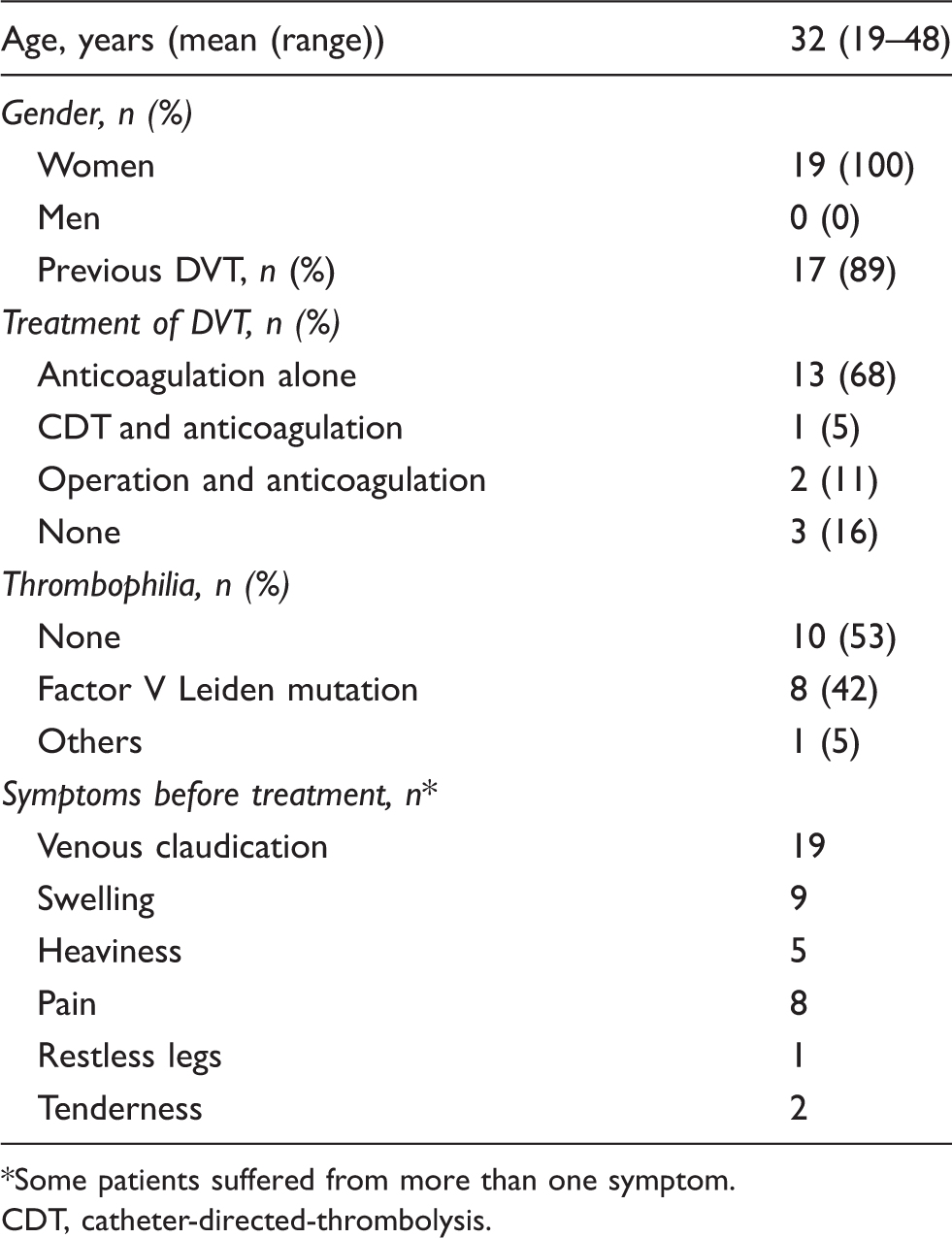
Some patients suffered from more than one symptom.
CDT, catheter-directed-thrombolysis.
Results after endovenous stenting at follow-up.

Some patients suffered from more than one symptom after the intervention.

(a) Iliac stenosis in a woman with venous claudication before treatment. (b) The same patient with the iliac stenosis after angioplasty and insertion of a 14 mm/9 cm Wallstent.
Primary patency rate of the inserted iliac stent was 89% (17/19); however, one patient had a prior stent inserted, and due to a stenosis proximal to that, this intervention was done. The median follow-up time was 81 months (range, 1–146 months; mean, 69 months) (Table 2). One patient had a recurrent full-leg DVT 5 years after the procedure unsuitable for catheter-directed thrombolysis (CDT) or re-stenting leading to moderate PTS (Villalta score of 12). Lifelong AC was initiated due to re-thrombosis. The other patient had a stenotic lesion in the common femoral vein causing the stent to occlude 3 weeks after the intervention leading to light PTS with venous claudication (Villalta scale of 5). The patient was kept on lifelong AC therapy due to Factor V Leiden mutation (heterozygote) and re-DVT.
Ultrasound duplex scan at follow-up is shown in Table 2. Reflux or obstruction was observed in five patients (two from the popliteal to the common femoral vein, two in the popliteal vein, and one in the femoral vein), 10 patients had no reflux in the deep system of the lower extremity (of those, two had greater saphenous vein reflux, one had smaller saphenous vein reflux), and four patients had scarring and thickening of the vein wall (one in the common femoral vein, two in the femoral vein, and one in the popliteal vein). Sixteen patients (84%) had total or almost total symptom relief at follow-up (Table 2). Three patients still suffered from light PTS; however, all reported that stenting had improved their symptoms considerably, apart from those two whose stents occluded.
Discussion
After an iliofemoral DVT a considerable number of patients will suffer from PTS leading to impaired quality of life. Furthermore PTS increases healthcare costs. Treatment success of established PTS relies on patient education and use of compression therapy (7); however, compliance can be poor, and in patients with severe PTS, conservative treatment may have little effect. Stenting in the iliofemoral venous segment for chronic venous disease was first described in 1985 (8). A large study of 447 limbs treated with stenting documented the importance of reducing venous outflow obstruction for the prevention of chronic venous insufficiency (CVI) (9). Several studies have shown stenting to be safe, with high patency rates, low rate of in-stent restenosis, and little need for re-intervention (10–12).
No specific criteria of when to perform angioplasty and stenting of an obstructive lesion exist in the literature. An iliac stenosis with a direct pressure gradient of 5 mmHg or higher suggests a hemodynamic significant stenosis and may indicate relieve of symptoms after stenting (13). Hemodynamic measurements are, however, poorly related to clinical status (14) and other methods such as IVUS, may give additive information about the degree of the stenosis (14). Morphological obstruction of 50% or higher has arbitrarily been chosen as a criteria for angioplasty and stenting (15).
Patency rate in this study was 89%, which is comparable to rates reported in previous studies (16–20). Patency rate mainly depends on the number of lesions needing recanalization, and if the common femoral vein is involved in the obstructive lesion (21). Patency rates are lower in cases with involvement of the common femoral vein. The main part of the patients in this study demonstrated no significant obstructions of the common femoral vein prior to endovascular treatment; however, three patients were stented to the very proximal part of the common femoral vein. Neglén et al. suggested that patency rates rely on the etiology (previous thrombosis is more common in patients with obstructive lesions in the common femoral vein), and emphasizes the importance of covering the entire obstructive lesion, and if needed, to stent below the inguinal ligament (11).
The iliac compression syndrome was described by May and Thurner (22) and by Cockett (23) and is a localized external compression of the vein narrowing the lumen by adjacent arteries. This appears most often on the left side, and in 24% of the “normal” population it leads to a 50% lumen reduction and in 66% it leads to a 25% lumen reduction (24). Furthermore, this is more common in women (25). Keeping in mind that our study population is very small, this may explain why all our patients were female and all the obstructions were located on the left side.
To suggest a randomized controlled study comparing conservative treatment to endovascular treatment in patients suffering from PTS due to iliac obstruction seems unethical and unfeasible. Both safety and efficacy of the angioplasty and stenting is high, and the clinical results are excellent, reducing PTS symptoms and hence the health costs in most of the patients. However, only dedicated centers should perform the endovascular procedures in selected patients. Patients with iliofemoral venous obstruction and moderate to severe PTS symptoms should, in our opinion, be offered angioplasty and stenting.
Future challenges in the treatment and care of PTS/CVI are: first, to acknowledge the fact that effective treatments exist; and second, to ensure, that potential candidates for endovascular treatment are referred to dedicated centers, that have experience and a proper set-up, so patients can be offered a variety of up-to-date surgical and endovascular high-quality treatment options.
In conclusion, PTS is the most severe long-term complication after DVT leading to impaired quality of life for a considerable number of patients suffering from venous claudication, pain, venous stasis dermatitis, edema, or ulcers. The Danish experience with angioplasty and stenting of iliac vein obstruction in local anesthesia seems to be safe and effective in this small group of selected patients suffering from severe PTS. The procedure is minimally invasive and shows excellent long-term outcomes.
Footnotes
Conflict of interest
None declared.