
Abstract
Psoriatic arthritis mutilans (PAM) is the most severe and rare form of psoriatic arthritis (PsA). We describe radiological development in a typical case of PAM covering three decades in order to elucidate the need for early diagnosis of PAM. Radiographs of hands and feet, taken from 1981 to 2010, were evaluated using the Psoriatic Arthritis Ratingen Score (PARS). When PsA was diagnosed, in 1981, gross deformity was observed in the second PIP joint of the left foot. Several pencil-in-cup deformities and gross osteolysis were present in the feet in the first decade of the disease. Over 10 years, many joints had reached maximum scores. During the follow-up, other joints became involved and the disease developed clinically. Reporting early signs suggestive of PAM, e.g. pencil-in cup deformities and gross osteolysis in any joint, should be mandatory and crucial. This would heighten our awareness of PAM, accelerate the diagnosis, and lead to improved effective treatment in order to minimize joint damages resulting in PAM.
Introduction
Psoriatic arthritis mutilans (PAM) is the most severe form of the five clinical presentations of psoriatic arthritis (PsA) described by Moll and Wright (1). The clinical manifestation of the condition is shortening of a digit due to gross osteolysis, resulting in the so-called “opera glass finger”, “telescopic finger”, or “doigt en lorgnette”. Previously published studies on this condition have used different definitions of PAM, as no international classification criteria are yet to be found in the literature. However, radiographic features have been found to be more sensitive than clinical findings (2). Recently, attempts have been made on the initiative of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) in order to develop a consensus definition of PAM, but these have not yet been globally accepted (2).
The reported prevalence of PAM varies considerably, in the range of 1–21% of patients with PsA (3–6). In the Nordic countries, the prevalence was found to be only about four cases per 1,000,000 inhabitants (3.7; 95% CI 2.8–4.6) in a multinational population-based study recently published by the Nordic PAM Study Group (7).
Radiographic evaluation is helpful and conventional radiographs are the most commonly used radiological tool. The radiographic features of PsA are well known, including joint destruction, inter-joint space narrowing, bony proliferation, periostitis, osteolysis, including pencil-in-cup deformity, and ankylosis. Any or all of these radiological changes may be present in one and the same patient. Involvement of the distal interphalangeal joints of the fingers is typical (8). Osteolysis is the defining feature of PAM and there is consensus (according to GRAPPA) that involvement of a single joint is sufficient to establish the diagnosis of PAM (2,9).
In this case report we present the radiographic findings of an almost 30-year follow-up in a patient afflicted by PAM.
Case report
The patient gave his written informed consent for this case presentation. The Bioethics and Data Protection Committees in all four countries approved the study protocol for the Nordic PAM study.
The patient was a 58-year-old man with a 34-year history of psoriasis. Serological tests showed that he was HLA-B27 positive and had a low titer of antinuclear antibodies (ANA) (1/200), though rheumatoid factor (RF) and anti-cyclic citrullinated peptide antibodies (ACPA) proved negative. Polyarthritis was reported at the age of 25 years. As psoriasis had been diagnosed 1 year prior to the appearance of joint symptoms, a diagnosis of PsA was made. During the first 10 years the patient was treated with NSAIDs, and in 1988, 9 years after PsA diagnosis, he was prescribed sulphasalazine, by which time dactylitis had affected all fingers. However, due to adverse reactions, this treatment was discontinued only a few months later. After 4 more years of NSAID treatment, methotrexate was initiated, first at a low dose combined with numerous local steroid injections. Later the patient accepted a methotrexate dosage of 12.5 mg/week. Since 2001 he has been treated with a TNF-α inhibitor (infliximab) combined with methotrexate. Between 1979 and 2001 he suffered from active polyarthritis with increased ESR and CRP values, but since the initiation of TNF-α inhibitor therapy the joints have not been inflamed and the ESR and CRP values have both been within the reference range. The diagnosis of PAM was first established in this patient's record in 1997, 18 years after the PsA diagnosis.
Psoriatic Arthritis Ratingen Scores of a patient with psoriatic arthritis mutilans in hands and feet visualized in serial radiographs from 1981 through 2010.

DS, destruction score; PR, progression rate; PS, proliferation score; Total, total score.
In the PARS scoring method, pedal PIP and DIP joints are not rated at all. In the current case, pedal IP joints were noted separately. As early as 1981 gross deformity was observed in the second PIP joint of the left foot. Pencil-in-cup deformities and gross osteolysis were present in two pedal PIP and DIP joints at the 1988 examination (Fig. 1a–d). Plantar enthesophytes were observed already at the first examination but did not progress over time. Fig. 2 shows typical dactylitic changes in the third finger of the left hand.
Serial radiographs from 1981 (a), 1988 (b), 2001 (c) through 2010 (d), showing typical changes of psoriatic arthritis mutilans in the left foot of a 58-year-old male patient. Development in chronic dactylitis of the third finger of the left hand in the reported case.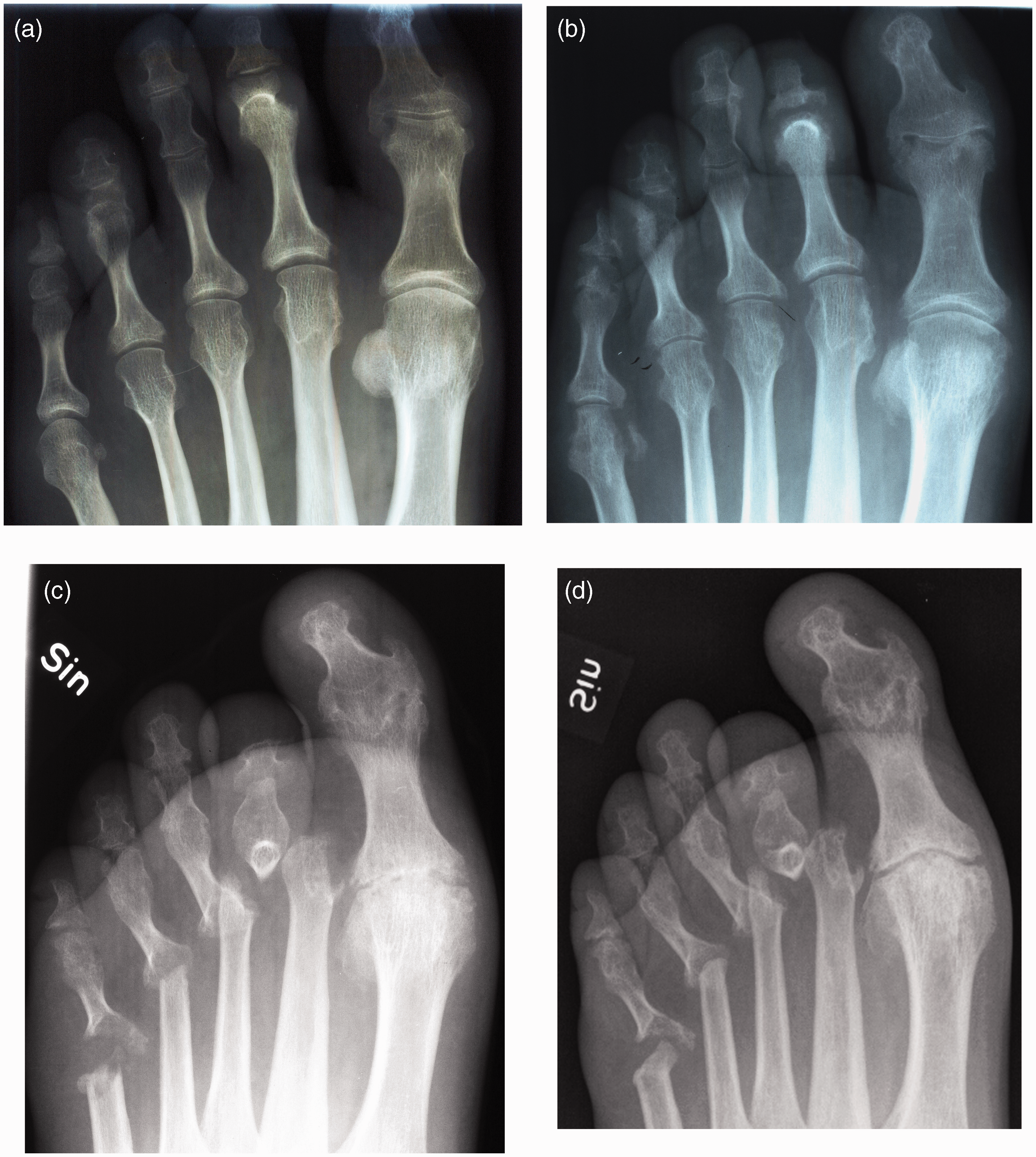

Discussion
This case report presents the natural course of events in a patient suffering from PsA, developing to PAM, untreated for decades. The clinical pattern of PsA often changes during the course of disease, as does the radiological pattern, and both need to be taken into clinical consideration (11). Had the radiological pattern of PAM been included, the diagnosis could have been made as early as in 1988, or 9 years previously, i.e. instead of 1997 when the diagnosis of PAM was first mentioned.
It is important to include all proximal and distal joints of hands and feet in a patient’s PsA assessment. In the present case the most severe progression was seen in the feet, even during the first decade of disease. Progression of the PIP joint changes was pronounced. Inclusion of the pedal PIP and DIP joints in radiographic scores might be of advantage, but the assessment of these joints is difficult on conventional radiographs for technical reasons, i.e. because of overlapping structures. However, the radiologist should report any sign suggesting PAM, such as gross osteolysis and pencil-in-cup deformities in any joint, and thus alert the clinician of a likely diagnosis of PAM.
The degree of destruction in PsA can be demonstrated by using a scoring system, as used in clinical trials. Feasibility, reliability, and sensitivity to change have been evaluated for four different radiographic scoring methods in 50 patients with PsA (12). Two assessors rated the radiographs by modified Steinbrocker scoring (STB), modified Sharp scoring (MSS), the modified Sharp–van der Heijde method (SvdH) and Psoriatic Arthritis Ratingen scoring (PARS). The SvdH method proved the most reliable and sensitive to changes, but took longest to perform by the observer. The PARS method, initially developed for PsA, was close to the SvdH and much quicker to perform. The smallest detectable changes were 2.9% (STB), 2.1% (MSS), 1.4% (SvdH), and 1.2% (PARS). PARS was therefore chosen to assess the progression of destruction in the present case. However, none of these methods include special scoring for mutilans changes; nor do they take pedal PIP and DIP joints into account.
There are relatively few published studies where radiographic scoring methods were applied to assess the progression of PsA. Ravindran et al. (13) studied 139 patients with established PsA and a median follow-up of 5.7 years, using the MSS. Their median progression score was +1.08 units/year. They found a close correlation between MSS and clinical joint scores, and other characteristic radiographic features of PsA. In the present case, with a follow-up of 29 years, the most rapid progression was seen early in the disease course, i.e. during the first decade, after which the radiological progress declined. Thus, prompt radiological assessment of patients with early PsA is mandatory. Importantly, many joints had, after only 10 years, reached maximum scores, although the joint damage still showed progression in the subsequent years, though fewer additional joints were then involved. Thus, the treatment with an TNF-α inhibitor in this present case may have slowed the progression of joint destruction (14).
In conclusion, awareness of any radiological sign of mutilans joint damage in PsA may lead to early recognition of PAM, to be followed by early aggressive treatment which may prevent severe joint destruction of the mutilans type seen in patients affected by PsA. Radiographic scoring methods can be used to assess progression in PsA but need to be further developed for assessment of PAM.
Footnotes
Acknowledgements
We thank NORDPSO for support of the Nordic PAM study.
Conflict of interest
None declared.
Funding
NORDPSO arranged and secured funding for the Nordic Psoriatic Arthritis Mutilans study.