
Abstract
A 7-year-old Japanese girl who had undergone living-donor liver transplantation (LT) at the age of 10 months for decompensated liver cirrhosis caused by biliary atresia presented with recurrent episodes of obscure gastrointestinal bleeding (GIB) with anemia. Over the following 6 years, she experienced five episodes of GIB requiring hospitalization. Subsequent evaluations including repeat esophagogastroduodenoscopy (EGD), colonoscopy (CS), contrast-enhanced computed tomography (CT), and Meckel’s scan all failed to reveal a bleeding source. However, varices at the site of hepaticojejunostomy were detected on abdominal ultrasonography and magnetic resonance angiography (MRA) at the age of 7 years. MRA might be more helpful than contrast-enhanced CT for identifying such bleeding.
Introduction
To date, descriptions of late-onset gastrointestinal bleeding (GIB) after liver transplantation (LT) have been limited, and the incidence, etiology, and timing of this situation remain poorly described. The focus of previous reports has mainly been on GIB immediately after LT, typically due to ulcers and postoperative Roux-en-Y bleeding (1). However, a few reports have noted patients with obscure GIB and portal hypertension who showed ectopic collaterals between the portal and systemic circulations (2,3). In cases of GIB occurring beyond the immediate post-LT period, ectopic varices represent an uncommon cause of GIB, accounting for up to 5% of cases of variceal bleeding (2). Generally, contrast-enhanced computed tomography (CT) has been suggested as a useful modality to diagnose extrahepatic disorders, including varicose veins after LT (4). The purpose of this report was to present findings of varices at the site of hepaticojejunostomy in a post-LT pediatric patient that remained undetected on contrast-enhanced CT, but were revealed on magnetic resonance angiography (MRA) and ultrasonography (USG).
Case report
A 7-year-old Japanese girl presented with melena and anemia. She had undergone segmental living-donor LT with Roux-en-Y biliary reconstruction at the age of 10 months. No significant abnormalities were apparent from her family history. She suffered from jaundice and pale stools after birth. At the age of 4 weeks, biliary atresia was diagnosed and Kasai portoenterostomy was performed. At the age of 10 months, segmental LT with her father as donor was performed using a Roux-en-Y biliary reconstruction. At the age of 19 months, she was admitted to our institution with the first episode of GIB and severe anemia. Esophagogastroduodenoscopy (EGD), colonoscopy (CS), and contrast-enhanced CT were performed, but only detected esophageal varices that were not involved as a source of bleeding. Symptoms subsided without any specific treatment. Similar episodes of GIB and anemia subsequently occurred at the ages of 21, 68, 82, and 86 months. No clear sources of bleeding or collaterals were identified on repeated EGD, CS, or contrast-enhanced CT. Meckel’s diverticulum was ruled out on Meckel’s scan. Intestinal histology showed no findings of graft-versus-host disease. At the age of 88 months, she was re-admitted to our institute for a sixth episode of GIB. Laboratory examinations revealed decreases in hemoglobin (5.8 g/dL), hematocrit (19.5%), serum iron (18 µg/dL), and ferritin (8 ng/mL). Results for clotting function tests were within normal ranges. EGD and CS revealed normal colonic mucosa with normal histological findings. Again, no obvious sources of bleeding were apparent. Contrast-enhanced CT still showed no bleeding sources or collaterals (Fig. 1). While no dilation, stenosis, or occlusion of the intrahepatic portal veins was found, multiple varices were confirmed in the mucosal lumen of the hepaticojejunostomy, positioned at the lower surface of the liver graft, on abdominal USG and MRA (Figs. 2 and 3). We were therefore initially planning to administer β-blockers to reduce portal hypertension. However, as no episodes of bleeding have been encountered after the sixth episode, we have strictly continued follow-up without medications. At 111 months old, regression of multiple varices was detected on MRA, indicating that sufficient collateral venous circulation may have developed.
Findings on contrast-enhanced computed tomography (CT) at the sixth episode of gastrointestinal bleeding (GIB). Contrast-enhanced CT showed no marked bleeding sources or collaterals. Findings of abdominal USG at the sixth episode of GIB. Varices were identified in the lumen at the site of hepaticojejunostomy. Arrows indicate varices. Arrowheads indicate liver graft. The findings of abdominal 2D phase contrast MRA at the sixth episode of GIB. Varices were identified at the site of hepaticojejunostomy. Arrows indicate varices of hepaticojejunostomy.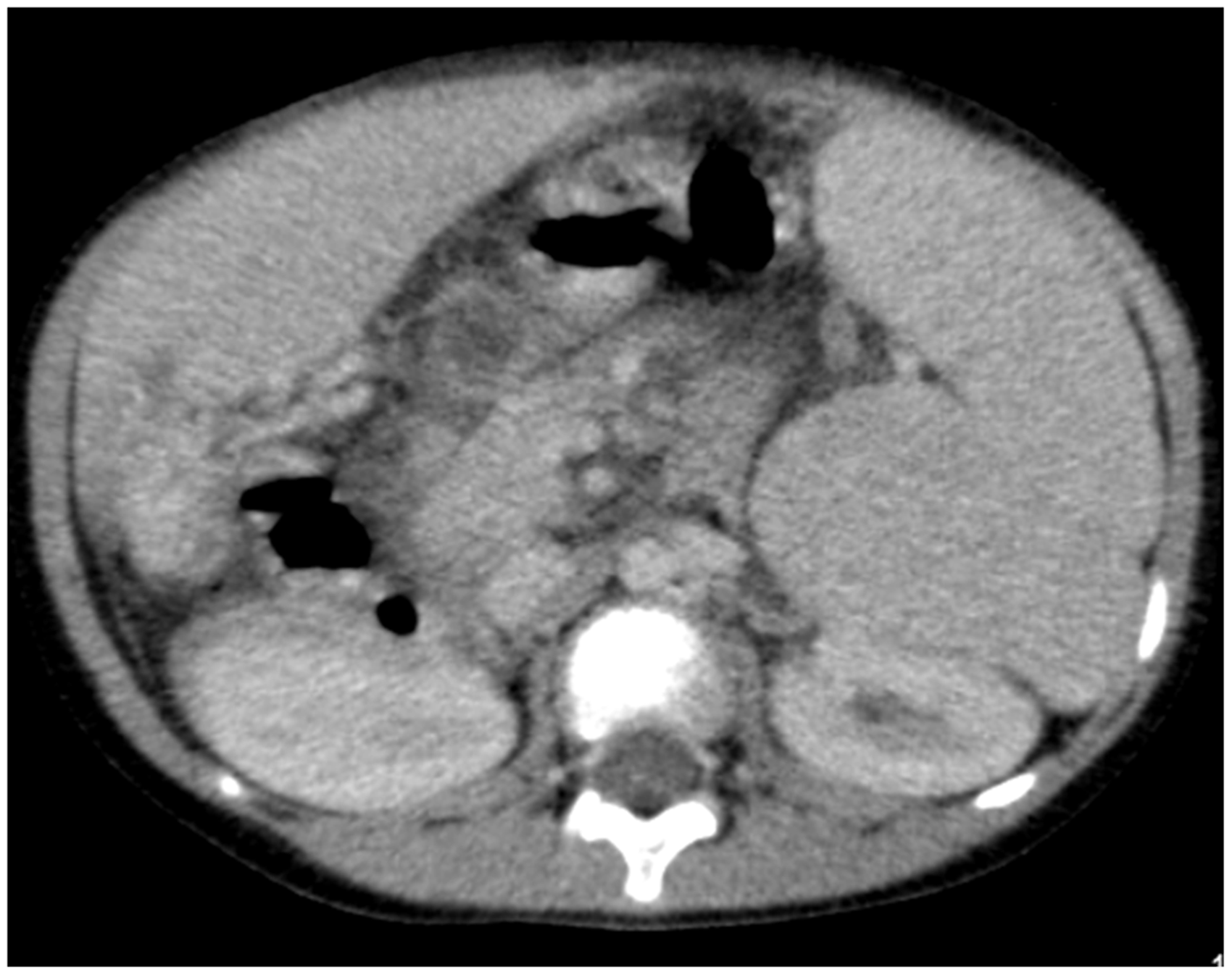


Discussion
According to the criteria of the American Gastroenterological Association, obscure bleeding is defined as bleeding from the gastrointestinal tract that persists or recurs without any obvious etiology after EGD, CS, and radiological evaluation of the small intestine (5). The bleeding source is not identified in 10–20% of adult GIB patients. Despite several evaluations with EGD, CS, and single- or double-balloon endoscopy, identification of obscure GIB is often difficult (6). In children, reports of obscure GIB post-LT have been limited. The etiology of GIB immediately after LT appears mostly attributable to ulcers, enteritis, and Roux-en-Y bleeding (1). On the other hand, a retrospective study of 156 post-LT patients that focused on portal hypertension and ectopic varices beyond the immediate post-LT period identified three children with GIB at the Roux-en-Y anastomosis. Several etiologies of late-onset portal hypertension were identified, such as post-LT portal vein stenosis, cirrhosis secondary to chronic rejection, and hepatic arterioportal fistula (6). In the present case, varices represented portal venous collaterals, and neither portal vein stenosis and occlusion nor hepatic arterioportal vein fistula were identified on ultrasonography or contrast-enhanced CT. In addition, chronic rejection of the liver graft appeared unlikely, because there was no evidence of elevated transaminases or cholestasis in serological analysis. Ling et al. reported on complications of child portal hypertension, with 44% of patients showing splenomegaly, ascites in 4%, and portal systemic collaterals in 14%. Portal hypertension did not represent a risk factor for GIB within 1 year after LT, but GIB had developed in 6% patients by last follow-up (median, 4.3-year post-LT) (7). In this case, latent portal hypertension after LT appeared involved in the development of varices at the site of hepatojejunostomy because ascites, splenomegaly, and mild esophageal varices were identified on abdominal USG and EGD at the time of the sixth admission.
There is currently no diagnostic gold standard for ectopic varices, because large randomized controlled studies have yet to be undertaken. Use of several imaging modalities, including USG, CT, MRA, and double-balloon enteroscopy (DBE), is important when evaluating varices. In particular, contrast-enhanced CT has been suggested as the primary imaging modality for evaluating extrahepatic disorders including varicose veins in pediatric patients after partial LT (4,8). However, despite undergoing contrast-enhanced CT on multiple occasions, varices at the site of hepaticojejunostomy were not identified in this case. Several possibilities might explain this inability to visualize varices on multiple contrast-enhanced CT. First, the timing of attempts to identify varices using contrast media did not match the timing of contrasting of varices. Second, contrasted varices might have been masked by the adjacent intestinal tract, which showed similar density to the contrasted varices. MRA, on the other hand, allowed selective suppression of the intensity of the adjacent gastrointestinal tract. Meanwhile, DBE has already been described as having huge diagnostic potential for Roux-en-Y loop varices in children with liver transplantation (6). In this case, we explored the option of DBE for visualizing and treating varices at the Roux-en-Y anastomosis, but could not perform DBE because the varices were located substantially above the sutures on MRA. We therefore determined that execution of DBE would have been overly difficult, because experience with pediatric DBE in our institute remains limited. MRA may thus be preferable for children, given the risks of the alternatives, including radiation exposure and allergy to iodine in contrast-enhanced CT and the physical and technical difficulties of DBE.
In conclusion, when obscure and recurrent GIB occurs during the late period after LT, varices at the site of hepaticojejunostomy should be considered as an important differential diagnosis. In pediatric cases where varices are not identifiable from serial contrast-enhanced CT, MRA could be more useful than contrast-enhanced CT in the identification of varices at the site of hepaticojejunostomy.
Footnotes
Conflict of interest
None declared.