
Abstract
Older individuals within residential care (RC) may have palliative care needs that intensify along the path of their illness to death. An end-of-life (EOL) conversation follows when transitioning from one care to another, to plan for future care, to consider the patient's wishes, and to avoid unnecessary suffering for both patient and family. The aim of this study was to describe registered nurses’ (RNs) experiences of EOL conversations when transitioning to EOL care in RC. The design of this study was a survey study with questionnaire data from RNs working in RC (n = 71), analyzed with descriptive statistics and using qualitative content analysis. This study is reported in accordance with the COREQ checklist. Three main categories and seven subcategories were identified. The first category was ‘Deficiencies in EOL conversations’ with the subcategories ‘EOL conversations at too late a stage’ and ‘Physicians’ absence in collaboration concerning EOL conversations’. The second category was ‘Nurse’s role in EOL conversations’ with the subcategories ‘Initiate EOL conversations’, ‘Cohesive link between stakeholders concerning EOL conversations’, and ‘Carry out EOL conversations’. The third category was ‘Family involvement in end of life’ with the subcategories ‘Family members’ participation in EOL conversation’ and ‘Unrealistic expectations at EOL conversation’. RNs at RC take a great responsibility regarding EOL conversations by often both initiating and carrying out the conversations. Such conversations need to be initiated at an early stage to enable patients to receive information or express their own wishes, and to have time to create good relationships with family members so they feel informed and involved.
Introduction
The aim of the present study was to describe registered nurses’ (RNs) experiences of end-of-life (EOL) conversations when transitioning to EOL in residential care (RC). An exploration of this question, specifically in relation to nursing, is important in this growing field of home care. We already know that demographic change means more and more people will live to an older age and need care measures.1–3 Older people often live the last part of life in RC, including palliative care. Death and dying are a natural part of life and palliative care aims to meet a person's physical, psychological, social, spiritual, and existential needs, as well as alleviating suffering regardless of how it arose or expressed itself. 4 Palliative care for older individuals is challenging as they often have a complex and unpredictable disease profiles, with many experiencing cognitive impairment. Communication skills are also affected towards the end of life. This affects the patients’ ability to make decisions and to process the information they receive about their illness and care. 5 To provide the best care possible at the end of life, conversations should be held where the individual's wishes can be expressed and the care can be planned in the best possible way until, and after, death. 4 International research already supports shared decision-making in navigating the complex balance between prolonging life and prolonging death, taking into account the perspectives of clinicians, patients, and their families’ preferences at the end of life. 6 Through this, many of the ethical dilemmas in EOL care can also be avoided. 7 This study can add knowledge about the RNs’ perspective in this situation to make it even more complete and professional.
The EOL conversation is a common concept referring to discussions between professionals, patients, and family members, sometimes referred to as EOL discussions or communications. These are related to Advanced Care Planning 8 and shared decision-making, and play a critical role in organization of the care. 9 The difference between the terms lies in their timing: the EOL conversation occurs when the direction of care changes based on the patient’s medical condition or the person is approaching the end of life, while Advanced Care Planning is conducted at an earlier stage to discuss the person's wishes before the EOL phase begins. The responsibility for carrying out the EOL conversation varies. In Sweden, the National Board of Health and Welfare strongly recommends EOL conversations in palliative care and intends for the EOL conversation to be a discussion between the physician responsible for the patient’s care and the patient, focusing on the decision to switch to palliative care at the end of life. 10
EOL conversations play a critical role in patients’ awareness of their disease and prognosis and help them participate in decisions regarding their own EOL care. 11 At the same time, these conversations have the potential to gather information about the resident's wishes for their care at the end of life. 12 This type of conversation leads to the implementation of more palliative care measures, increased adherence to patients’ wishes, and fewer life-sustaining measures, making it a vital component of high-quality palliative care.13–15 EOL conversations promote palliative care for older individuals living in RC, 16 and these conversations should ideally start at an early stage of the disease or when a patient moves into RC. Open EOL communication can positively impact medical, psychological, and relational outcomes during the dying process for patient and family. 17 Even though EOL conversations are a highly recommended measure in palliative care, many older people are not offered them.18–20 In RC in Sweden, in 2019–2020, 76% of individuals aged older than 65 years had such conversations before their death despite that being death expected. 21 Factors that influence the lack of EOL conversations between physicians and patients at the end of life, despite existing guidelines and efforts to implement them, including physicians’ feelings that they lack competence in conducting such conversations. 8 Studies show that RNs recognize that communication about changes in therapies often take place post facto. 12 The presence of cognitive impairment, such as dementia, stroke, old age, or when patients have already lost their decision-making capacity are factors. 22 If the patient lives in RC and is already receiving treatment for their issues, this is also a factor that can affect these EOL conversations.
RNs can serve as both advocates and emotional pillars for patients and their family, acting as intermediaries between the patient, the family, and physicians in the context of RC.15,23 RNs are also often the ones who make most decisions regarding the care of older individuals. 24 A lack of common language between different professions can cause uncertainty in contexts involving death and dying, 25 which are natural aspects of caring for older individuals. In addition to providing skilled care, RNs caring for older and dying individuals have a major responsibility for maintaining continuous dialogue with these patients, which requires expert communication skills. 14 Education, experience, and competence are thereby of considerable importance as starting points for RNs to be able to participate and contribute to discussions about information, planning, and decisions at the end of life.23,26 Even though EOL conversations are highly recommended during transitions when care changes direction, a considerable proportion of people aged ≥65 years in RC have not had a documented EOL conversation before their death, even though the death was anticipated. RNs have a fundamental role in care. By describing their experiences with EOL conversations within RC, specific prerequisites and challenges in this context might be clarified, thereby increasing knowledge about EOL conversations.
Design
This qualitative survey was conducted via a web-based questionnaire with open-ended and closed items. The data were analyzed using qualitative content by Elo and Kyngäs (2008). 27 This study follows the COnsolidated criteria for REporting Qualitative research (COREQ) checklist. 28
Context and participants
In Sweden, municipalities are obliged to provide permanent housing for older individuals (age ≥65 years) who need round-the-clock care due to an untenable home situation. 29 Further, they are obliged to offer good healthcare for older individuals living in RC. 30 Medical treatment in RC by physicians, however, is provided by the regions through an agreement. 31 The inclusion criteria for this study were RNs in current employment or having previous experience of working in RC for older individuals and with experience of EOL conversations. No further inclusion criteria were set.
Data collection
In October 2021, a web-based questionnaire was posted on a Facebook group named “Registered nurse” (in Swedish: Sjuksköterska). This group had 35,000 members at the time. The questionnaire had substantially open-ended questions, was constructed using Office 365 Forms, and was based on previous research, policy documents, and the authors’ experiences of EOL conversations. The questionnaire contained information about the study and the first question confirmed the participant's consent (Appendix 1). A pilot study with five RNs was conducted, resulting in certain questions being clarified. Data collection ended when we judged that the richness of the collected data was sufficient to address the study’s aim. A total of 81 RNs answered the questionnaire; of them, 71 met the inclusion criteria for the study. These 71 RNs answered the open-ended questions, spanning 19 written pages.
Data analysis
Statistical analyses were conducted using Excel to present background characteristics and conditions related to EOL conversations within RC. All participants answered all open-ended questions. Before analysis, each participant's responses were compiled into a cohesive text to ensure that no individual statement would influence the results. In three of the five free-text questions, RNs’ experiences were specifically requested (Appendix 1). The other two free-text questions are also based on the RNs’ experiences, focusing on how they approach the EOL conversations and their role in these discussions, rather than strictly adhering to local guidelines. The data from open-ended questions were analyzed through qualitative content analysis in three phases using an inductive approach, as outlined by Elo and Kyngäs. 27 In the preparatory phase, the data were read several times to achieve a deeper understanding and to gain an overall perspective. In the organization phase, the meaning-bearing parts of the data—i.e., the text consisting of sentences or longer paragraphs relevant to the aim of the study—were identified through open coding. This involving segmenting the data into meaningful expressions, which included describing annotations using a word or a short sequence. Based on these expressions, headings were created. The headings on an overall level were merged, and subcategories and categories were created. In the final phase, the reporting phase, the results were presented in three identified categories and seven subcategories, which synthesized the findings.
Ethical considerations
Approval for the study was obtained through the ethical board at Mälardalen University, Sweden (Dr nr 2023/2430). The RNs invited to the study were informed that participation was voluntary and that the information collected would be handled in such a way as to ensure that only authorized individuals have access to it. Additional ethical aspects were considered in line with the Declaration of the World Medical Association in Helsinki 32 and the Swedish Data Protection Agency GDPR (General Data Protection Regulation). 33 To protect the participants, a joint decision was made to anonymize the data and collect minimal personal information, as it was not possible to withdraw consent.
Throughout the analysis process, ethical discussions were held between the authors and with fellow researchers at the lab, as there was a risk that both the data collection and results might be influenced by the author's own pre-understanding and clinical experience as RNs within palliative care.
Results
Most of the RNs (n = 57, 80.3%) were employed in RC for older individuals, and a half of them (50.9%) had worked as RNs for 6 years or more (Table 1). Among those with previous employment at RC, a majority (78.5%) had worked as RNs for 6 years or more. Most of the RNs reported that EOL conversations were initiated by the RNs (RNs in current employment at RC: 86.0%; RNs in previous employment at RC: 64.3%), and approximately half reported that physicians participated in EOL conversations (RNs in current employment at RC: 50.9%; RNs in previous employment at RC: 50.0%).
The categories and subcategories identified in the analysis describing RNs’ experiences of EOL conversations when transitioning to EOL care in RC for older individuals are presented in Figure 1.
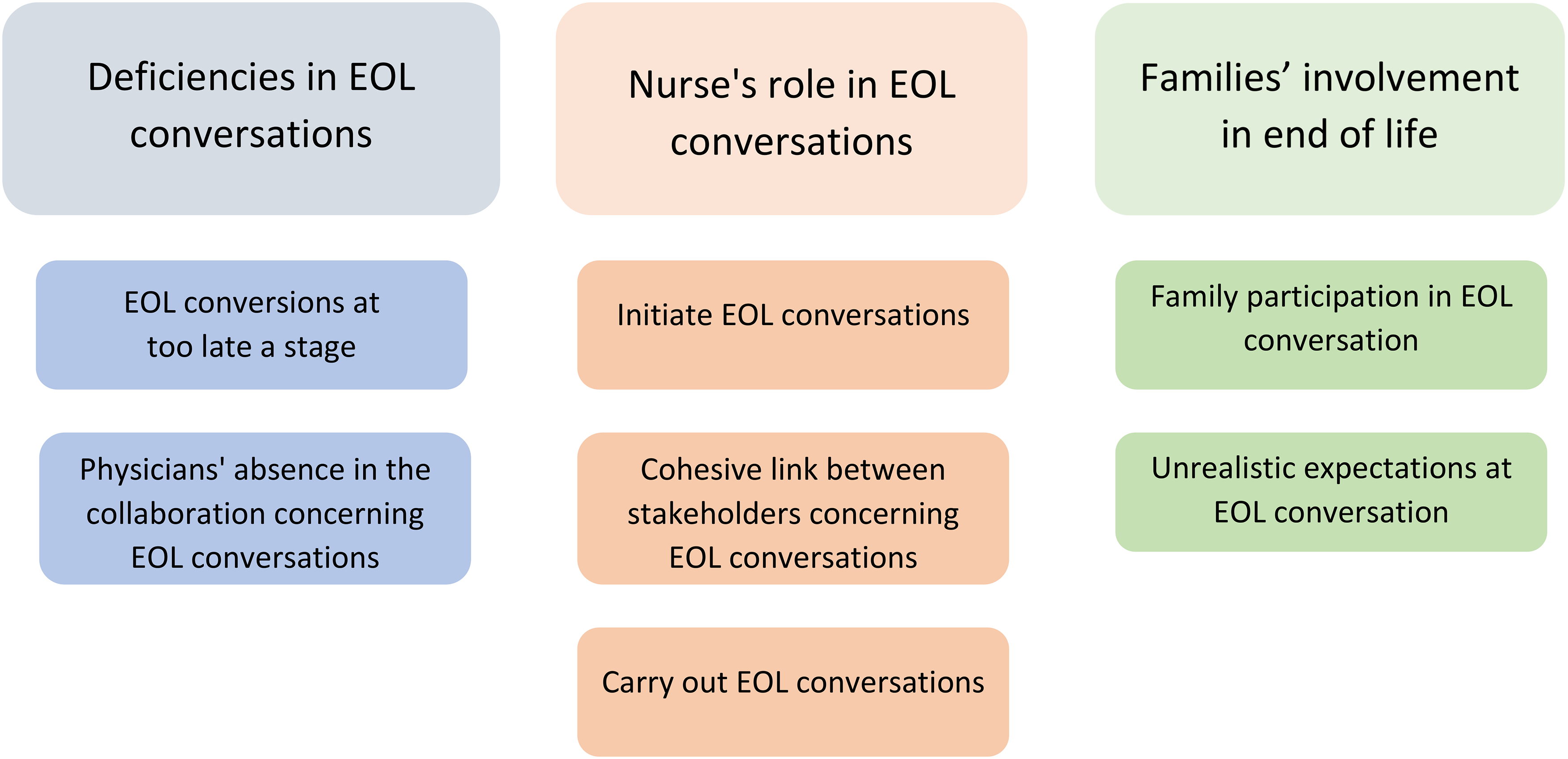
The categories and subcategories identified in the analysis describing registered nurses’ experiences of end-of-life (EOL) conversations when transitioning to EOL care in residential care (RC) for older individuals.
Background information regarding RNs, and their experiences of EOL conversations in RC.
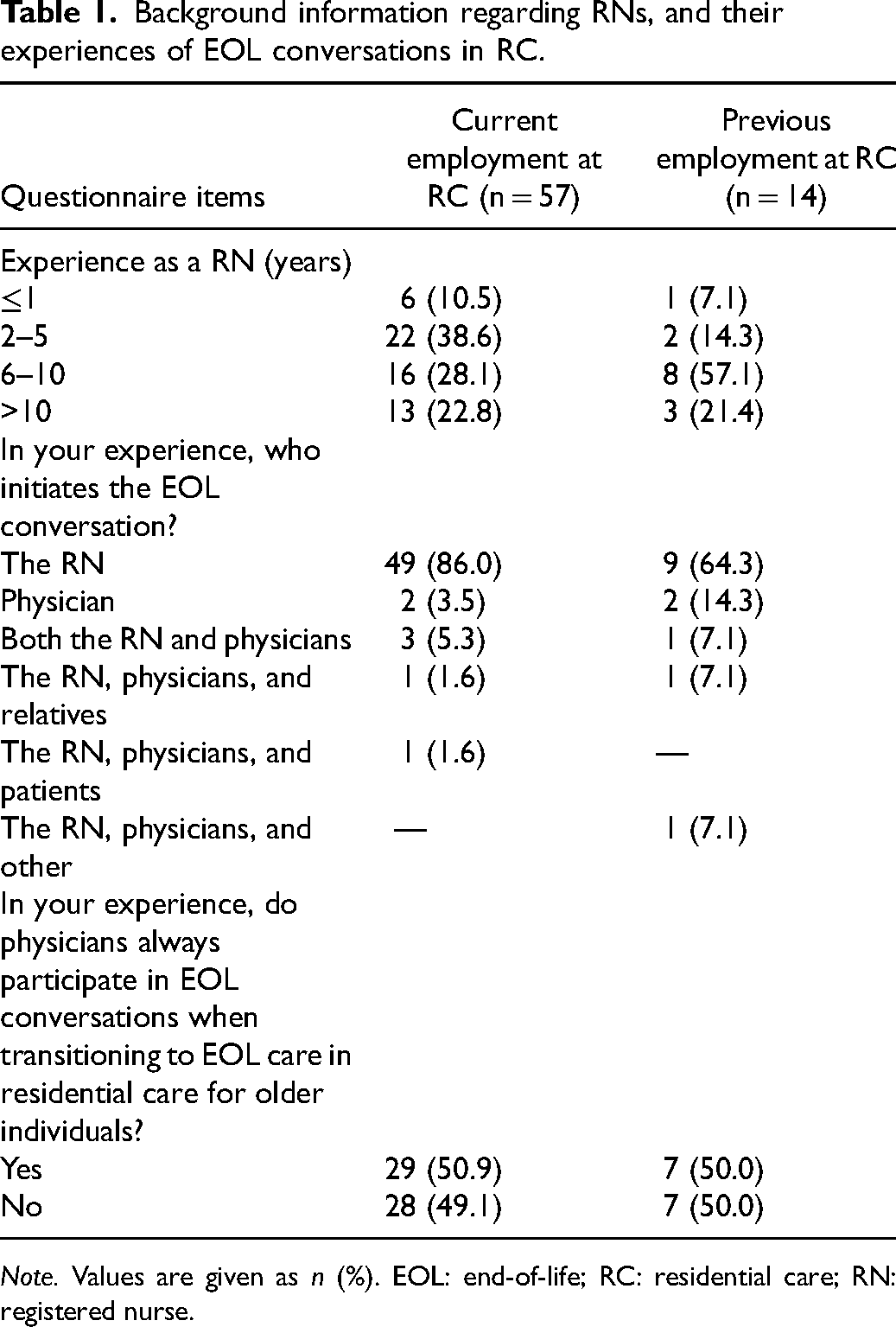
Note. Values are given as n (%). EOL: end-of-life; RC: residential care; RN: registered nurse.
Deficiencies in EOL conversations
The RNs’ reported shortcomings in the implementation of and in collaboration with physicians related to EOL conversations when transitioning to EOL care in RC. They also reported that those conversations took place too late, after the patient had already significantly deteriorated.
EOL conversations at too late a stage
The RNs stated that EOL conversations often took place too late, and that they should have taken place at a much earlier stage in the care process: “EOL conversations would often be needed earlier, ideally the topic would be raised at the time of admission and then could be brought up when needed” (P37); and “I think care and treatment should be discussed initially at moving in with the patient and document their wishes about how they want life to continue” (P4). The RNs reported that one reason EOL conversations were not held or occurred too late was that many patients in RC had cognitive impairment or a diagnosis of dementia. Instead, there was an unspoken transition to palliative care and the late EOL conversation took place with the family when death was imminent.
The RNs reported that often the patient's general condition was so poor once the EOL conversation was carried out that they were unable to assimilate information or express their wishes, which the RNs considered to be a shortcoming. “Many of our patients are in such a bad condition at the EOL that they cannot directly participate very much at all” (P18). The EOL conversations where the patient was present were described as positive in cases where the patient was able to understand and convey information. Otherwise, the RNs stated that patient participation in EOL conversations created unnecessary anxiety and confusion for the patient.
If the conversation was carried out too late or not at all, it was expressed as difficult for the RN in charge to know what level of care was appropriate as there was no explicit care plan. The RNs also pointed out that EOL conversations could take place several times at various stages of care and did not need to be limited to a single occasion.
Physicians’ absence in the collaboration concerning EOL conversations
The RNs reported that physicians did not always attend EOL conversations. “In my years, I have been involved in 2–3 EOL conversations where the physician was the one who lead the conversation. The rest we as RNs have had to take. So really, I guess you could say that most people have not had a real EOL conversation” (P64). The RNs stated that physicians were not confident in their role related to EOL discussions and often shied away from holding these conversations and making decisions related to it: “…have experienced some physicians as afraid to make decisions about EOL” (P34). The RNs described those physicians as acting too late and usually not until the RN had made several prompts about needing EOL conversations.
The RNs also reported that physicians have too little knowledge about palliative care, including EOL care, for patients in RC: “…In many cases I have witnessed that physicians avoid the EOL conversation, which only prolongs the suffering of patients or leads to the family not understanding what had happened if the patient dies” (P54). The RNs stated that a well-executed EOL conversation was preceded by the physician reading the patients’ medical records. This was not always carried out due to lack of time and that the physician trusted that the RNs would contribute with information during the conversation. The RNs reported that physicians often could not adapt their communication to the patient or relatives’ level and expressed themselves in a clumsy or unclear manner.
RNs also stated that the time physicians working at healthcare centers planned for RC was not enough to carry out EOL conversations to the extent that was needed. “…our physician only works 50% and therefore does not have the time to participate in such things. Never heard of physicians participating” (P46). Sometimes patients died before a proper EOL conversation had been held. The RNs reported that if EOL conversations and decisions about care did not exist, there was a risk that the patient's suffering was prolonged or that the patient was unnecessarily sent to inpatient care and died there instead of in the safety of their home. Families were sometimes not aware of the situation and did not understand what happened if the patient suddenly died. However, some RNs stated having a good collaboration with physicians who had a good knowledge of EOL care and understood the importance of raising questions about EOL care early on with RC patients.
Nurse's role in EOL conversations
The RNs reported that they took on a great deal of responsibility related to the implementation of EOL conversations in RC. They were usually the ones who initiated the conversation, acting as the link between participants, and often kept the conversation going as physicians did not always participate.
Initiate EOL conversations
The RNs stated that it was primarily RNs who initiated EOL conversations when it was relevant to transition to EOL care for a patient: “The physician in charge makes the decision, but often the RN in charge initiates it so that the EOL conversation is carried out with the patient and in consultation with the family” (P12). The RNs described that when a patient has deteriorated, the RN in charge must report this to the physician as soon as possible and initiate a care plan that includes EOL conversations: “The RN's role is to initiate, to tell the physician that it is time for him to make a decision about care at the end of life” (P33). However, the RNs expressed that it requires a high level of competence, experience, and good patient knowledge to take the initiative for EOL conversations.
Cohesive link between stakeholders concerning EOL conversations
It emerged in the analysis that the RNs experienced being a link between participants before, during, and after an EOL conversation. As RNs, they often needed to act as an interpreter and convey what the physician said in a more comprehensible way to the patient and the family: “Often the RN acts as an interpreter during the conversations and explains in a more concrete way what the physician says” (P21). In addition to acting as an interpreter, the RNs described that they were the ones who gave concrete examples of the measures that could be relevant. For example, which medicines were used for which purposes and when and how they were administered. The RNs also gave information about appropriate care and what and how measures could be carried out at the RC. [The RN’s role is] to be the link between family and patient and between them and the physician. To give advice based on my profession and to give support to the patient/the family in the discussion and decision and to give support to the physician as the one [the RN] who cares for the patient daily. (P38) [The RN’s role is] to help support the patient to dare to ask questions and support and help to make the patient's case according to previous wishes if the patient cannot express his will himself. Also, to be available afterwards to answer questions or support if needed. (P78) Listen to patients’ wishes at the palliative stage when the person can no longer express himself. Which family members we should contact, giving safety and calmness, listening to what the physician says and how the patient takes in. After the conversation, questions often arise in individual conversation with the patient and sometimes the family. (P51)
Carry out EOL conversations
The RNs reported that they carried out several EOL conversations on their own without a physician present, even though it was the physician's responsibility: “Unfortunately, physicians do not always have time to attend, so the conversation is handled by the RN responsible for the patient” (P49). In these cases, the conversation was conducted in the same way as if a physician had been present. Decisions and information were then passed on to physicians who executed medical decisions and prescriptions. The RNs stated that it was often perceived as more positive and rewarding to conduct the EOL conversation without a physician; however, the patient and the family were always offered contact with a physician in connection with the conversation. The RNs reported that the patient and the family in most cases declined contact with the physician as they did not see it as necessary after having the conversation with the RN: “In some cases, a physician's appointment was offered, but the patient or the family had no interest in seeing a physician. Sometimes they have no relationship with the physician and felt that the conversation the RN could offer had been enough” (P30).
The RNs stated that even though physicians participated in the conversation, it was often still the RN who led the conversation as they had knowledge of the patient's situation and which aspects were important to discuss. In cases where the physician was aware of the patient's situation and had good communication skills, the RN took a less hands-on role, confirmed the physician's information, and was more of an active listener.
Families’ involvement in end of life
The RNs stated that the family's involvement at the end of life was important and could be beneficial for all parties. However, family participation in EOL conversations could also lead to obstacles if the family had unrealistic expectations or a lack of knowledge.
Family participation in EOL conversation
The RNs reported that it was important to keep the family well-informed about the patient's state of health, and they considered the family's participation in EOL conversations to be positive. Continuous information about the patient's state of health both before and after an EOL conversation was described as beneficial so that the care could be planned and executed as effectively as possible for both the patient and the family. The RNs felt that the family usually understood the patient's situation and were prepared for the possibility that a deterioration could occur, leading to death.
The RNs stated that most of the family members who were asked to participate in EOL conversations wanted to be there, and those who did not have the opportunity to participate physically participated online or via telephone. The family members who did not have the opportunity to participate usually wished to be informed later by a RN or physician.
Further, the RNs described that these conversations resulted in a consensus and good knowledge about how the care would continue to be conducted. The family was able to contribute with information about the patient's previously expressed wishes and often had their own ideas about how the care should be conducted. The RNs reported that the family's participation in the patient's care at the end of life could help the grieving process after the patient died. The RNs stated that the memory of the last period with the patient was something that the family carried with them. Therefore, to have a good experience of this was obviously important: “My experience says that those conversations are usually the better ones. The family have been able to hear thoughts and wishes from their older family member. This is also usually good in the grief work afterward” (P9).
Unrealistic expectations at EOL conversation
The RNs stated that the family often had unrealistic expectations of care. If they did not have a realistic picture of the patient's state of health, it made it difficult to talk about EOL and could lead to the family experiencing dissatisfaction and mistrust of the care that was given. The RNs reported that there was a general reluctance among some family members to admit that death was imminent. In some cases, this was in combination with an ignorance of what death looks like.
The RNs stated that when a family member did not see the patient as often as the healthcare staff, they had not noticed the gradual deterioration in the patient’s state of health and were surprised and shocked when the EOL conversation was initiated. The lack of insight into the patient's state of health sometimes led to family members wanting investigations and treatments to be carried out at all costs so that the patient would get better again, even for the patient to be sent to inpatient care. There was a desire for a supply of nutrition intravenously when the patient stopped eating and drinking, and the RNs reported that RNs and physicians needed to explain what effects various treatments and measures would have and why they were beneficial to the patient, during an EOL conversation: “Some understand and accept. Some want to save lives at all costs, and there you have a challenge to explain why you do not hang onto a fluid bag (risk of pulmonary edema) or give other treatment” (P61).
Discussion
There is always an ethical dimension in RNs’ work with dying patients and in conversations about dying. However, the aim of this study was to describe RNs’ experiences of EOL conversations when transitioning to EOL care in RC. The RNs stated that EOL conversations were often conducted too late, by which time the patient was in a serious general condition, making it difficult to assimilate information or express their own wishes. Previous research shows that this patient group is affected when their decision-making capacity and ability to process information about their illness and care are affected. 5 Cognitive impairment and/or a diagnosis of dementia can also be a significant factor in late or missing EOL conversations. 22 The RNs stated that EOL conversations should be a practice during enrolment, which has also been shown in previous research.14,15
Further, the RNs described that they were the ones who primarily initiated EOL conversations when transitioning to EOL care. This is consistent with previous research that shows it is common for RNs to raise the issue more actively than before. 34 Furthermore, in accordance with previous research within cancer care, 23 the RNs reported that starting and conducting an EOL conversation independently requires not only a good knowledge of the patient and a well-established relationship with the family but also a high level of competence. In addition, this situation can create both confusion and insecurity among RNs due to prevailing regulations in Sweden, which stipulate that the physician who is responsible for the patient's care should conduct the EOL conversation 10 ; however, the RN in charge should be present to ensure continuity. 35 In addition, in practice, it is often RNs who hold the EOL conversations. It is conceivable that this task could be delegated to experienced specialist RNs on duty who both know the patient and can carry out the conversation at short notice. One can also reflect on the fact that the RNs in the present study shouldered much responsibility when implementing EOL conversations, and that half of those who reported that they initiated the conversations had only worked as RNs for 5 years or less.
The RNs in the present study also reported that physicians do not always physically participate in EOL conversations and that contact with a physician takes place later via telephone, which is consistent with previous research concerning acutely ill individuals in RC. 15 This leads to a lack of both a clinical assessment by the physician and a relationship between the physician, the patient, and the family. Further, in accordance with a study by Kuusisto et al., 36 the RNs stated that physicians are perceived as insecure in their role both when it comes to initiating the EOL conversation and in the practical implementation. Another aspect of the result is that RNs reported not getting a response from physicians when they highlighted a deterioration in the patient's condition and the need of an EOL conversation. One can reflect on whether physicians prioritize other issues than EOL conversations with the older individuals living in RC and their families, and if physicians rely on the RN’’ sense of responsibility and competence in this regard. However, lack of a common language between different professions has previously been shown to cause uncertainty and gaps in a context involving death and dying compliance, 25 and this might occur in the current context.
The RNs also reported usually having a good relationship with the family, which was beneficial when EOL conversations involving the family were initiated. This is consistent with Meleis’ 37 transition theory, where participation of the family is an important part of being able to prepare for end of life and is referred to as situational transition. RNs in the current study also described that when the family had not been present or well informed during the illness, distrust of care and treatment was created, and there were unrealistic expectations of continued care. This is confirmed by Goddard et al., 13 who showed that the demands of family members and their wishes for EOL care can be a challenge for RNs.
The results also show that RNs reported continuous information as important. This is in accordance with Meleis’ 37 transition theory, which states that the outcome of the transition is affected by the person's and their family's ability to understand the transition as well as what wishes, expectations. and previous knowledge exist. Further, healthcare staff are responsible for facilitating and supporting both the patient's and the family's ability to master the changes that come in connection with the transition. One suggestion is to standardize conversations by including the patient’s and family’s wishes, needs, and expectations upon admission to RC, Highlighting their previous wishes, knowledge and experience creates a solid foundation for participation in EOL care.
Methodological strengths and limitations
This study is exploratory in the sense that EOL conversations have mainly been studied in contexts other than RC. The advantage of using a web-based survey was that RNs had time to reflect over their answers. This was also considered positive from an infection prevention aspect due to the ongoing COVID-19 pandemic. A pilot survey increased the study's quality and credibility. The validity of the study was acceptable as the questionnaire items focused on the RNs’ own experiences. The reliability was also acceptable as the responses were anonymized and could not be linked to an individual. The survey gave rich data, even if the data did not have the same depth as the interviews. From a research ethics perspective, the data collection procedure had benefits, such as sending out invitations via Facebook. The potential disadvantages included the anonymity of participants, which meant that those who did not join the study could not identified or included. However, a web-based survey distributed and answered over the Internet allowed for a broader sample of participants, providing a variation years of experience among the RNs, thus strengthening the credibility and the generalizability of the results. In this way, the limited number of participants may also represent the total number of RNs in the Facebook group, although conclusions need to be drawn with caution. A possible limitation is that we did not collect additional background information, such as level of education. However, the choice not to collect any personal data to protect the participants’ integrity led to a strengthening of the confidentiality requirement. Inductive content analysis was considered an appropriate method for this study, given that the phenomenon has been investigated to a lesser extent in this context, and the study thus had a more exploitative approach.
Conclusion
An examination of RNs’ experiences in these situations can provide insights for organizational improvements as well as expand the personal knowledge base. RNs experienced a good relationship with the family, which was beneficial when EOL conversations were initiated. Using these relations has the potential to further develop quality in this phase of care. RNs employed in RC reported that they shoulder a great responsibility regarding EOL conversations by often both initiating and conducting the conversations without physicians, which also seems to be expected by other stakeholders. This occurred even though some RNs had limited professional experience. This knowledge, based on the RNs' perspective, could enhance the completeness and professionalism of EOL conversations. According to RNs, such standardized conversations need to be initiated at an early stage to enable patients to receive information or express their own wishes, and to have time to create good relationships with the family so they feel informed and involved. Building on the transition theory in palliative care might increase the possibility of providing the best possible care to both patients and families in EOL care.
Footnotes
Author contributions
ME, JF, MS and L-KG contributed to the study design. ME, JF and MS carried out the data analyses. ME and JF drafted the first version of the manuscript. ME, JF, MS and L-KG participated in interpretation of results, critically revised the manuscript for important intellectual content, contributed to successive drafts, and agreed on the final version. ME, JF, MS and L-KG read and approved the final manuscript.
Data availability statement
The datasets generated and/or analyzed during the current study are not publicly available due to Swedish regulations and laws but are available from the corresponding author on reasonable request.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public commercial, or not-for-profit sectors.
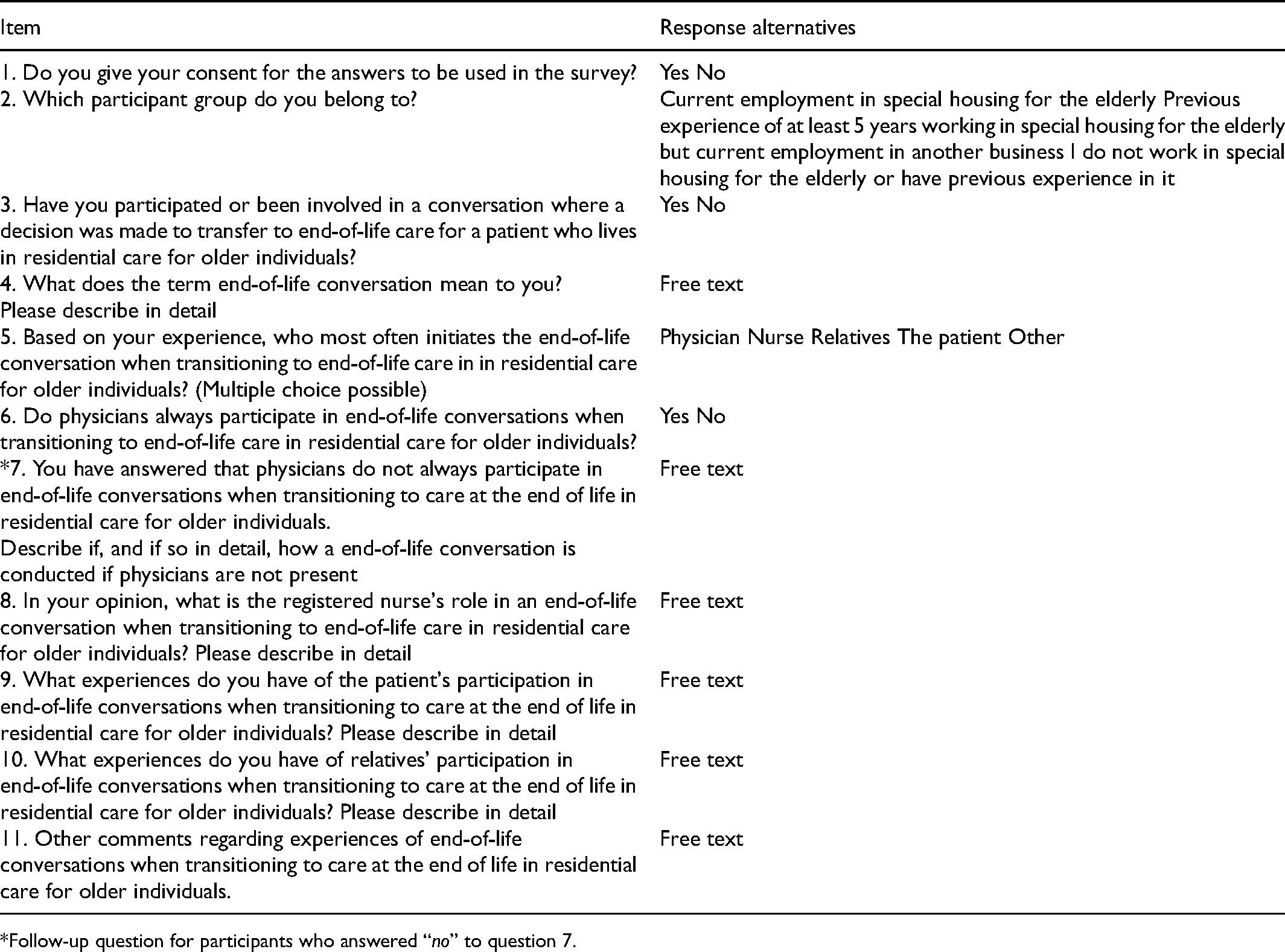
Appendix 1. Questionnaire items and response alternatives used in the survey
| Item | Response alternatives |
|---|---|
| 1. Do you give your consent for the answers to be used in the survey? | Yes No |
| 2. Which participant group do you belong to? | Current employment in special housing for the elderly Previous experience of at least 5 years working in special housing for the elderly but current employment in another business I do not work in special housing for the elderly or have previous experience in it |
| 3. Have you participated or been involved in a conversation where a decision was made to transfer to end-of-life care for a patient who lives in residential care for older individuals? | Yes No |
| 4. What does the term end-of-life conversation mean to you? Please describe in detail |
Free text |
| 5. Based on your experience, who most often initiates the end-of-life conversation when transitioning to end-of-life care in in residential care for older individuals? (Multiple choice possible) | Physician Nurse Relatives The patient Other |
| 6. Do physicians always participate in end-of-life conversations when transitioning to end-of-life care in residential care for older individuals? | Yes No |
| *7. You have answered that physicians do not always participate in end-of-life conversations when transitioning to care at the end of life in residential care for older individuals. Describe if, and if so in detail, how a end-of-life conversation is conducted if physicians are not present |
Free text |
| 8. In your opinion, what is the registered nurse's role in an end-of-life conversation when transitioning to end-of-life care in residential care for older individuals? Please describe in detail | Free text |
| 9. What experiences do you have of the patient's participation in end-of-life conversations when transitioning to care at the end of life in residential care for older individuals? Please describe in detail | Free text |
| 10. What experiences do you have of relatives’ participation in end-of-life conversations when transitioning to care at the end of life in residential care for older individuals? Please describe in detail | Free text |
| 11. Other comments regarding experiences of end-of-life conversations when transitioning to care at the end of life in residential care for older individuals. | Free text |
*Follow-up question for participants who answered “no” to question 7.