
Abstract
The World Health Organization and UNICEF recommend exclusive breastfeeding of all infants for the first 6 months of life, but a majority of mothers do not succeed in complying with that despite an expressed maternal wish to do so. A lot of mothers undergo an unwanted early cessation of breastfeeding within the first 6 months postpartum, and primiparous mothers are at particularly high risk of early cessation. Thus, the aim of the study was to explore how primiparous women experienced an unwanted early cessation of breastfeeding. The study had a phenomenological-hermeneutical approach. Data collection involved semi-structured interviews with five primiparous women in Denmark, analysed using Kirsti Malterud's approach to systematic text condensation. The study was performed in line with the COREQ Checklist. Three main codes emerged from our analysis: (1) Not meeting expectations; what do others think of me? (2) Breastfeeding; an emotionally hard fight leading to feeling defeated; and (3) Healthcare system under pressure and being left alone with inadequate support. The women were left with feelings such as a sense of defeat, inadequacy, grief and a weakened understanding of themselves as mothers. Our findings provide important insights into how mothers experience early cessations; however, further research is needed.
Keywords
Introduction
Strong evidence exists that breastfeeding is best for infants’ health, development and nutrition; furthermore, evidence indicates that breastfeeding has considerable positive lifelong effects on both the infant's and the mother's health.1,2 Therefore, the World Health Organization (WHO) and UNICEF recommend exclusive breastfeeding with no other food or liquid for the first 6 months of life.3,4 The literature shows that most mothers intend to breastfeed according to the recommendations; however, the overall worldwide rate of exclusive breastfeeding of infants under 6 months of age is only 40%. 3
As registered nurses (RNs) in the Nordic Countries, supporting the breastfeeding establishment and maintenance is part of our responsibilities, thus any issue with regard to breastfeeding should be our concern; however, the literature suggests that RNs sometimes struggle to provide breastfeeding counselling.5,6 Therefore, this issue is a matter that concerns the mothers as well as the nurses.
Early breastfeeding problems, such as severe pain or lack of sufficient support for the establishment and maintenance of breastfeeding, influence mothers to stop breastfeeding.7–10 When searching in large literature databases, such as CINAHL, PubMed, Embase and PsycInfo, it is clear that early breastfeeding problems leading to early cessation of breastfeeding are well-described in the literature, whereas the mothers’ own experiences of the early, and often unwanted, cessation of breastfeeding have received only scant attention. Some studies have shown that women who experience unwanted early cessation of breastfeeding are more likely to experience symptoms related to postnatal depression compared to those who succeed in breastfeeding according to the recommendations.11,12 Furthermore, studies show that women who, during pregnancy, intended to breastfeed according to the recommendations but did not succeed in doing so were much more likely to experience guilt and shame with regard to motherhood than were women who succeeded in breastfeeding according to the recommendations. 13 Although women's own experiences of unwanted early cessation are not well described, the available literature suggests that the phenomenon is both complex and important.
Today, the general presumption is that motherhood is characterised as being anything but easy as there are so many expectations to live up to in relation to being a ‘good’ mother. The high standards of what defines a good mother may seem impossible to meet, according to the common view, and how a mother nourishes her infant seems to be relevant in terms of whether one is deemed a good enough mother and therefore lives up to the aforementioned expectations. Overall, motherhood today is characterised by the pursuit of the natural in terms of having a natural pregnancy, a natural birth and a natural way of feeding the infant, i.e. breastfeeding instead of using formula.14–16
This implicit pressure, combined with health authorities’ breastfeeding recommendations, may very well lead to difficult feelings if breastfeeding is unsuccessful. It is easily imaginable, when being primiparous, motherhood is unfamiliar, and one's self-image as a mother is yet to be created. Therefore, it is reasonable to believe that unmet expectations regarding motherhood among this group of primiparous women, such as unwanted early cessation of breastfeeding, may be particularly difficult for them. Thus, we believe that seeking knowledge on how mothers experience unsuccessful breastfeeding establishment and/or continuation is relevant to understand and help these women and their infants.
Aim
The aim of the present study was to explore the experiences of primiparous women who had gone through unintended early cessation of breastfeeding.
Methods
Design
The design was qualitative and employed a phenomenological-hermeneutic approach inspired by Kirsti Malterud, who in turn drew on Amedeo Giorgi. 17 The study used Malterud's systematic text condensation, which involves an interaction between being openly curious and interpretive in order to identify meaning units leading to codes. This phenomenological-hermeneutic approach is characterised by this dual interaction of both bridling and using the researchers' preconceptions during the research process. 17 We have sought to minimise the potential bias that our preconceptions otherwise could have caused by being openly curious and deliberately attempting to bridle our preconceptions in the first phases of the research process, particularly during the interviews and when reading our data the first couple of times before the actual analysis.
Using Malterud's theory of interpretation, the study endeavoured to explain and understand the meaning of the primiparous women's lived experiences regarding unsuccessful breastfeeding as told by the participants themselves.
The study was performed in line with the Consolidated Criteria for Reporting Qualitative Research (COREQ) Checklist by Tong et al. 18
Data collection
The data were collected between February and March 2022 and consisted of individual interviews with five primiparous women. Neither of the two authors knew the five women and no relationships were established before the study commencement. All five women were informed about the aim of study (to explore how primiparous women experienced an unwanted early cessation of breastfeeding). The interviews, inspired by Steinar Kvale and Svend Brinkmann, 19 were conducted by the first author and involved a semi-structured interview guide with topics such as ‘breastfeeding experience; their history and their own perspectives of why it did not work out’ and ‘early cessation and its potential implications for their motherhood and womanhood’. The authors had no personal reasons or interests in the research topic, other than a scientific interest. All interviews used in-depth, open-ended questions to capture the nuances of the mothers’ lived experiences of unwanted early cessation of breastfeeding. For example, they were asked how they experienced the time leading up to breastfeeding cessation and how they experienced the time during and after cessation. Four interviews were conducted using a secure video meeting platform (visual recording); due to technical problems, one interview was conducted via telephone (audio recording), and no one else besides the mothers (and their babies) and the first author was present during the interviews. The interviews lasted between 45 and 58 min, and they were recorded and transcribed verbatim by the first author.
Sampling and participants
To ensure data variation, purposeful sampling was used when recruiting the participants for the study. The overall criterion for including participants was that the mothers were primiparous. Furthermore, we sought variety in their duration of breastfeeding. Participants were approached online; as authors, we wrote a post online on SoMe for two different groups of Danish mothers, explaining the study's aim and inclusion criteria, and encouraging mothers who fitted the criteria and were interested in participating in the study to contact us. Five women (age range 28–42 years) who fitted the inclusion criteria were selected and we obtained their consent to participate in the interview and none of the women dropped out during or after. All women had a higher education (2–5 years) and were living in a relationship with the father of the child. The five women lived in five different cities and regions in Denmark. Four of the women were ethnic Danes and one was ethnic Dutch but was living permanently in Denmark. Two of the women had been pregnant and given birth again, but the interview was about their experiences with their firstborn child.
Ethical considerations
This study followed the guidelines of the Declaration of Helsinki and associated principles for ethical research. 20
All participants were informed verbally and in writing about the aim of the study, confidentiality, anonymisation of identity, voluntary participation and the right to withdraw from the study at any time, and all signed a consent letter regarding the aforementioned and their voluntary participation.
According to Danish Law, qualitative studies, such as ours, do not need ethics approval; thus, we did not apply for any ethical approval before the study.
Data analysis
The first author analysed the data, and both researchers discussed and reflected on them using Malterud's procedure of interpretation, systematic text condensation, from which themes derived. Table 1 provides an example of the steps in the data analysis.
Example of steps in data analysis.
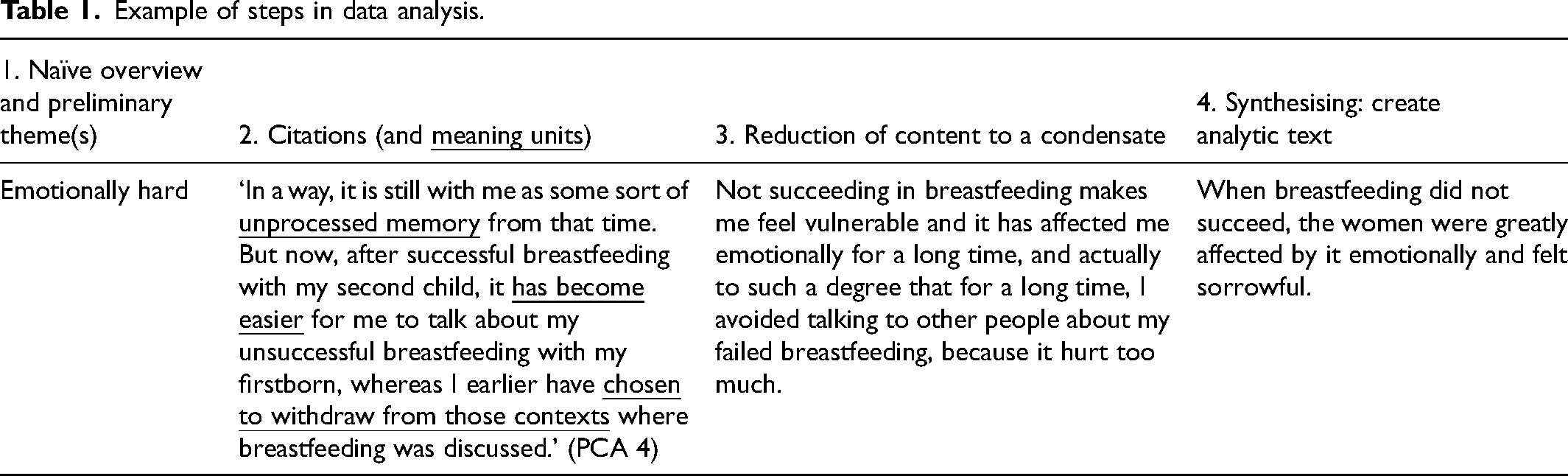
This approach has four steps: total impression; identifying and sorting meaning units; condensation; and synthesising. 18 The first step, total impression, involves trying to create a naïve overview of the data while aiming at bracketing out our preconceptions and identifying preliminary themes from the material. The second step, identifying and sorting meaning units, involves identifying and organising elements that may elucidate the study question by systematically reviewing the transcript line by line (meaning units, which means a text fragment containing some information about the research question), and while doing this, establishing code groups. The third step, condensation, involves sorting the meaning units of the actual code group into a few subgroups and reducing the content into a condensate by creating an artificial quotation. With the fourth and final step, synthesising, descriptions on the basis of the previous steps are developed, creating an analytical text for each code group to gain a deeper understanding of how the women interpreted the experience of unwanted early cessation when being primiparous. Throughout the ‘Findings’ section, participant quotations are presented to illustrate the findings and each quotation is identified by participant number.
Findings
Using systematic text condensation, we identified three main codes:
Not meeting expectations; what do others think of me? Breastfeeding; an emotionally hard fight leading to feeling defeated Healthcare system under pressure and being left alone with inadequate support
We elaborate on all three codes below. Selected quotations are included that unfold and validate the interpretations.
Not meeting expectations; what do others think of me?
Although the women had personal intentions and hopes regarding breastfeeding their infant, they expressed feeling external pressure from the healthcare system and people in general about how they fed their infant. When meeting other people, concerns were raised about whether one was seen to be doing the right thing as a mother. One of the mothers described it as follows: ‘Though most people probably won’t admit it, there are judgements about feeding your infant using formula milk instead of breastfeeding because…it is not the right thing to do’ (PCA 4).
According to the women who participated in the study, this perspective was also evident in the healthcare system. Thus, in addition to feeling that breastfeeding was better than formula and being aware that other people might be thinking that too, the women were also very aware of the health authorities’ scientific recommendations regarding exclusive breastfeeding for 6 months, and therefore felt that breastfeeding undeniably was the best. Although the women expressed the desire to breastfeed, they experienced the healthcare system as insistent regarding the importance of establishing and continuing breastfeeding. One of the mothers expressed it this way: ‘The healthcare system is so intent on breastfeeding that thinking about it makes me completely sick. At least, they should present people with an alternative, so people know there are other ways of feeding infants’ (PCA 5). Being aware of the recommendations while not being able to live up to them or expectations of how to ‘properly’ nourish an infant was experienced as difficult by the women, as they genuinely wished to be a good mother for their child, in their own opinion and with respect to society's opinion. One mother stated: ‘It was as if breastfeeding was the only possibility. No one ever presented me with an alternative until the situation had become problematic’ (PCA 5). In addition, the women had fought so hard trying to establish breastfeeding, and they knew that strangers with no knowledge of their situation would not be aware of that. So, when giving up breastfeeding and meeting the world with a bottle, the women feared what others might think of them as mothers: ‘I was concerned that other people might think … that I had taken the easy way out. I know it is a crazy thought, but it is a strong feeling of not being a “real” mother’ (PCA 1).
During pregnancy, the women did not expect breastfeeding to be a problem and assumed their bodies intuitively would know what to do when the baby was born and should latch on, because no one had informed them about the potential struggle breastfeeding could be. Therefore, they expected to breastfeed and had expected to breastfeed exclusively in accordance with the recommendations (the first 6 months postpartum). When the women discovered that their breastfeeding establishment was problematic and may not succeed, they felt ashamed of their bodies and themselves as women and mothers. Thus, they immediately blamed themselves and simultaneously feared what others might think of them as mothers. This internal pressure to breastfeed was reinforced by the direct external pressure they felt when meeting the healthcare system that was insistent regarding the importance of establishing and continuing breastfeeding.
Therefore, the women expressed feelings of guilt and shame about ceasing breastfeeding earlier than planned and recommended as they believed that a good mother would and could breastfeed her child because that is what the health authorities say is best. Thus, some might believe you do not want what is best for your child. The women knew that this was unlikely, but still had some fear about this, which led to shame and self-blame. The women experienced that it was challenging meeting the world with a bottle as they felt ashamed and guilty about not establishing and/or continuing with breastfeeding, experiencing an inconsistency between how they wished to act and how they actually acted. Thus, they had to align their prepartum preconceived image of themselves as mothers with the postpartum actual image of themselves as mothers and society's view of the good mother complicated this process and reinforced their feelings of shame.
Breastfeeding: an emotionally hard fight leading to feeling defeated
As mentioned in the previous code, the women were emotionally affected by not succeeding in breastfeeding and were affected for quite some time after. Feelings such as sadness, self-recrimination and even grief dominated the time during and after the unwanted early cessation of breastfeeding. One of the women described it as follows: ‘The following days, weeks and even months, I felt grief-stricken that the breastfeeding did not work out as I had hoped. And I can still feel this grief, I can actually feel the grief right now as we speak, as I am sitting here with tears in my eyes simply talking about the matter. Also, I felt sad that my body could not do it properly … and, of course, I blamed myself.’ (PCA 4)
This underlines the complexity of breastfeeding cessation; it is more than just a biological matter, affecting the women psychologically and emotionally.
Furthermore, the women had a particular way of talking about breastfeeding cessation. They all described it as a hard fight that they had lost, almost to such an extent that it sounded like they were soldiers in war rather than mothers trying to nourish an infant. The women fought bravely to establish and maintain breastfeeding, and most of them experienced that making the decision to stop was complex as well as difficult, and as such kept trying. One of the mothers phrased it as follows: ‘I felt that I had to do everything possible to make this work’ (PCA 4); and another described it with these words: ‘I kept on getting more and more emotionally unwell, and yet I kept thinking that… I have to give it just one more chance and I simply have to keep on trying… again and again’ (PCA 1). Most of the women stopped fighting for breastfeeding only after they were physically and emotionally exhausted and when they could do no more.
The women also described how they needed help from relevant healthcare professionals to make the decision because of its complexity. In a way, they instinctively sought a kind of permission to end this ongoing fight. One of the mothers explains it as follows: ‘I guess the fact that a healthcare professional finally confirmed what I had been feeling all along – that it was really difficult, and that it simply would not work out, and something clearly was not working – gave me permission to consider giving up the fight.’ (PCA 1)
Despite having fought so hard, all of the women described how they were left feeling defeated. They felt that they had failed as mothers and blamed themselves and their bodies for failing at something they allegedly ought to succeed at as women: ‘Well, my thought was: you had one job, and you could not even succeed at that. And so you really blame yourself and your body for that’ (PCA 5). These feelings of failure and inadequacy, and of not meeting their personal breastfeeding intentions, left the women sorrowful to some degree. They expressed grief about the early unwanted cessation of breastfeeding that still affected them greatly though it had happened 6–24 months before the interviews. During the interviews, the women brought up the expression ‘breastfeeding grief’. The women explicitly expressed that they had experienced a genuine grief at not being able to breastfeed as they had hoped and planned, and while experiencing this breastfeeding grief, they felt that their situation and feelings were neglected by others, which made the situation even worse. One of the mothers explained it as follows: ‘Unsuccessful breastfeeding is often overlooked and ignored by others, because nobody has died and there is a common understanding that you can easily give your child a bottle with formula, and the problem is solved… But it does not change the fact that I as a mother feel grief about not being able to breastfeed my child as I had hoped and wished.’ (PCA 4)
Undergoing unwanted early cessation of breastfeeding and thereby allegedly suffering a personal ‘defeat’ that brought feelings of sadness, grief, self-recrimination and shame with it, while experiencing everyone else simply ignoring the importance of the experience, was challenging emotionally. Furthermore, it underlined a paradox, as although the women described how utterly crucial the establishment and continuation of breastfeeding was considered by the public and the healthcare system, when breastfeeding failed, no help, support, attention or compassionate understanding were given. The mothers were left alone, and this presumably intensified their difficult situation.
Healthcare system under pressure and being left alone with inadequate support
All of the interviewed women were primiparous; thus, after giving birth, they subsequently were offered hospital admission. However, they all found their hospital admission to be a tumultuous experience characterised by well-meaning yet chaotic and stressed health professionals who simply did not have the time to provide the necessary support or care, indicating that the healthcare system was perceived as being under massive pressure. Thus, when meeting the hectic healthcare system, the women did not feel seen, heard or understood, resulting in a feeling of being left alone with a task (breastfeeding) that was overwhelming and foreign to them.
Due to being primiparous, none of the women had any breastfeeding experience; however, several of them described that they had an intuitive sensation multiple times of something that was not right regarding their breastfeeding, e.g. the latch felt wrong. However, the women did not know whether it really should feel this way or how they could change it to the better. Moreover, when they contacted the health professionals at the hospital, their concerns were promptly rejected and they were reassured that everything looked just fine. One of the women expressed: ‘When my infant was put upon my breast and should latch for the first time after being born, I immediately felt an inner alarm clock ringing, telling me that something was not right at all, and therefore I called for help… When the nurse entered the room, the atmosphere was quite stressed and hectic, and I explained how I felt and she very quickly took a look at my infant's latch and immediately reassured me that everything looked fine, and then hurried out of the room again.’ (PCA 3)
These continuous, hasty conclusions, that ‘everything was just fine’, made the women doubt their bodies’ signals and they were thereby confused. Even though they had no experience with breastfeeding, they repeatedly felt that something was not right; the latch hurt and somehow just felt wrong. Thus, their bodies were really trying to tell them something, but the health professionals were so busy that they were not capable of helping the women translate what their bodies’ signals were trying to tell. On the contrary, they were so busy that the women were led to ignore their bodies ‘signals, which further must have challenged their attempt to establish breastfeeding.
In addition, the repeated attempts to seek help from the stressed healthcare professionals, who never had the time to properly listen, examine and assist but merely assured the women that everything looked fine before quickly rushing away, made the women feel like burdens who were in the way. Thus, many of the women chose to handle their issues on their own and stopped asking for help. The assistance provided was so insufficient and uncomfortable to request as the health professionals obviously were under much pressure. This left the women with a feeling of being very much alone.
During the interviews, several of the women wondered about the paradoxical situation they had been in; they were new mothers who wished to breastfeed and tried their best to establish breastfeeding as they had been told by society and the healthcare system that it was the best possible way to nourish their child. However, then when they engaged with the healthcare system to establish breastfeeding, they received inadequate support. It seemed the system lacked the necessary resources to provide proper care. One of the mothers phrased it like this: ‘To me, it seemed as if the healthcare system did not have either the time or the resources to prioritise breastfeeding support… Therefore, the system's attitude in regard to breastfeeding was like “Well if you can’t breastfeed, then why don’t you just give your infant a bottle instead?” Still, they constantly emphasised the importance and benefits of breastfeeding. However, I never experienced a health professional who really took the time to sit with me and say “Why don’t you try and latch the infant and then I will help you do this properly”’ (PCA 5)
After the premature and unwanted cessation of breastfeeding, the women experienced not only grief and self-blame but also a certain anger towards the healthcare system for abandoning them during such a critical time. Since the healthcare system had established the breastfeeding recommendations, the women felt that the system was partly to blame for the breastfeeding pressure they faced, both internally and externally. Although they kept blaming themselves for not succeeding with breastfeeding, they also acknowledged that the healthcare system was partly at fault. It had abandoned them completely during their attempt to establish and maintain breastfeeding and after they experienced the unwanted early cessation. Unfortunately, this realisation, which each woman came to on her own, did not eliminate their self-blame, shame and guilt for ceasing earlier than hoped and planned. However, it did somewhat alleviate these feelings.
Thus, the overall understanding is that the three codes are interconnected and thematically related. Both individually and collectively, these codes clarify that the phenomenon of unwanted early cessation of breastfeeding is highly complex and characterised by an emotionally challenging process.
As a phenomenon, breastfeeding may be viewed as a completely simple, natural and intuitive biological process. However, when breastfeeding is unsuccessful, there is nothing simple or intuitive about it. On the contrary, the experience of (unsuccessful) breastfeeding is emotional and psychologically complicated. The women included in this study genuinely wished to breastfeed and fought (far too) hard to succeed. During their attempts to establish and maintain breastfeeding, they gradually recognised the severity of their situation and how increasingly incapacitated they had become. However, they were continuously subjected to both internal and external breastfeeding pressures, which seemed to reinforce each other, further contributing to the challenging psychological process that characterised the unwanted early cessation of breastfeeding. Furthermore, the primiparous women clearly had some preconceived notions of breastfeeding and preconceived expectations of themselves as mothers. Therefore, their self-understanding and identity as mothers and women were deeply challenged when breastfeeding was unsuccessful. As a result, the decision to cease breastfeeding was very difficult for them.
Discussion
This study showed that primiparous women who intended to breastfeed according to the recommendations but did not succeed in doing so, and thereby experienced unwanted early cessation of breastfeeding within the first 6 months postpartum, were greatly affected by it emotionally. Unwanted cessation of breastfeeding is a complex phenomenon and cannot be simplified to a matter of biology only. Similar to other studies, this study has shown that breastfeeding problems leading to unwanted cessation are emotional matters as well. This is not a new phenomenon; a study undertaken in 2000 by Mozingo et al. described how mothers who had experienced unwanted early cessation of breastfeeding felt guilt, self-directed anger, shame and disappointment; and this finding has subsequently been supported by other more recent studies.21,22 This indicates that the intensity and nature of how women are affected by their breastfeeding experiences have remained relatively unchanged over time.
Our findings showed that the mothers were concerned about what others might think of them when feeding their infant with a bottle instead of breastfeeding. This concern was extended to foreigners, family, friends and health professionals. The women in our study expressed that they felt an external pressure to breastfeed, and health professionals were also directly contributing to this feeling as they repeatedly encouraged the women to breastfeed, both before and after the birth. The women were left with a clear impression that ‘breast is best’. The key problem when asserting that something is definitely ‘the best’ is that this indirectly implies that any alternative is inferior and possibly even harmful. A recent study from 2024 by Grattan et al. found that perceived pressure to breastfeed (from friends/family or health professionals) negatively impacts postpartum mental health outcomes over time. 23 This effect is particularly pronounced for those who place a high importance on breastfeeding as a critical aspect of being a successful mother. The study presented that many well-meaning breastfeeding interventions in our healthcare system backfire on the mother's mental health as they do not consider the maternal mental health at all but solely consider increasing breastfeeding rates. 23 However, it is reasonable to believe that health professionals sometimes can find themselves struggling with the balancing act of promoting breastfeeding. A recent study from 2024 by Hamnøy et al. describes health professionals’ experiences of this balancing act of being obliged to support and promote breastfeeding in a manner that accords with the national recommendations but does not pressure the mothers too much. 5
The concern of what others might think of them is also described in a study from 2013 by Larsen and Kronborg, 24 who found that not only did the women have concerns about this matter, but they also experienced others interfering when they fed their infant with a bottle, which the women in our study had not experienced. As for the women in our study, their level of concern was generally high, not only regarding others’ opinions but also regarding their own personal ambitions and internalised beliefs about motherhood. They expressed concerns about whether they lived up to the high modern standards of how to be a good mother – a ‘real mother’. They felt guilt and shame when they realised that they had to give up breastfeeding because a ‘real’ mother ought to breastfeed her child and be able to make her body do so. A clash thus existed between the women's hopes and desires for motherhood and the reality of motherhood because they had internalised breastfeeding as an essential aspect of their motherhood identity.
A similar finding was identified by Jackson et al. in 2021. They found that mothers who during pregnancy intended to breastfeed postpartum but did not succeed had remarkably higher levels of guilt and shame than those who succeeded in breastfeeding and thereby met their personal breastfeeding intentions. 13 This could suggest that the key to understanding why some women experience early cessation in breastfeeding to be so emotionally painful and sorrowful as described in this study could partly be attributed to their prenatal intentions regarding infant feeding. Identifying women's prenatal breastfeeding intentions may therefore be expedient as it may help identify those who could be in need of help and compassionate support if breastfeeding is unsuccessful.
A study from 2015 by Borra et al. investigated how unwanted cessation of breastfeeding negatively affected women in relation to postpartum depression, showing that women who had breastfeeding intentions during pregnancy that they were not able to meet postnatally had the highest risk of postnatal depression (PPD). 25 This finding is supported by a study from 2011 by Watkins et al., and it emphasises the complexity and severity of the matter; it is not only a matter of how infants are fed and how mothers feel about the way their infant is fed but also a matter of maternal health, currently and prospectively, affecting the woman, her child and the family. 12
In view of this, and considering the high global rates of early cessation of breastfeeding that highlight how often mothers are unable to breastfeed, this situation is particularly concerning. The literature shows that women's breastfeeding self-efficacy is greatly affected by their breastfeeding experiences within the first week postpartum. This is worrying because breastfeeding self-efficacy is an important determinant of breastfeeding duration. If the experiences in the first week postpartum are negative, the odds for having low breastfeeding self-efficacy increase ninefold, and the likelihood of a drop in breastfeeding self-efficacy triples, particularly among primiparous women. 26 Thus, maternal health should be a matter of the highest priority due to its importance for the child's wellbeing and development, as well as the mother's future quality of life.
Methodological reflections
The study is weakened by its sample size of only five participants, but it is strengthened by its qualitative approach that used semi-structured interviews with in-depth narratives on the lived experience of being primiparous and undergoing unwanted early cessation of breastfeeding as rich data were obtained. Purposeful sampling for variety in the women's duration of breastfeeding supported variety in the data. The participants were quite homogenous in terms of sociodemographic variables, but our findings are supported by other studies and reviews of more diverse groups of mothers. The interviews were conducted using a secure video meeting platform (n = 4) or telephone (n = 1), and the participants were not known by the interviewer (first author). Despite the lack of face-to-face interaction, a safe and strong connection was established, allowing the interview to address delicate and personal matters. The study focused on primiparous mothers; yet, two of the included women had subsequent pregnancies and births. The interviews specifically addressed their experiences with their firstborn child. This may have affected their responses, and the potential recall bias for these two women may have been greater than for the other women who participated in our study. However, both of these women gave birth to their firstborn infants in 2020, while the other three women had their firstborn infants in 2019, 2020 and 2021. Therefore, their timelines for their firstborn infants are not significantly different.
The analytical process, inspired by Kirsti Malterud's phenomenological-hermeneutic approach, was undertaken by the first author and was supervised and validated by the second author. Following the steps of the analysis enabled analytical rigour while being true to the participants’ expressions and intentions. The structural analysis included interpretation-providing quotations, making the two main codes clear. Research reflexivity was applied by both researchers throughout the data collection and analysis process.
Conclusion
This study showed that primiparous mothers undergoing unwanted early cessation of breastfeeding experience it as emotionally challenging. The study concluded that the attempt to establish and maintain breastfeeding was often described as a regular fight. Undergoing cessation and losing this fight led to feelings of defeat and inadequacy as a mother. It also triggered irrational thoughts about whether they were good enough mothers while bottle-feeding their infants. Furthermore, grief, self-recrimination, shame and guilt about not succeeding with breastfeeding dominated the period during and after breastfeeding cessation. These feelings were compounded by a sense of abandonment by the healthcare system both during their attempts to establish breastfeeding and after the early cessation. Therefore, on the basis of our study, it is reasonable to conclude that it is essential that primiparous mothers who are unable to meet their breastfeeding intentions, must be offered special compassionate support and help from relevant healthcare professionals before, during and after cessation.
Relevance for clinical practice
This study produced new important knowledge about the lived experiences of mothers experiencing unwanted early cessation and how to help and support primiparous mothers undergoing unwanted breastfeeding cessation. Some of the findings are supported by other studies and some are not, suggesting that further research on this matter is needed, especially due to the study's limitations regarding the number of participants. Nevertheless, findings from the study provide relevant insights for clinical practice. This study imparts knowledge about the need for support from relevant healthcare professionals for mothers struggling to establish proper breastfeeding. These mothers may require support in making timely decisions about cessation. In addition, mothers who intended to breastfeed but were ultimately unable to do so needed compassionate support.
Footnotes
Author contributions
Both authors have substantially contributed to the conception or design of the work; or the acquisition, analysis or interpretation of data for the work. Both authors have drafted or revised the paper critically for important intellectual content. Both authors have given final approval of the version to be published. Both authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
The authors are sincerely thankful to the women who voluntarily participated in this study.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.