
Abstract
Home care supports clients in living at home. Among home care professionals, nurses are the largest group. The aim of this integrative review was to examine literature results of competencies that were required of nurses when working in home care. The review process followed the method by Whittemore and Knafl. A database search was conducted using CINAHL, PubMed and Cochrane. The PRISMA search strategy was used in the process. Nine selected articles were evaluated using the Joanna Briggs Institute criteria. The content analysis was used in analysing data. Eight competencies were defined: nursing practice at home; managing in changing situations; technological competence; communication and interpersonal skills; teamworking; continuous development; leadership and management skills; and personality factors in home care. The review suggested that nurses experienced a need for several competence requirements when working alone. Looking after patients with multiple health problems and having changing situations at work need continuous competence development. Situations to update and develop competence in daily work are needed. Further research is needed to confirm competence requirements for both registered and licensed practical nurses. The PRISMA checklist was used to guideline manuscript reporting.
Introduction
Providing health and social services at home is increasing in Europe 1 as a response to the growing number of older people in the population, 2 policy priorities such as deinstitutionalisation and community-based solutions, changes in attitudes and expectations for care, and technology. 3
Home care is an umbrella term covering care services that are provided at home 4 with an aim to support the functional activity and quality of life for the patient instead of hospital care.3,5 Home care policies and the practical organisation and the availability of services vary between countries, 1 and variations also occur within countries between municipalities. 6 Services are provided as private or public. Private services may be non-profit or for profit. 1
Care providers are both professional and non-professional. Nurses are the largest group of professionals in home care; other professionals include home care assistants, social workers and physicians. In addition, different therapists, home workers and volunteers work in home care. 3 Home nurses and general practitioners coordinate care. 7
Nursing practice in home care includes interactive, educational, caring and administrative activities, all of which need to be supported by various kinds of knowledge. 8 Nurses must be able to assess and attend to patients with complex needs, of different ages and in different home situations.9,10 Nurses work in multidisciplinary teams to make plans that meet patients’ needs and involve families in patients’ care. 11 The work includes caring for minority groups,10,12 depression care, 13 telephone counselling, 14 supporting in daily activities, maintaining documentation, 15 leadership of other nurses, practising evidence-based nursing and pedagogical competency.10,15
The concept of ‘competence’ is difficult to define and assess. 16 Woodruff defined competence as the aspect of a job that an individual can perform. The job consists of roles, deliverables and outputs that require several individual competencies. Competency is the behaviour that supports such performance. 17 McConnell described competence as an individual ‘s capacity to carry out job responsibilities. The assessment of competence evaluates potential knowledge and skills. Competency is an individual's performance in a certain situation. The assessment of competency evaluates a person’s ability to perform and use knowledge and integrate that knowledge and skills. 18 According to Cowan et al., 19 nursing practice needs multiple combinations of knowledge and skills, as well as performance, values and attitude. Fukada 20 described competence as abilities gained from experiences and learning. These enable us to work effectively in certain circumstances. Motivation is needed to use those abilities. Competency is a behavioural characteristic based on the interests and experiences of individuals and is influenced by their motivation and attitudes. Nursing competency requires the ability to combine knowledge and skills in particular situations. Gonczi 21 described competence as the capacity to integrate knowledge, values, attitudes and skills into practical situations. According to Moore et al., 22 there are differences in the use of terminology and the interpretation of terms. They suggested that competence is an area of work, competency is the behaviour that supports this area and competencies are the attributes that support a behaviour.
There are earlier reviews with definitions of competence requirements in home care. Bing-Johnson et al. 15 described competence requirements in Norway home care and nursing homes. That review integrates a literature review and Norwegian policy documents. Rusli et al. 23 described competence requirements in home-based nursing care between 1992 and 2020 in several countries and multiple types of studies.
In this review, home care is defined as the care of adult patients in the home, excluding nursing homes and outpatient clinics environments. This review is based on an integrative review including peer-reviewed articles only from home care and limited to 2011–2023, because home care services have since changed. 3
In this review, competence requirements included nurses’ own experiences because nurses work alone and understand their experience is important. Nurses felt that a lack of competence affected work satisfaction negatively. 24 In addition, patients’ care needs have become demanding 25 and nurses need adequate competence, work experience and training to provide high-quality services with patient safety. 26 Nurses in this review were defined as registered, public health, district, licensed practice or assistant nurses. Competence is defined according to Meretoja et al., 27 as the functional adequacy and capacity of nurses to integrate knowledge, skills and their attitudes and values in a home care context. The term ‘competencies’ is used in this study from the plural of competence because it is also used in original studies in this review.
The aim of this study was to examine the literature results and answer the question: What competencies do nurses require when working in home care?
Material and methods
Design
The process in this integrative review followed Whittemore and Knafl's five phases: problem identification; literature search; data evaluation; data analysis; and presentation. 28 The literature search process and reporting followed the PRISMA statement and PRISMA 2020 guidelines. 29 The studies with different methodologies were included this review.
Literature search and data evaluation
The literature search was carried out in CINAHL (EBSCO) on 15 May 2021, PubMed (Medline) on 10 August 2021 and Cochrane Library on 10 August 2021 and was limited to the years 2011–2021. Demographic changes and the increasing number of older people 2 brought about a need for organising and finding solutions to provide community care 30 and care in the home. 3 The search was updated on 11 March 2023, but no additional articles were selected.
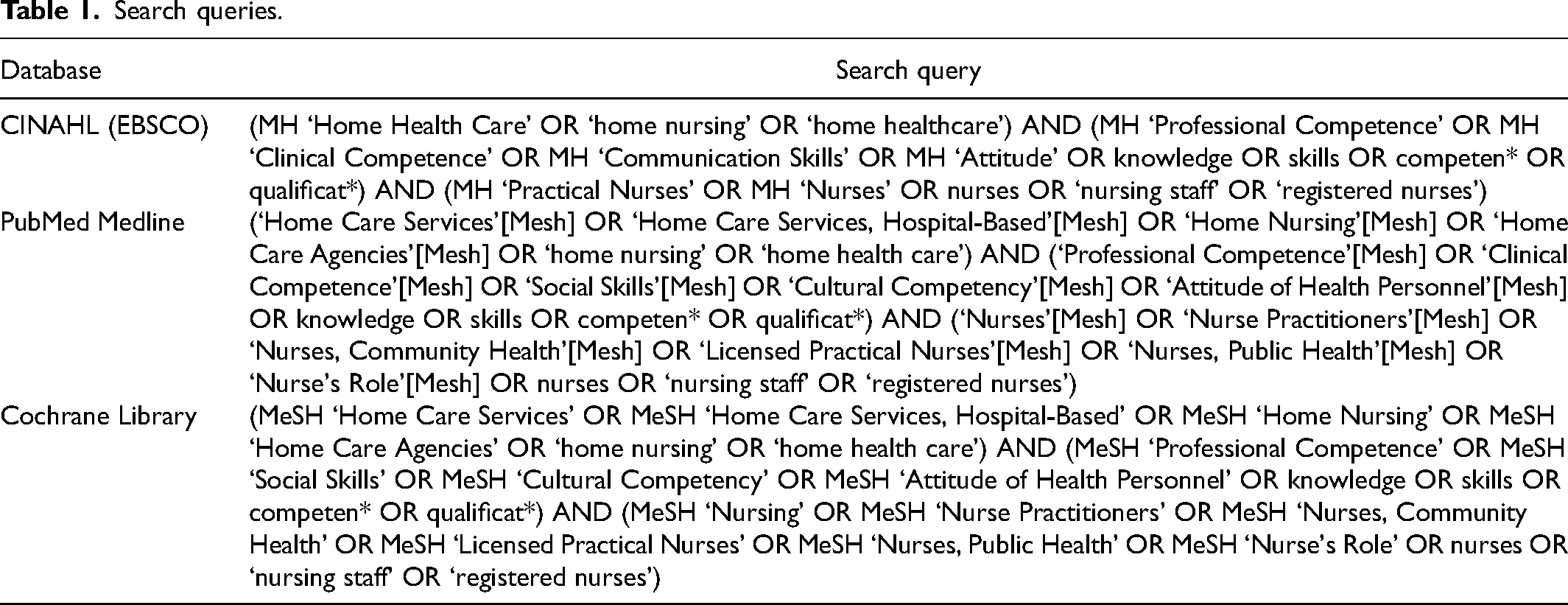
The first author planned the search strategy together with an information specialist. 28 The search terms were ‘competence’, ‘nurse’ and ‘home care’. Searches were conducted separately in every database, using the database's own Medical Subject Headings (MeSH) terms derived from keywords, as well as common search terms: ‘knowledge’ OR ‘skills’ OR ‘competen*’ OR ‘qualificat*’ AND ‘nurses’ OR ‘nursing staff’ OR ‘registered nurses’ AND ‘home nursing’ OR ‘home healthcare’ (Table 1).
Search queries.
The inclusion criteria were as follows: (1) articles describing nurses’ competencies working in home care; (2) articles published in scientific peer-reviewed journals; and (3) articles in English. The exclusion criteria were as follows: (1) articles describing the competencies of professionals other than registered nurses, public, district or licensed practice nurses or nursing assistants; (2) articles that included data from working environments other than home care; (3) articles combining data on the competencies of nurses and other professionals; (4) articles describing results measuring competencies; and (5) articles that were case reports or series, narrative reports or expert opinions.
The search resulted in a total of 1856 articles from the databases (Figure 1) as follows: 1070 in CINAHL; 561 in Medline; and 225 in Cochrane (45 reviews and 180 trials). Two records were identified manually searching for author names and citations. Duplicate records were removed (n = 155). All article titles and abstracts were considered against criteria by the first author. In all, 64 reports were either not retrievable, the full text was unavailable or the study was not in English. After reading the full texts of 703 studies, a total of 90 articles were included and were considered by both authors. The full texts of the selected studies were reviewed and considered using the criteria by the authors independently, the results were compared and a consensus was reached. The articles were grouped as included, to be discussed or excluded. The authors discussed their independent choices and by consensus, and more than 45 articles were excluded. Those articles did not clearly fit the inclusion criteria. During this discussion, case reports or series, narrative reports and expert opinions were also excluded (n = 36). No articles that were manually searched were selected. Finally, nine studies included in this review.
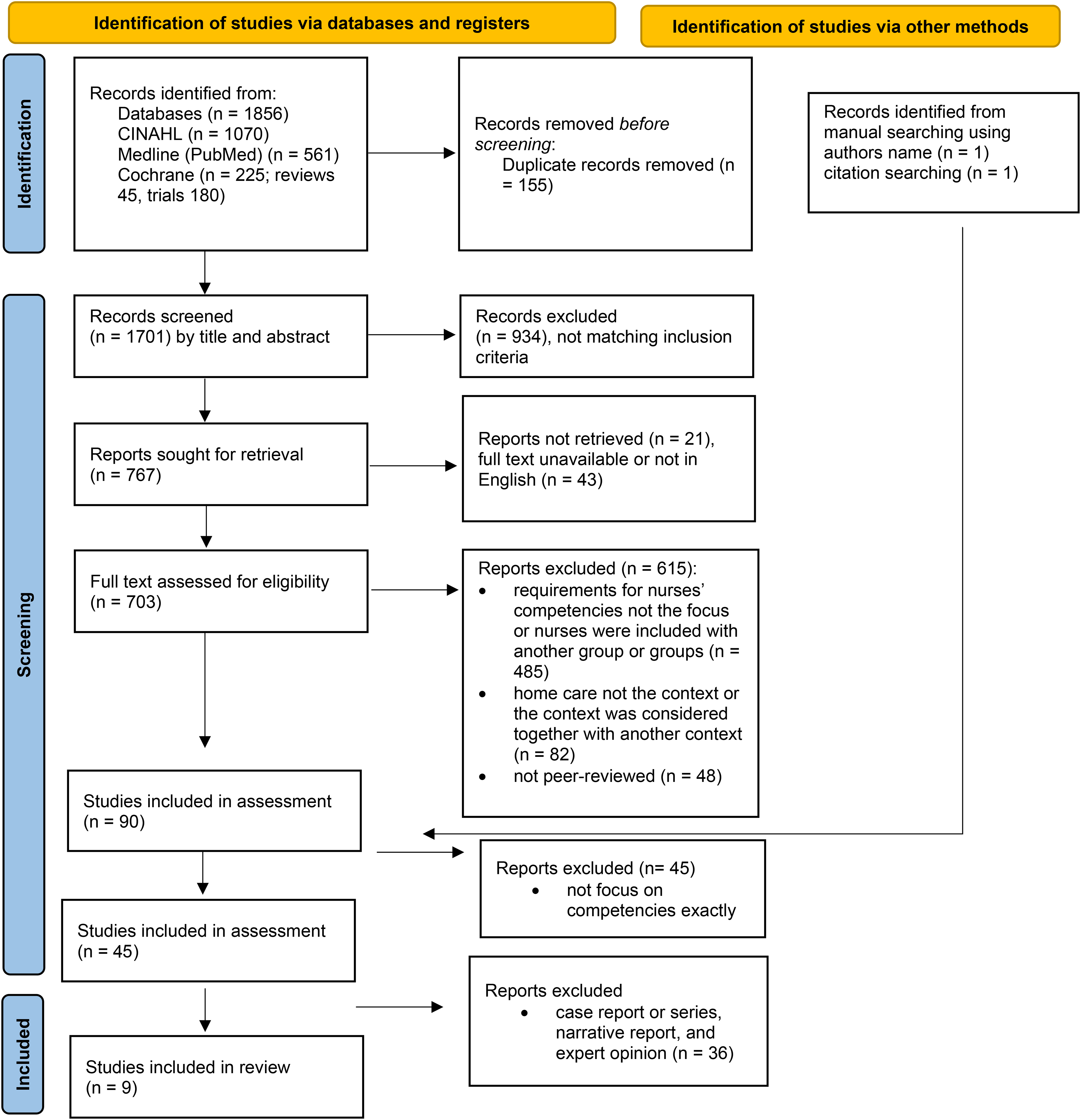
PRISMA flow chart of the selection of included studies.
The nine selected articles were read in full and assessed by both authors separately using the Joanna Briggs Institute's evaluation criteria. 31 A checklist was used for systematic reviews syntheses, 32 for qualitative studies 33 and for analytical cross-sectional studies. 34 The scales were in the range of 8–11, depending on the checklist. The alternatives of responses were yes, no, unclear and not applicable.
Data analysis and presentation
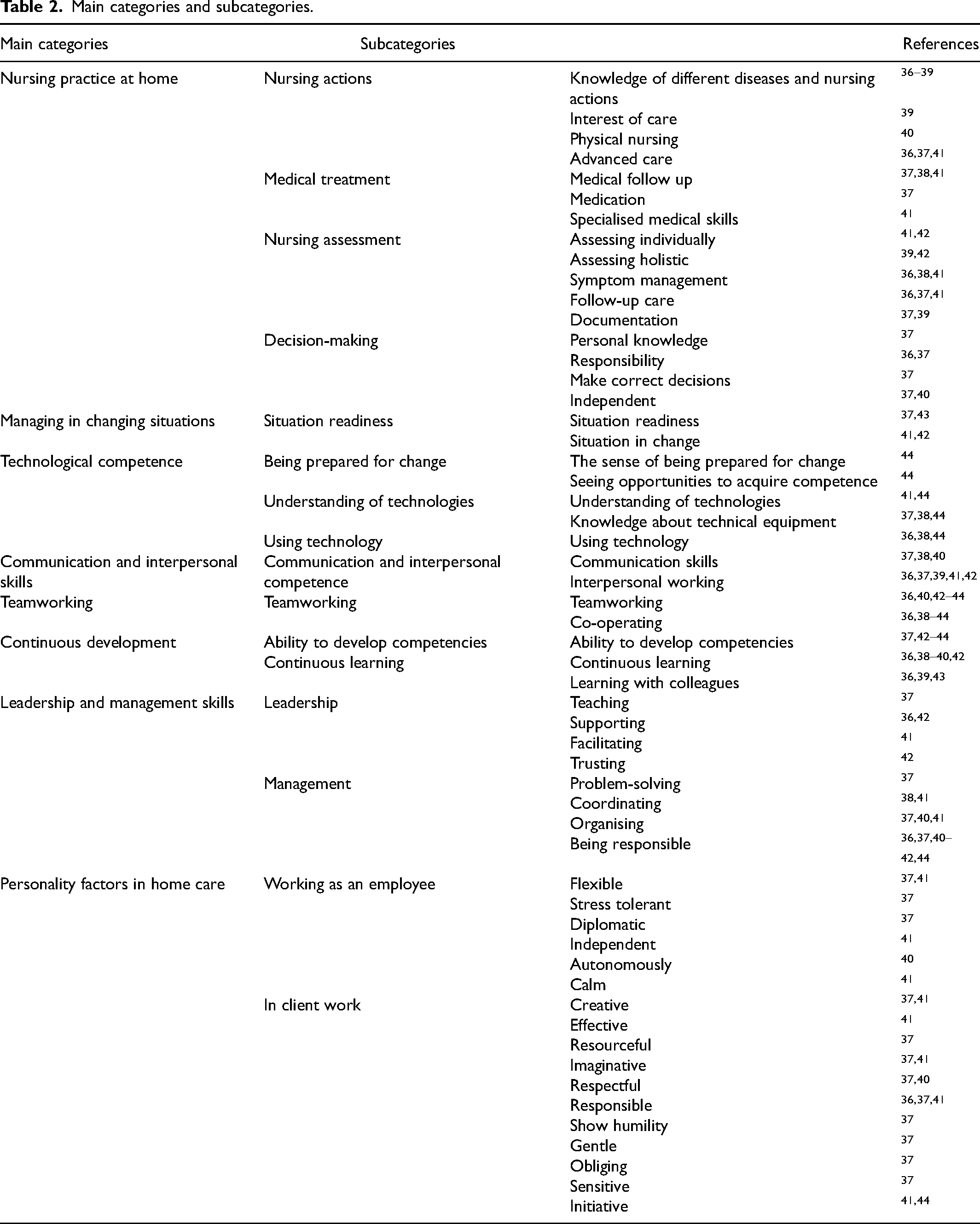
The content analysis was used to analyse data, 35 meaning units were extracted. Sentences were highlighted and condensed according to the aim of the study. Similar condensed sentences were grouped, and categories were created and named. The original expression of the studies was used to form categories. The single quantitative study's expressions in data were based of the results of most important skills for home nursing. In the single review article in the data, categorisation was based on the results of the analysis, not based on the separate results of individual articles, thus avoiding the duplication of results. The categories and subcategories were described and these were connected to primary sources 28 (Table 2).
Main categories and subcategories.
Ethical considerations
In this literature review, the authors followed good scientific practice and the ethical principles of the Declaration of Helsinki. 45 The design and process of the data search were executed and described. The articles in this review were selected from peer-reviewed scientific journals and were assessed by two authors separately. The appropriate references were used ethically and clearly presented.
Results
Nine articles were included for review. One of the articles was a review, seven were qualitative studies and one was a quantitative study (Table 3).
Characteristics of the articles included in the review.
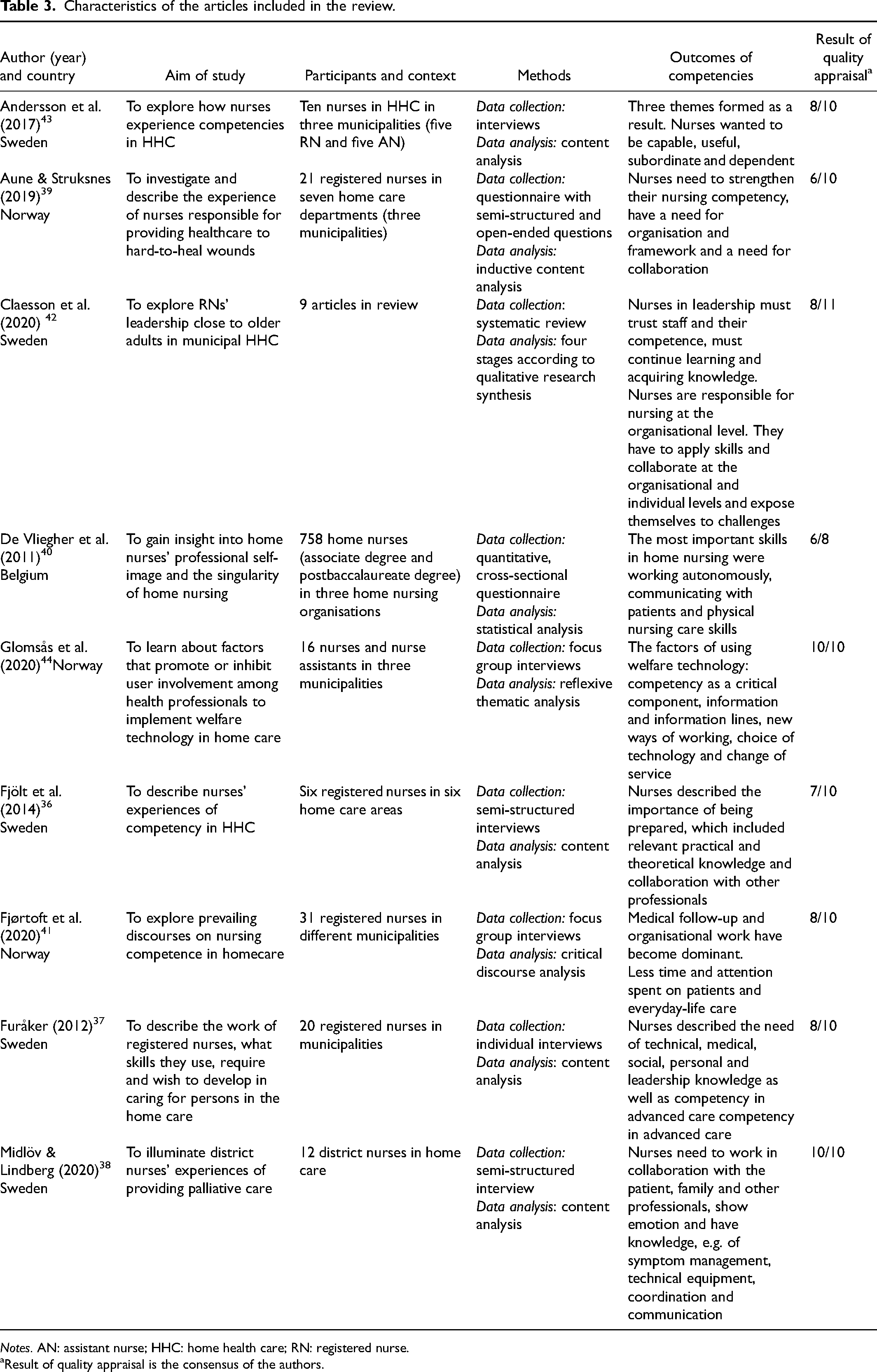
Notes. AN: assistant nurse; HHC: home health care; RN: registered nurse.
Result of quality appraisal is the consensus of the authors.
The articles originated from three countries: Sweden36–38,42,43; Norway39,41,44; and Belgium. 40 A single review article 42 included studies from the UK, Sweden, Norway and Canada.
Six studies described the competencies of registered nurses,36,37,39,41,43,44 one study those of district nurses 38 and one those of a registered home nurse. 40 Two studies included descriptions of both registered and assistant nurses’ competencies 43 or only nursing assistants’ competencies. 44 The review article 42 encompassed nine articles, of which five described the competencies of registered nurses, two of nurse specialists and two of district nurses. One article also included auxiliary nurses.
The sample sizes in the studies of this review were in the range of 6–31 nurses in the qualitative studies, 758 in the quantitative study and 4–20 nurses in the single review article (all qualitative studies).
Five studies referred to the concept ‘home care’,37–39,41,44 two ‘home healthcare’36,43 and one ‘home nursing’. 40 In the review article, there were five studies from home care, one from palliative home care, one from home healthcare, one from community palliative care and one from municipal home care services. 42
This review identified eight main competencies for nurses working in home care: nursing practice at home; managing in changing situations; technological competence; communication and interpersonal skills; teamworking; continuous development; leadership and management skills; and personality factors in home care.
Nursing practice at home
Nursing actions need professional competency comprising both knowledge and skills. 41 Nurses need a wide knowledge of different diseases and nursing actions in somatic, psychiatric and palliative care.37,38 They need, for example, the knowledge of functional impairments, 36 of dementia,36,37 of palliative care36–38 and of mental illness.36,37
Nurses experienced that it is important to have physical nursing care 40 and wound care skills. The competencies include both knowledge and training, but also an interest in care, for example, wound care. 39 In the home, patients were often more seriously ill, requiring advanced care36,37,41 and, increasingly, specialised knowledge and skills are required. 41
In the context of medical treatment competency, nurses mentioned medical follow-up in relation to diseases and symptoms,38,41 medical knowledge – both somatic and psychiatric in nature
37
– and specialised medical knowledge.
41
Nurses discussed their personal responsibility for more seriously ill patients in home care with new treatments and medical equipment. (A3)
Home care patients often spend long periods of time alone; hence, nurses need knowledge of symptom interpretation and management.36,38 Assessment is a complex task that requires both working skills and professional competence. 42 Assessing patients individually41,42 and holistically39,42 was important, as was recognising the individual situation of each patient and any changes they experienced. 41 The professional assessment included monitoring skills, using evidence-based knowledge, 36 and the need for follow-up care 41 and prevention, including orthopaedic assessment in relation to falls and evaluation 37 or prevention in wound care. 39 The careful documentation of care provision in connection with each visit was important.37,39
Nurses described their work in home care as independent. 41 They mentioned that working autonomously is an important skill. 40 The role of decision-making was emphasised because the nurses were working alone. The nurses described decision-making as relying on personal knowledge and responsibility. They needed training to make correct decisions, for example regarding drug treatment.36,37
Managing in changing situations
Responding to changing situations required situation readiness, 43 the competency to improve 37 and an ability to find good solutions. Nurses needed skills in perceiving patients’ home situations and prioritising acute concerns in the care of each individual patient. 41
Nurses typically serve the best interests of their patients and colleagues. 43 They must ask relevant questions for information 37 and feel confident to carry out their tasks.36,42,43 They must have the ability to intervene in situations where care is required, 42 notably when patients are seriously ill or new treatments and medical equipment demand high levels of skill and responsibility.36,44 However, increasing demands for care leave less time to deal with individual patients. 41
Technological competence
Increasingly advanced care demands high levels of technological knowledge 38 and skills38,44 to deliver optimal service to patients. For example, palliative care is becoming increasingly technical 38 and advanced technical knowledge is needed,37,41 for example in the use of new equipment, such as pain control infusion pumps and central lines in medical treatment 37 or medical robots. 44
The implementation of new technologies also changes the dialogue with patients and their next of kin as well as with other professionals. Nurses need to be prepared for change, make use of the opportunities to acquire technological competence and be ready to use technology. They need knowledge and understanding of technologies, 44 technical equipment38,44 and how to use them.36,44
Communication and interpersonal skills
Working in home care needs social knowledge, such as communication skills37,38,40 and collaborative skills. 41 Nurses need to know how to ask relevant questions, to communicate effectively with patients who have difficulty understanding or accepting their situation 37 or who come from other cultures, 38 to ensure that patients are not left alone at home without follow-up visits, 36 to discuss with patients and their relatives38–41 and to explain all aspects of the care they are providing. Nurses respond to individuals to ensure correct care processes, and they respond to individuals as a part of care. 37 They engage in mutual relationships, working together with colleagues, patients and their next of kin. 42
Teamworking
Teamwork is crucial in home care. 36 Nurses described working on a joint project, working together 41 and team collaboration, 38 cooperating with colleagues36,39,40,43 and staff 36 or with other healthcare providers,36,38,39,41 such as occupational therapists, physiotherapists, curators and priests. 38 Teamwork also involves collaborating at an organisational level 42 and with managers.40,42,43 In addition, for example, using welfare technology requires collaborating with IT experts and the suppliers of technology. 44
Continuous development
Continuous professional development for nurses involves information, 44 training39,43 and continuing education.39,40 Nurses need the ability to develop42,43 and knowledge to improve37,44 their competencies.
Continuous learning means that nurses also develop their competencies by learning with others, such as cooperating and sharing with colleagues36,37,39,43 and other professionals, e.g. clinics, hospitals,36,38 emergency units
37
and specialist agencies.36,37 Several nurses emphasised the importance of cooperating and sharing competencies with each other since this influenced their capacity to provide quality care and treatment. (A1)
Leadership and management skills
Leadership among nurses includes teaching the nursing staff, enrolled nurses and new colleagues, patients and their next of kin, and students. 37 Management involves organising and facilitating patient services,40,41 delegating nursing care, 37 coordinating care by consulting and planning home visits with doctors, 38 supporting colleagues36,42 and solving problems. 37 Leaders must be able to guide and advise their team members. 43
Registered nurses must trust their own and other nurses’ competencies
42
but they also have responsibility for the coordination of care38,40 and care planning,
37
complying with contracts of patients’ services.
41
Registered nurses are responsible for patient safety
42
and care,36,42 and nursing staff's working conditions at the organisational level.
42
The assessment process is a complex situation where RNs’ leadership requires that they use their whole being and all their senses in combination with professional competence and working skills. (A2)
Personality factors in home care
Nurses described the personality factors they need for working in home care both with client work and as an employee.
Nurses must be gentle, obliging, stress-tolerant, flexible37,41 as well as capable of working independently
41
and anonymously,
40
effective
41
and able to show humility and respect.
37
This means that they must also be resourceful,
37
imaginative, creative and able to devise solutions to new problems or situations.37,41 Registered nurses describe themselves as a guest in a person's home, which could be both satisfactory and demanding… being a guest means that invitation is needed and RN's must follow certain rules regarding behaviours, such as being respectful and obliging. (A1)
Other characteristics mentioned in the articles included being friendly,
41
sensitive, humble, diplomatic,
37
calm
41
and able to take initiative, e.g. to improve their competence with technology.
44
When they [nurses] talked about nurse competence, they linked professional knowledge and skills with personal attributes, for example being calm, friendly and flexible. (A8)
Discussion
The aim of this integrative review was to examine the literature results of the competencies required by nurses in home care. In this review, the articles mostly described the experiences of registered nurses. Only two of the articles also included the experiences of assistant nurses even though a large part of nursing professionals in community care consists of personnel with relatively low qualifications. 15
Nurses in home care must be competent, 41 having knowledge and ability. 42 To provide high-quality home care, nurses need both relevant theoretical and practical knowledge 36 and personal expertise 39 in different areas and contexts.37,42 The nursing practice at home needs holistic and evidence-based knowledge of different diseases 36 and skills to apply it in different situations. 43 Nursing assessment 42 and decision-making 36 are considered important because nurses work autonomously. 40 According to earlier reviews, nurses need critical thinking and problem-solving skills to make adequate assessments and able to work in problematic situations15,23 Patients in home care are more seriously ill 36 and their health conditions become increasingly demanding. 25
Nurses described themselves as guests. They must be sensitive and diplomatic in communicating with patients and their families. Many visits on duty, documentation and changing situations37. need organising and priority work. 41 The combined needs of patients and of the work community may lead to moral stress. 43 The working environment in patients’ homes is unique. 8 Travelling between patients’ geographical locations, lack of time and working in patients’ own homes require nurses to adjust to changing circumstances and ethical knowledge, experiences and creativity. 46
Nurses felt that they have less competency in technological skills than competency in care. 40 The confined competence has an influence on nurses’ attitudes and willingness using technology. 44 However, technological solutions improve the effectiveness of home care, 3 for example by saving time in administering medication. 47
In this review, nurses mentioned that developing competencies is difficult because of a lack of time and to have adequate knowledge could lead to increased stress and could impact job satisfaction. 36 They experienced that learning with other staff36–38 and colleagues36,37,39,43 provides one way to update knowledge alongside training39,43 and education.39,40 In the study by Hasson and Arnetz, 24 home-based nursing staff also report lack of knowledge. Professional development is a required competency in home care. 23 Multiprofessional discussion and consultation has also been identified as an important role in caring for older people by other studies. 48
This review completes previous reviews, where there were some differences. In their wide scoping review, Rusli et al. 23 included 64 articles published in 1992–2020 about home-based nursing with several methods of data collection from different countries. In their review, Bing-Johnson et al. 15 included both articles from Nordic countries published in 2000–2014 and national documents in community care. In the present review, articles were mainly from Nordic countries except for one from Belgium and a review article that also included articles from the United Kingdom and Canada. This review was limited to studies published in 2011–2023 and only in the home care environment; it describes nurses’ own experiences of required competencies via peer-reviewed scientific journals excluding case reports or series, narrative reports and expert opinions. This review also included an assessment of studies.
The results of this review are similar to those of previous reviews, although in the review by Rusli's et al., 23 the quality and safety category indicated that nurses must have knowledge of the quality of care and safety. In addition, technological solutions, e.g. providing a telehealth service, must be safe and ensure care. In the present review, personality factors in home care were also included in the results of nurses’ competence requirements. This category included the characteristics and attitudes that nurses mentioned in the articles as playing an important role in their nursing ability, being a competent nurse or the personal attributes that they linked to their knowledge and skills, 41 and which they mentioned as specific characteristics that they utilise in home care 37 or as professional attitudes.40,44 These characters are included in competence categories in early studies. 49
Conclusions
The competencies in this review included eight categories of knowledge, skills, attitudes and values that nurses require for work in home care. The review included studies from five countries. It is important to use these results in practice to understand that there are differences in home care service organisations between and within countries. These differences have effects on professionals’ competence requirements.
This review reported updated information with earlier reviews to use developing continuous learning and competence development in home care units. It is important that competence development could be a part of daily work. Adequate knowledge and skills could have an effect on job satisfaction. However, different solutions and practices need to be found to develop competencies because of lack of time in daily work. A competent nursing staff is important for providing quality services and nursing in home care and allowing to support people at living at home. Continuing changes in home care services need updating competence but also gaining new knowledge.. The results of this review will also be used for education and training development. This review provides information about the content of training.
Registered and practical nurses are the largest professional group working in home care and it is important to understand their experiences of competence requirements. In this review, only two studies described both. More knowledge is needed of nurses’ experiences of competencies, especially practical nurses’ competence requirements, as they work as the largest professional team in home care.
Methodological limitations and strengths
The study design included studies with different methodologies. There is always a possibility that some articles were not found in the electronic literature search. The review included only articles that had been published in English. To solve these limitations, the first author planned the search strategy together with an information specialist and searches were conducted separately using the database's own MeSH terms and common search terms. The PRISMA toolkit was used in selecting process. 29
The selected articles were read in full by both authors and assessed separately based on the authors’ own understanding according to the Joanna Briggs Institute criteria. The tools for different methods were used appropriately. The review followed Whittemore and Knafl's framework. 28 The definitions of ‘nurse’, ‘home care’ and ‘competence’ varied in studies, and it is possible that some articles were not found. The differences in definitions made the analysis challenging but the authors’ discussed evaluations of the articles and the findings of the analysis strengthened it.
Footnotes
Acknowledgements
We would like to thank the information specialists of Tampere University supporting developing search strategies and advising us to use databases.
Author contributions
The first author performed the data search. Both authors performed data evaluation, analysis, interpretation and drafted the manuscript for submission to the journal.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.