
Abstract
It is extremely important to have an overall view of nurses’ well-being and anxiety levels during the COVID-19 pandemic to support the well-being and working conditions of workers in optimal ways in future crises. The aim of the study was to describe changes in the anxiety levels of nurses from the beginning of the COVID-19 pandemic to a time point 18 months later, and to describe how the working conditions, interactions between workers, psychological distress, and managers’ actions were associated with the anxiety of nursing staff. The repeated cross-sectional survey was distributed to nurses at two Finnish hospitals. The mean anxiety scores of nurses increased over the examined 18-month period, but still indicated mild anxiety at both time points. Working conditions, interactions between workers, and psychological distress were associated with anxiety. At both measurement points, the nurses who did not receive support from their manager had higher levels of anxiety compared to those who received support. Hospital organizations can take advantage of the results when preparing for new pandemics and producing concrete plans to support nurses’ mental health and coping at work.
Background
As nurses have been the main force in the fight against COVID-19, they have been exposed to anxiety and constant psychological distress.1–3 COVID-19 has caused unexpected situations, changes in hospitals’ daily routines, and unknown threats and fears, which in turn may have exacerbated this anxiety.4,5 Therefore, it is extremely important to pay close attention to nurses’ anxiety levels caused by the COVID-19 pandemic to support nurses beyond the COVID-19 crisis by any means possible.
The pandemic has progressed in different stages and waves, each of which has affected the healthcare capacity and, more importantly, the anxiety level of hospital workers. 6 In 2022, Lixia et al. analysed the psychological status of hospital workers at the late stage of the COVID-19 outbreak when the epidemic peak had ended in China, in April 2020. 7 The results showed that despite the late stage, hospital workers still had extensive anxiety, depression, and physical symptoms. 7 Moreover, Maunder et al. in 2021 conducted a study on hospital workers before the peak of the second wave in Canada (autumn 2020) and immediately after a peak in cases (winter 2021). The results showed a high psychological burden that increased as the pandemic continued along with emotional exhaustion that varied by occupational role, being the highest among nurses. 8 In addition, in 2022, Wynter et al. compared the well-being of hospital workers at two different time points during the COVID-19 pandemic in Australia: between wave 1 (May–June 2020) and wave 2 (October–December 2020). They found that depression, anxiety, and stress scores were higher during the second wave. 9
During the waves of the pandemic, COVID-19-related job stressors and intense and heavy working conditions may have resulted in compound psychological distress and anxiety.6,10 Further, job dissatisfaction, a higher number of COVID-19 cases at one's work facility, concerns about becoming infected at work, and feeling unprepared for the pandemic have been found to be strongly associated with nurses’ distress.2,10 Moreover, nurses have expressed decreased interactions with colleagues when their exhaustion and psychological distress continued; this was because all support had to be allocated to patients. 1 In addition, whether the patient has a suspected or confirmed COVID-19 infection has also been found to affect nurses’ level of anxiety, in that anxiety is significantly higher in nurses who work with patients suspected to have the infection. 2
During the COVID-19 pandemic, nurses have reported not only anxiety but also overwhelming grief, and even guilt and post-traumatic stress disorder. 11 This emphasizes the role of nursing managers’ support and actions that are paramount for hospital nurses to cope with the COVID-19 pandemic. 12 However, recent studies revealed some lack of managerial support during the COVID-19 pandemic. The results showed that hospital workers’ job satisfaction and well-being were not supported enough – or, in some cases, at all – and hospital staff experienced a lack of encouragement from their manager and needed more discussions and information about what was to come. 12 Moreover, an incompetent and less supportive manager is perceived to cause more anxiety. 1 Furthermore, managers’ internal crisis communication style needs development and should include more emotional elements and consideration of the diversity of units and professions. 13 It is even more important that, during a crisis such as COVID-19, the basic daily management practice tasks are performed – encouraging and listening to workers, building a common understanding, providing information, and being visible to them. 12
Along with anxiety- and management-related challenges, the changes and stressors caused by the COVID-19 pandemic have reduced work satisfaction and increased nurses’ turnover intention.14–16 This is an urgent concern that needs to be addressed. A recent study found that during the COVID-19 pandemic, good resilience promoted nurses’ high-quality care and enhanced their job satisfaction, which in turn reduced their intentions to leave nursing. 16 During the pandemic, it is essential to improve nurses’ working conditions to ensure their work engagement. Consequently, it is important that healthcare managers foster a resilient workplace and reinforce positive coping strategies among nurses. 17
Follow-up research on nurses’ anxiety caused by COVID-19 is limited and scant, and the published studies mainly describe anxiety that occurred at a certain point in time. To address this gap, we investigated nurses’ anxiety levels in the early stage of the COVID-19 pandemic and 18 months later. It is important to have an overall view of nurses’ well-being and anxiety levels during the entire COVID-19 pandemic to support nurses’ well-being and working conditions in optimal ways, also beyond the pandemic.
Aim
The primary aim of the study was to describe the changes in the anxiety levels of Finnish hospital nurses from the beginning of the COVID-19 pandemic (April–May 2020) to a time point 18 months later (November–December 2021). The secondary aim was to describe how the working conditions, interactions between workers, psychological distress, and managers’ actions are associated with the anxiety of nursing staff.
Methods
Data collection
The repeated cross-sectional survey was distributed to nursing staff at one Finnish university hospital and one central hospital. The first dataset was collected during the early stages (April–May 2020) of the COVID-19 pandemic, and the second dataset was collected 18 months later (November–December 2021). Both datasets were collected from the same hospitals. Nursing staff includes Registered Nurses (RN) and Practical Nurses. In Finland, RNs have a 3.5-year Bachelor level education provided by Universities of Applied Sciences. The practical nurses have 2 years of vocational training.
The nurses could respond to the survey voluntarily and anonymously via the Webropol system, which is a web-based tool to collect research data (webropol.com). The Webropol system made a reply link, which was sent to the nursing managers, who forwarded it to their nurses with an email message. This ensured the anonymity of the participant nurses. In addition, a reminder was sent to answer the survey through the managers, while it was not possible to send personal reminders when it was impossible to trace the non-responders.
Study instruments
The Generalized Anxiety Disorder 7-item scale (GAD-7) was used to measure hospital nurses’ anxiety during the COVID-19 pandemic. The GAD-7 is a self-rated scale used to evaluate the severity of anxiety symptoms.18,19 The scale is sensitive to a noticeable change in anxiety severity and it is easy to score. 20 The scale has also demonstrated high reliability and validity in many earlier studies.19–22 In this study, the Cronbach's alpha coefficient of the GAD-7 was 0.90. Every item is rated on a 4-point scale (0 = not at all, 1 = some of the time, 2 = more than half of the time, 3 = nearly every day), and the total scores are in the range of 0–21 points.
The questionnaire also comprised five groups of items based on earlier literature. The items’ validity and reliability were tested in an earlier study.5,12 The items were as follows: (1) worker's background factors: sex, age, occupational group, etc.; (2) changes in working conditions: remote working and transfer to a new work unit; (3) interaction between co-workers: cooperation between co-workers and professions, and team spirit; (4) psychological distress: work-related stress, difficulty concentrating at work, work-related thoughts outside working hours, and a workload that threatens physical and psychological health; and (5) manager's actions: support, encouragement, and discussing COVID-19-related worries. For each item, the response alternatives were ‘yes’, ‘uncertain’, and ‘no’. The respondents were also given an opportunity to share their experiences of the COVID-19 pandemic. However, these results are not reported in the present study.
Statistical analysis
The data were analysed statistically using SPSS 26 software. Differences were considered statistically significant with a p-value < 0.05. 23 The descriptive statistics include frequency and percentage distributions, standard deviations, range (min–max), and means. According to earlier studies, the GAD-7 scale points can be divided into four anxiety levels: normal (0–4.99); mild (5.0–9.99); moderate (10–14.99); and severe (15–21).19–22
The associations between anxiety levels and background factors (demographic factors, changes in work conditions, interaction between co-workers, psychological distress, and manager's actions) were analysed using a chi-square test (χ2), independent t-test, and two-way ANOVA with Bonferroni-corrected pairwise comparisons. For the analysis, the nurses were categorized into four age groups (18–34, 35–44, 45–54, and ≥55 years), three educational levels (university, university of applied sciences, and other), and four work experience groups (0–3, 4–10, 11–20, ≥21 years). The amount of remote work was categorized into three groups (100%, approximately 50%, 0%).
Multivariable logistic regression with the enter method was used to examine the background factors independently associated with clinically significant anxiety. The regression model includes datasets for both years (2020 and 2021). Earlier studies have reported that 10 points is the cut-off point for clinically significant anxiety, and this was also used as the cut-off point in the present study.19,24 The logistic regression analysis includes all background factors that are shown in Tables 1 and 3. The year variable (2020 and 2021) was also added to the regression model. The associations between anxiety and background risk factors are presented as odd ratios (OR) and 95% confidence intervals (CI).
The nurses’ background factors and total GAD-7 scores in 2020 and 2021 datasets.
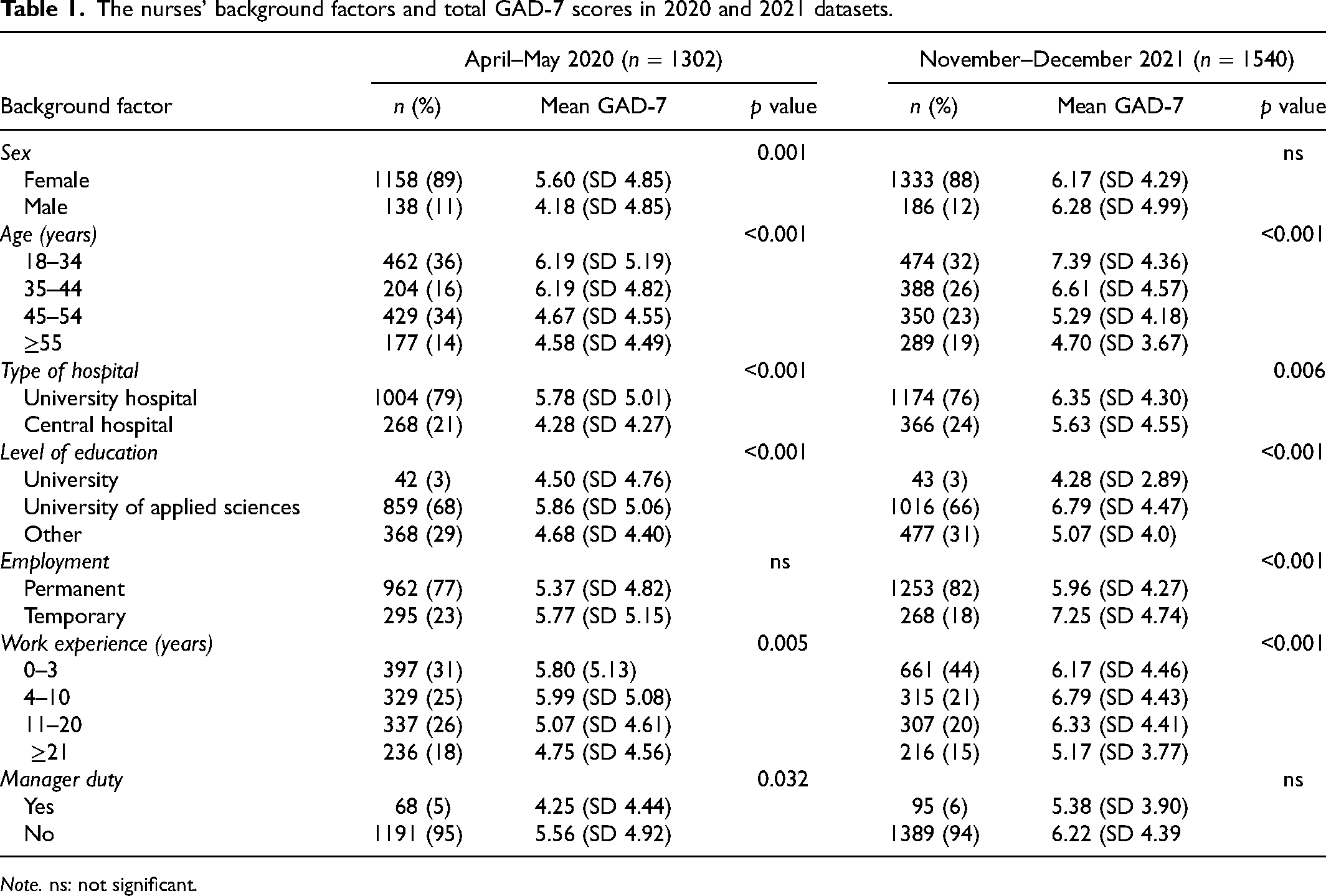
Note. ns: not significant.
Ethical approval
Written permission to conduct the research was obtained from both hospitals. According to Finnish ethical guidelines and research legislation, a review by an institutional ethics committee was not required for this study. 45 Participation in this study was voluntary and the participating hospital nurses were informed of the study in writing. They also had an opportunity to ask for more information from the researchers and withdraw from the study at any time without providing a reason. No individual respondents can be identified based on their responses.
Results
Participants
The total sample size was 2842 (April–May 2020: n = 1302; November–December 2021: n = 1540), yielding a response rate of 19% and 24%, respectively. Most of the participants were women (n = 2,491, 89%), permanent employees (n = 2,215, 80%), and worked at the university hospital (n = 2,178, 78%). The majority had work experience of 0–10 years (n = 1,702, 60%). Detailed descriptive background variables are shown in Table 1.
The hospital nurses’ anxiety level
According to our results, the nurses experienced mild anxiety at the 2020 and 2021 time points. However, their GAD-7 score increased significantly between the years. In 2020, the total mean GAD-7 score was 5.46 (SD 4.90, range 0–21), whereas in 2021, the GAD-7 mean was 6.18 (SD 4.37, range 0–21) (p = 0.023).
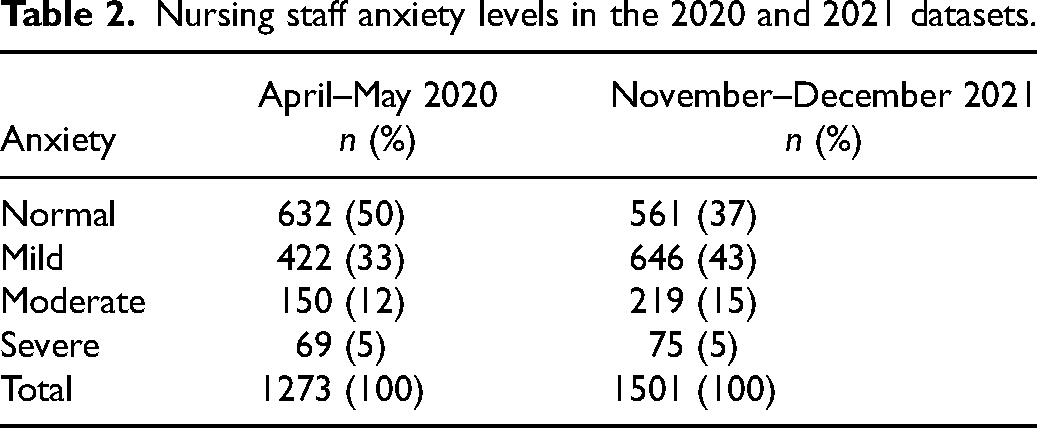
At the beginning of the COVID-19 pandemic in 2020, 50% (n = 632) of the nurses had no anxiety, whereas 18 months later, 37% (n = 561) reported no anxiety. In the early stages of the COVID-19 outbreak in 2020, 33% (n = 422) of the nurses had mild anxiety levels and in 2021, the corresponding rate was 43% (n = 646). Over the 18-month follow-up, moderate anxiety increased among the nurses: in 2020, 12% (n = 150) and in 2021, 15% (n = 219) had moderate anxiety. In 2020, 5% (n = 69) and in 2021, 5% (n = 75) had severe anxiety (Table 2).
Nursing staff anxiety levels in the 2020 and 2021 datasets.
Association of background factors with nurses’ anxiety
Demographic data
In the early stages of the pandemic in 2020, female nurses reported significantly higher anxiety levels compared to their male colleagues (mean 5.60 vs. 4.18, p = 0.001). In 2021, female and male nurses had a mild anxiety level (mean 6.17 vs. 6.28, p = 0.76), and there were no statistically significant differences between the sexes. In 2020, nurses in the 18–34-year and 35–44-year age categories had significantly more anxiety than the older (45–54 and ≥55) nurses (p < 0.001). The youngest workers (aged 18–34 years) in 2021 continued to report the highest anxiety levels (mean 7.39, SD 4.36) and those aged ≥55 years the lowest anxiety levels (mean 4.70, SD 3.67, p < 0.001 for age group difference) (Table 1).
The university hospital nurses had significantly higher anxiety levels compared to those of the central hospital nurses in 2020 (mean 5.78 vs. 4.28, p < 0.001) and 2021 (mean 6.35 vs. 5.63, p < 0.001). In 2020, nurses with a degree from a university of applied sciences had significantly higher anxiety levels compared to the nurses with a degree from a university or other educational levels (mean 5.86 vs. 4.50 and 4.68, p < 0.001). The results were similar 18 months later in 2021 (mean 6.79 vs. 4.28 and 5.07, p < 0.001) (Table 1).
In 2020, there was no significant difference between the permanent (mean 5.37) and temporary employees’ (mean 5.77) total anxiety means (p = 0.21). Meanwhile, 18 months later, anxiety was significantly higher among temporary workers compared to permanent workers (mean 7.25 vs. 5.96, p < 0.001). In 2020, the nurses with 4–10 years of work experience reported significantly more anxiety than those who had ≥21 years of work experience (mean 5.99 vs. 4.75, p = 0.005). The results were similar in 2021 (mean 6.79 vs. 5.17, p < 0.001). Nurses with a managerial duty experienced significantly less anxiety than others in 2020 (mean 4.25 vs. 5.56, p 0.032) but this difference was no longer found in 2021 (mean 5.38 vs. 6.22, p = 0.072) (Table 1).
Changes in work conditions
In 2020, nurses who worked remotely for approximately 50% of their total working hours had significantly less anxiety than those who worked fully remotely or did not work remotely at all (mean 3.93 vs. 4.25 and 5.57, p = 0.020). The results were similar 18 months later (mean 4.71 vs. 7.28 and 6.28, p < 0.001) (Table 3).
Nurses GAD-7 anxiety scale associations with changes in work conditions, interaction between workers, psychological distress, and manager’s actions.
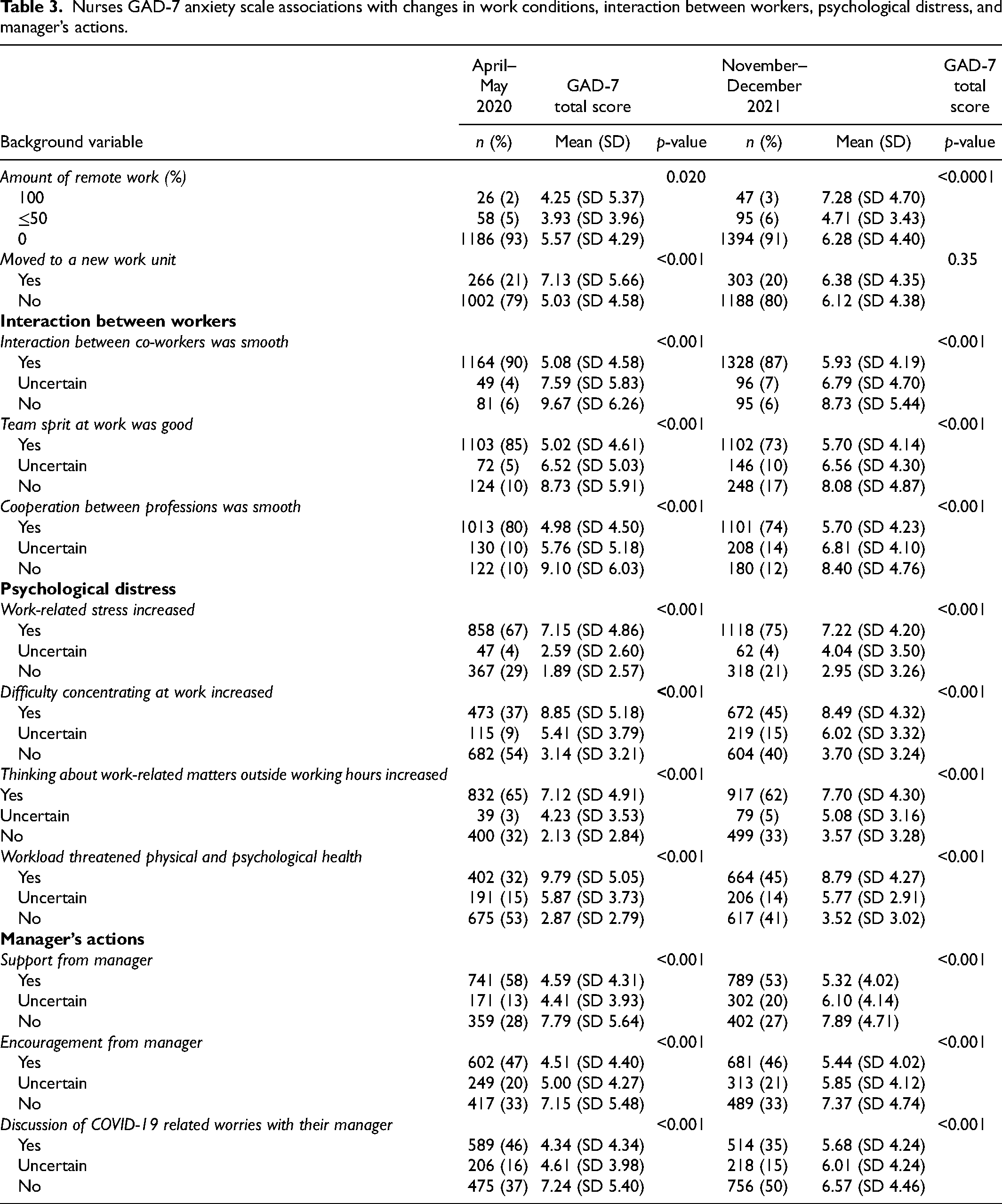
Nurses who had moved to a new work unit in the spring of 2020 had significantly more anxiety than those who had stayed in a familiar unit (mean 7.13 vs. 5.03, p < 0.001). Eighteen months later, moving to a new work unit was not associated with nurses’ anxiety (mean 6.38 vs. 6.12, p = 0.35) (Table 3).
Interaction between co-workers
In 2020 and 2021, 90% (n = 1164) and 87% (n = 1328) of the nurses, respectively, reported feeling that interactions between co-workers were smooth during the COVID-19 pandemic (p < 0.001). In 2020, those nurses reporting smooth interactions with co-workers experienced significantly less anxiety compared to those who did not find the interactions smooth (mean 5.08 vs. 9.67, p < 0.001). The results were similar 18 months later (mean 5.93 vs. 8.73, p < 0.001) (Table 3).
In 2020, 85% (n = 1103) of the nurses felt that the team spirit was good during the COVID-19 pandemic compared to 73% (n = 1102) during the later stages of the pandemic in 2021 (p < 0.001). Those nurses who reported finding the team spirit good had less anxiety than those who felt it was poor in both 2020 (mean 5.02 vs. 8.73, p < 0.001) and 2021 (mean 5.70 vs. 8.08, p < 0.001) (Table 3).
The experience of smooth cooperation between professions decreased from 80% (n = 1013) to 74% (n = 1101) between the two time points (p < 0.001). Those who felt that cooperation was smooth had less anxiety compared to those who were uncertain or experienced poor cooperation in both 2020 (mean 4.98 vs. 9.10, p < 0.001) and 2021 (mean 5.70 vs. 8.40, p < 0.001) (Table 3).
Psychological distress
In 2020 and 201, 67% (n = 858) and 75% (n = 1118) of the nurses, respectively, felt that their work-related stress had increased during the COVID-19 pandemic (p < 0.001). In 2020, workers who felt that work-related stress had increased during the pandemic experienced significantly more anxiety than those whose stress levels had not increased (mean 7.15 vs. 1.89, p < 0.001), which was similar to the result in 2021 (mean 7.22 vs. 2.95, p < 0.001) (Table 3).
In 2020 and 2021, 37% (n = 473) and 45% (n = 672) of the nurses, respectively, experienced more difficulties concentrating at work during the COVID-19 outbreak (p < 0.001). The nurses who had experienced increasing difficulty concentrating also had more anxiety in both 2020 (mean 8.85 vs. 3.14, p < 0.001) and 2021 (mean 8.49 vs. 3.70, p < 0.001) (Table 3).
In 2020, 65% (n = 832) of the nurses reported an increase in their work-related thoughts during their free time, whereas the corresponding rate in 2021 was 62% (n = 917) (p < 0.001). Those nurses who reported thinking about work-related issues in their free time had higher anxiety levels compared to others in both 2020 (mean 7.12 vs. 2.13, p < 0.001) and 2021 (mean 7.70 vs. 3.57 p < 0.001) (Table 3).
In 2020 and 2021, 32% (n = 402) and 45% (n = 664) of the nurses felt that their physical and psychological workload had increased during the COVID-19 outbreak so much that it threatened their health (p < 0.001). The nurses whose work-related physical and psychological workload had increased had higher anxiety levels compared to the others in both 2020 (mean 9.79 vs. 2.87, p < 0.001) and 2021 (mean 8.79 vs. 3.52, p < 0.001) (Table 3).
Manager's actions
In 2020 and 2021, 58% (n = 741) and 53% (n = 789) of the nurses, respectively, felt that they had received support from their managers (p < 0.001). At both measurement points, the nurses who did not receive support from their manager had more anxiety compared to those who received support (2020 mean 7.79 vs. 4.59, p < 0.001; 2021 mean 7.89 vs. 5.32, p < 0.001). In 2020 and 2021, 47% (n = 602) and 46% (n = 681) of the nurses, respectively, felt that they received encouragement from their manager (p < 0.001). They also experienced less anxiety than those who felt that they were not encouraged (2020 mean 4.51 vs. 7.15, p < 0.001; 2021 mean 5.44 vs. 7.37, p < 0.001) (Table 3).
In 2020 and 2021, 46% (n = 589) and 35% (n = 514) of nurses, respectively, felt that they were able to discuss their COVID-19-related worries with their manager (p < 0.001). Those who had been able to discuss their COVID-19-related worries with their manager had less anxiety in both 2020 (mean 5.68 vs. 7.24, p < 0.001) and 2021 (mean 4.34 vs. 7.24, p < 0.001) (Table 3).
Risk factors of nurses’ clinically significant anxiety
According to the multivariable logistic regression analysis, the independent risk factors that predicted the nurses’ clinically significant anxiety (GAD-7 ≥10) during the COVID-19 outbreak were short duration of work experience, working in a university hospital, difficulty concentrating at work, and physical and psychological workload threatening one's health (Table 4). The nurses’ likelihood of experiencing anxiety decreased with higher working experience. The nurses with work experience ≥21 years were less likely to experience anxiety than those with 0–10 years of work experience (OR 1.92–1.95, 95% CI 1.34–2.82, p < 0.001). The nurses at the university hospital were more likely to experience anxiety than those working at the central hospital (OR 1.38, 95% CI 1.01–1.87, p = 0.037). Work-related concentrating difficulties increased the nurses’ likelihood of having anxiety (OR 1.49, 95% CI 1.10–2.01, p = 0.010). In addition, the nurses who reported that the work-related physical and psychological burden threatened their health were more likely to have anxiety than those who had not been overburdened (OR 2.97, 95% CI 2.15–4.09, p < 0.001) (Table 4).
Logistic regression model to predict variables associated with nurses’ clinically significant anxiety (GAD-7 ≥10).*
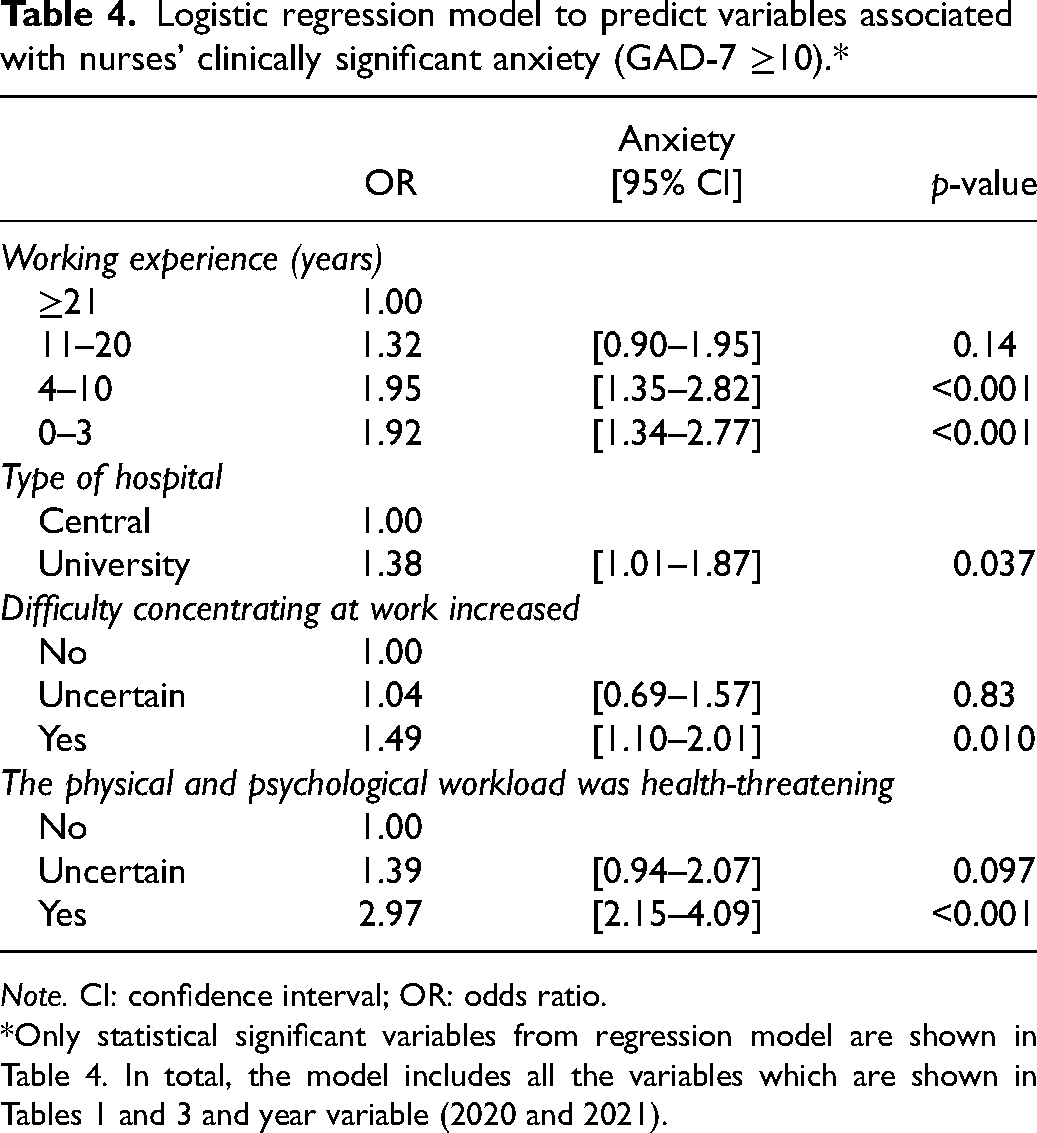
Note. CI: confidence interval; OR: odds ratio.
*Only statistical significant variables from regression model are shown in Table 4. In total, the model includes all the variables which are shown in Tables 1 and 3 and year variable (2020 and 2021).
Discussion
This study provides new evidence about the anxiety experienced by hospital nurses during the different stages and waves of the COVID-19 pandemic. The fact that there is little previous research evidence available on the anxiety levels of Nordic nurses during the COVID-19 pandemic also contributes to the novelty value of this study. Based on our study results, Finnish nurses’ total anxiety mean scores increased over the 18-month period, but still indicated mild anxiety in both time points. However, the number of nurses whose level of anxiety was normal compared those those who had a GAD-7 ≥5 decreased 13% between the two time points. In addition, the number of nurses with mild anxiety increased by 10% between the years (Table 2). This can been seen as a natural reaction in a prolonged situation. However, it is unclear if that is a permanent or temporary reaction. More specifically, in Finnish hospitals during the early stages of the COVID-19 outbreak (spring 2020), 50% of nurses experienced mild to severe anxiety, while in late 2021, the figure had risen to 63%. A total of 17%–20% of Finnish nurses experienced moderate or severe anxiety (GAD-7 ≥10), which means that they had clinically significant anxiety. It is obvious that this group of nurses would have needed targeted and individual interventions. This study also revealed that nurses had higher levels of anxiety compared to the Finnish population on average. Overall, 13.3% of the total Finnish population has been found to have mild symptoms of anxiety, 6.7% moderate symptoms of anxiety, and 2.5% severe symptoms of anxiety. 24 Furthermore, another Finnish study revealed that the proportion of clinically anxious men was 2.8% and women was 4.4%. 25
Earlier COVID outbreak studies have shown the prevalence of nurses’ anxiety to be in the range of 22%–85.6%.26–33 Compared to these results, Finnish nurses had lower levels of anxiety during the COVID-19 pandemic than their colleagues worldwide. One explanation for this finding is that, in Finland, the COVID-19 outbreak was not extremely severe and the number of COVID-19 patients in hospitals was moderate.5,34 Compared to other Nordic countries, Finnish nurses were found to have higher levels of anxiety than their Danish and Norwegian colleagues during the COVID-19 pandemic.35–37
At the early stage of the COVID-19 pandemic, female nurses had significantly higher levels of anxiety than their male colleagues. Studies have shown that women have experienced more anxiety and other psychological reactions than men during the COVID-19 outbreak.27,38 As the COVID-19 outbreak continued, there was no longer a difference between the sexes. The results of this study confirm those of an earlier study5,31 that found that younger workers with less work experience were more susceptible to the burden of expectational situations, and their need for support should receive special attention.5,31 Older age and longer work experience strengthen workers’ confidence in managing a new situation, and they also have more knowledge and better self-regulation. 31 Saeedi and colleagues also noted that older and more highly educated nurses used more problem-oriented strategies than younger nurses. 31 The results of this study also confirm that during the COVID-19 pandemic, managers experienced the least anxiety.5,39
During the COVID-19 outbreak, the amount of remote work increased considerably. Our results showed that hybrid working time (approximately 50% of remote work) seems to protect nurses against anxiety. This may be one of the most important factors promoting hospital workers’ mental well-being. Telemedicine and other technical innovations enable a new way to treat patients. This study's results also showed that working in a university hospital increased the risk of anxiety. In 2021, Mattila et al. pointed out that working at a university hospital requires highly specialized expertise and skills to manage complex treatments, which can expose nurses to more changes in their work than in a central hospital setting. 5 University hospitals also treat the most severely ill patients, which may increase nurses’ anxiety risk.
Knowledge of the COVID-19 virus has increased, and the related treatment protocols have become well-established. Therefore, based on our study results, it is alarming that hospital nurses’ work-related stress, work-related concentration difficulties, work-related thoughts during their free time, and physical and psychological workload all increased in the 18-month period. The logistic regression analysis showed that difficulty concentrating at work and physical and psychological workload are the risk factors that predict an increase in clinically significant anxiety. This is consistent with earlier studies showing a high psychological burden and emotional exhaustion as the pandemic continued.7–9,28 Earlier studies emphasized relationships between positive mental health and social support, coping behaviours, and resilience.8,9 According to the results, constant interaction between different professional groups and teamwork can reduce the experience of anxiety. In 2021, the study by Teo et al. indicated that if teams worked well together, workers were significantly less anxious. 39 It is important to strengthen working communities so that they have resilience to cope with future crises. It is worth noting that managers’ actions slightly decreased over the 18-month period. This is an alarming trend because it is known that managers’ actions, such as support and encouragement, have a significant effect on the anxiety levels of workers. 12 This study's results show that levels of anxiety were lower among those who felt they had received support, encouragement, and an opportunity to discuss their COVID-19-related worries with their manager. According to our view, managers did not have sufficient leadership skills in these exceptional circumstances. This should be considered in future management training.
The results of this study show that the anxiety of nurses did not decrease as the pandemic continued. However, serious anxiety did not increase between the two time points, but still one-fifth of the nurses experienced clinically significant anxiety. In addition, it seems that the ability of hospitals to identify and especially to offer support interventions has been poor as the pandemic has continued. Consequently, there is a risk that the COVID-19 pandemic will leave staff with prolonged anxiety symptoms, stress, and overload, which may threaten their ability to work. This is a serious signal to managers, indicating that attention should be paid to the mental well-being of hospital workers and that proactive methods should be introduced to strengthen workers’ resilience and positive coping strategies.1,8 It is also known that people with symptoms of GAD utilize healthcare services more than other groups.25,40 Based on the results of our study, we argue that symptoms of GAD in nurses lead to increased absences from work, which are expensive for the employer and cause human suffering to the worker. Employers should be interested in the well-being of their staff both during and beyond the COVID-19 pandemic. We recommend that hospitals improve interventions that support the psychological resilience of workers in case of future pandemics and crises.
As Vanhaecht et al. have noted, the COVID-19 outbreak required major adaptations from healthcare organizations and their workers. 41 Our study indicates that the COVID-19 outbreak has a long-term impact: nurses have been subjected to a lot of uncertainty, stress, and anxiety, and they have not been able to recover from the crisis. Therefore, future studies are recommended for follow-up, and there is a need for longitudinal research to examine the long-term effects of the COVID-19 pandemic, mitigate the anxiety and stress due to the COVID-19 pandemic, and address other potential future crises.
Limitations
This study has some limitations. First, the sample size was moderate, and the response rate was relatively low, which might add to the response bias and limit the generalizability of the results. However, the response rates of the present study were in line with response rates from earlier COVID-19 studies.5,12,39,42,43 In addition, web-based data collection may have an impact on the response rate, as web-based surveys are known to reduce response rates. 44 Not having any personal contact with the respondents might explain the low response rate. COVID-19 outbreak also caused extra workload for the nurses, which probably decreased their willingness to participate in the study. Second, we do not know the baseline anxiety level of the respondents or how many of them had been previously diagnosed with clinical anxiety. Furthermore, we have only been able to compare the level of anxiety with the general level of the Finnish adult population. Third, the study design was repeated cross-sectionally, showing the anxiety at the time the respondents filled out the questionnaire. It was not possible to connect the results at the individual level between the sampling points. Because there were partly different respondents in two datasets, it limited the examination of changes at the individual level between the two time points. However, this study provides important and marginally published follow-up information concerning nurses’ mental health and associated factors during the COVID-19 outbreak.
Conclusion
It is obvious that hospital nurses’ anxiety has been prolonged, and this might have many serious consequences for their mental health. Consequently, this may cause serious and long-term problems for healthcare organizations. Moreover, the COVID-19 outbreak seems to cause global trauma and has affected the mental well-being of nurses in many ways. We assume that hospital nurses might have experienced prolonged anxiety due to the pandemic. Therefore, we suggest that ‘prolonged anxiety’ could be a unifying concept used to describe nurses’ mental health problems, stress, and fatigue during and beyond the COVID-19 outbreak. This topic needs to be taken seriously, as it may have a particular impact on the attractiveness of healthcare careers and the successful recruitment of professionals in the future. Equally, hospital organizations must prepare for future pandemics by drawing up concrete plans to support nurses’ mental health and coping at work.
Footnotes
Author contribution
is the first author of this paper. Together with XX, XX, XX, XX and XX, she is responsible for the conception, study design and data collection. XX is a biostatistician, and he was responsible for data analysis together with XX. All authors were responsible for the critical revision of the manuscript.
Data availability
Data are not publicly available but may be accessed upon request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.