
Abstract
Various dementia training interventions have been developed for nursing staff, but there is inconclusive evidence on their effectiveness and which elements are key to positive outcomes. The aim of this study was to evaluate how nurses assess the prevalence of challenging behavior of people with dementia, nursing staff members’ responses to challenging behavior, and nurses’ competence, before the training and three and 12 months after the training. The main content of the training intervention was advancing person-centered care and its development. Data were collected through a survey of nursing staff (n = 127) at two Finnish nursing homes across three distinct time points. The TREND statement was used to enhance the quality and transparency of the research. The prevalence of challenging behavior in the experimental group significantly decreased one year after training, while no change was observed in the control group. No change in nursing staff members’ responses to challenging behavior was observed in either group over the study period. Nurses in the experimental group demonstrated significant improvements in self-assessed competence both three months and one year after the training intervention. Hence, regular nursing staff training can decrease the prevalence of challenging behavior among older people with dementia and enhance nurses’ competence in nursing. The support of supervisors plays a significant role in these changes.
Keywords
Introduction
It has been estimated that approximately 50 million people worldwide have dementia, with 10 million people developing dementia every year. 1 By 2050, the number of people with dementia in Europe is predicted to double; 2 as such, the number of people living with dementia in Finland is forecast to increase as the population ages.1,3 This is because the prevalence of dementia rapidly increases with age. 4 In Finland, about one-third of older residents in nursing homes have dementia. 3
Neuropsychiatric symptoms are common in dementia,5,6 and demonstrate nearly universal incidence across all stages and types of dementia. 7 These symptoms, such as agitation, depression, apathy, repetitive questioning, psychosis, aggression, sleep problems, and wandering, 8 are referred to as behavioral changes, or BPSD (behavioral and psychological symptoms in dementia). These symptoms can also be categorized under the umbrella term ‘challenging behavior’. 9 In nursing homes, more than 80% of older people with dementia experience at least one of the behaviors mentioned above.10,11 In this study, the term challenging behavior will be used to describe these neuropsychiatric symptoms. A generally accepted definition for challenging behavior is ‘an expression of distress in an individual with dementia or others in the environment, such as staff, arising from physical or psychological unmet need in the person with dementia’ (p. 43).12
According to Evripidou et al., 13 nursing staff lack the knowledge, communication skills, management strategies, and attitudes required to provide care that is favorable towards older people with dementia. Even though various training interventions have been developed, there is no general consensus on the key elements that sufficiently prepare nursing home staff for dementia care. 14 The adequate training of nursing staff continues to be an international issue of concern for the provision of high-quality dementia care. 15 For example, the World Health Organization 16 (WHO) highlights training as a crucial element of the 2017–2025 Global Action Plan for the public health response to dementia. The WHO 1 listed detecting and addressing challenging behavior as a primary goal, while Spector et al. 17 feel that the healthcare sector must work to minimize organizational barriers in the care of people with dementia. Both of these objectives require specific competencies, which can only be developed through training interventions that focus on nurses’ knowledge of, and practical experience with, challenging behavior among older patients. 18
Previous research19–23 that has applied the Cohen-Mansfield Agitation Inventory (CMAI) to the nursing home environment has found that neuropsychiatric symptoms, aggression, and challenging behavior all decrease after a staff training intervention. In contrast, it has also been reported24–27 that staff training interventions have no effect on the prevalence of challenging behavior. Psychosocial interventions, such as music therapy and cognitive behavioral therapy, have proven to be effective at reducing symptoms of depression or anxiety among older people with dementia. 28 According to previous studies,19,20 instructional, practical, and group-based training approaches that support the interaction skills of nursing staff, e.g. by focusing on person-centered thinking, including consistent recognition and maintenance of the person's autonomy, 29 can alleviate challenging behavior in dementia care.
However, Moniz-Cook et al. 30 previously stated that there is only weak evidence regarding which standard psychosocial approaches are the most effective at decreasing challenging behavior. They note that most studies on this topic have lacked the methodological rigor required to provide strong empirical evidence of the effectiveness of interventions. Differences in the duration, content, implementation, and measurable variables of previously described training interventions make it difficult to reliably assess which components of training interventions are effective. 31 Hence, little is currently known about the most effective approaches for designing, delivering and implementing dementia training. 32 This study aims to fill the existing knowledge gaps by evaluating how nurses assess the prevalence of challenging behavior of people with dementia, nursing staff members’ responses to challenging behavior, and nurses’ competence before the training and three and 12 months after the training.
Research questions
How do nurses assess the prevalence of challenging behavior of people with dementia three and 12 months after the provision of nursing staff training?
Are there any discernible changes in nursing staff members’ self-assessed responses to challenging behavior and self-assessed competence in caring for older people with dementia three and 12 months after the provision of training?
Methods
The present study applied a one-year follow-up quasi-experimental design in which one nursing home in Eastern Finland served as an experimental group and another nursing home in the same region served as a control group. Both nursing homes were specialized in dementia care. Nursing home staff in the experimental group (n = 66) received a face-to-face training intervention while nursing home staff in the control group (n = 61) carried out their work without any additional training. Data were collected from registered nurses and licensed practical nurses with vocational training (n = 127) using a structured questionnaire. More specifically, a paper questionnaire was used to collect data at the baseline time point, as well as three and 12 months after the completion of the training. The research was conducted between May 2018 and November 2019. The TREND statement 33 was used to enhance the quality and transparency of the research.
The questionnaire (Appendix A) designed for this study was based on a literature review of the subject and previous studies.34,35 The content validity of the questionnaire 36 was evaluated by a panel of four senior experts with experience in education as well as gerontological nursing and dementia care. The questionnaire demonstrated a content validity index score of 1, which is indicative of satisfactory content validity. A majority of the items (85%) were adapted from prior questionnaires34,35 that have been proven to be valid. The questionnaire contained 20 questions, distributed as follows: background information (seven items); prevalence of challenging behavior (one item) and forms of challenging behavior (one item); responses to challenging behavior (one item); competence (three items); suitability of facilities (one item); physical limitations (one item); leadership (one item); the impact of challenging behavior on coping at work (one item); and general nursing issues (three items).
Training intervention
The training intervention (Table 1) designed for this study by the first author is based on a previous literature review. 31 Nursing staff were asked about their training needs before the training; thus, they contributed to the content of the provided training. Nurses’ training needs were mainly related to concrete examples of policies in challenging situations, common work community practices and interaction skills.
Training outline.

Nursing staff in the experimental group participated in a 14-hour training intervention organized over seven separate days between August and November 2018. Each training session included different content and built on the previous session. The overall aim of the training intervention was to have nursing staff consider their own values as well as how the values of the work community affect the care provided to older people with dementia. The training was delivered by the first author, and the training sessions were delivered in the afternoon (from 1 pm to 3 pm) in the nursing home – a time when as many staff members as possible were able to participate. Each training session included a 15–20-min introduction to the topic, after which the educator presented activating and interactive ways of working. For example, the participants discussed certain issues together and performed tasks in small groups. The joint discussions and tasks were used to identify new operating models and competencies that are in line with the principle of individuality in caring for people with dementia. The nursing home supervisors also participated in each training session.
Data analysis
Descriptive statistics were used to analyze the data; all of the statistical analyses were performed in IBM SPSS Statistics for Windows (ver. 27; IBM Corporation, Armonk, NY). A two-way ANOVA was first performed to determine the statistical significance of the main effects (group, time) and interactions (group × time). If the two-way ANOVA revealed significant main effects or interactions, a pairwise comparison between the groups and measurement time points was conducted. The threshold for statistical significance was set at p < 0.05.
Ethical considerations
The study followed the principles of the Declaration of Helsinki 37 and Finnish National Board on Research Integrity TENK guidelines. 38 The local ethical committee provided approval for the study (104/2016). Furthermore, written informed consent was obtained from each of the study participants. The participants were made aware of the fact that participation in the study was voluntary and that they had a right to withdraw from the study at any point. The questionnaire was answered anonymously.
Results
The staff were given up to three weeks to complete and return the questionnaires, with response rates of 83% (n = 106), 74% (n = 94), and 73% (n = 93) for the questionnaires handed out at the baseline time point, three months after training, and one year after training, respectively.
Demographic characteristics of the respondents
At the baseline time point, the two groups did not significantly differ in age (p = 0.717), work experience at the unit (p = 0.355), work experience in dementia care (p = 0.799), education (p = 0.687), type of job contract (p = 0.140), or workplace (p = 0.108). The two groups significantly differed in gender (p = 0.044) at the baseline time point (Table 2). The two nursing homes provide care to 178 people over the age of 65 years, and the majority of these people have dementia.
Background characteristics at each measurement, presented as mean values (SD), n (%).

EG: experimental group; CG: control group; M: mean; SD: standard deviation.
Nurses’ assessment of the prevalence of challenging behavior
At the baseline time point (Table 3), the two nursing homes did not significantly differ in terms of the prevalence of residents’ challenging behavior. However, assessments by the nursing staff showed that the prevalence of challenging behavior decreased significantly (p = 0.005) three months after the training had finished. More specifically, half (n = 22, 51%) of the experimental group respondents reported that challenging behavior occurred daily, while the other half (n = 21, 49%) reported that it occurred weekly. No change in residents’ challenging behavior from the baseline time point to the threemonth follow-up time point was observed in the control group (p = 0.317), with four-fifths (n = 41, 80.4%) of the respondents reported that challenging behavior occurs daily,19.6% reported weekly prevalence.
The prevalence and impact of challenging behavior among older people with dementia in two nursing homes n (%).

EG: experimental group; CG: control group.
*According to baseline. #According to group.
In the experimental group, a statistically significant decrease in residents’ challenging behavior was also observed one year after the training had finished (p = 0.011), although the prevalence of challenging behavior had slightly increased from what was reported three months after the training had finished. No change in the prevalence of residents’ challenging behavior was observed in the control group (p = 0.872) one year after the training had finished.
Respondents also assessed how challenging behavior impacted their coping at work. For example, three months after the training had finished, nursing staff in the experimental group reported a statistically significant decrease (p = 0.034) in coping at work, i.e. challenging behavior affected coping at work less than it did at the baseline time point. No change in coping at work was reported by staff in the control group (p = 0.262). However, no significant differences in coping at work were observed for either group (experimental and control) between the baseline time point and one year after training (p = 0.132, p = 0.107).
Nurses’ responses to challenging behavior
No changes in nursing staff members’ responses to challenging behavior were discerned in either group across the studied time points (Table 4). Both before the training and one year after the training, nursing staff members were present during challenging situations and asked the affected older people what was wrong. Nursing staff in both the experimental and control groups were judged to have managed the situations well.
Nursing staff responses to challenging behavior, presented as mean values (SD).
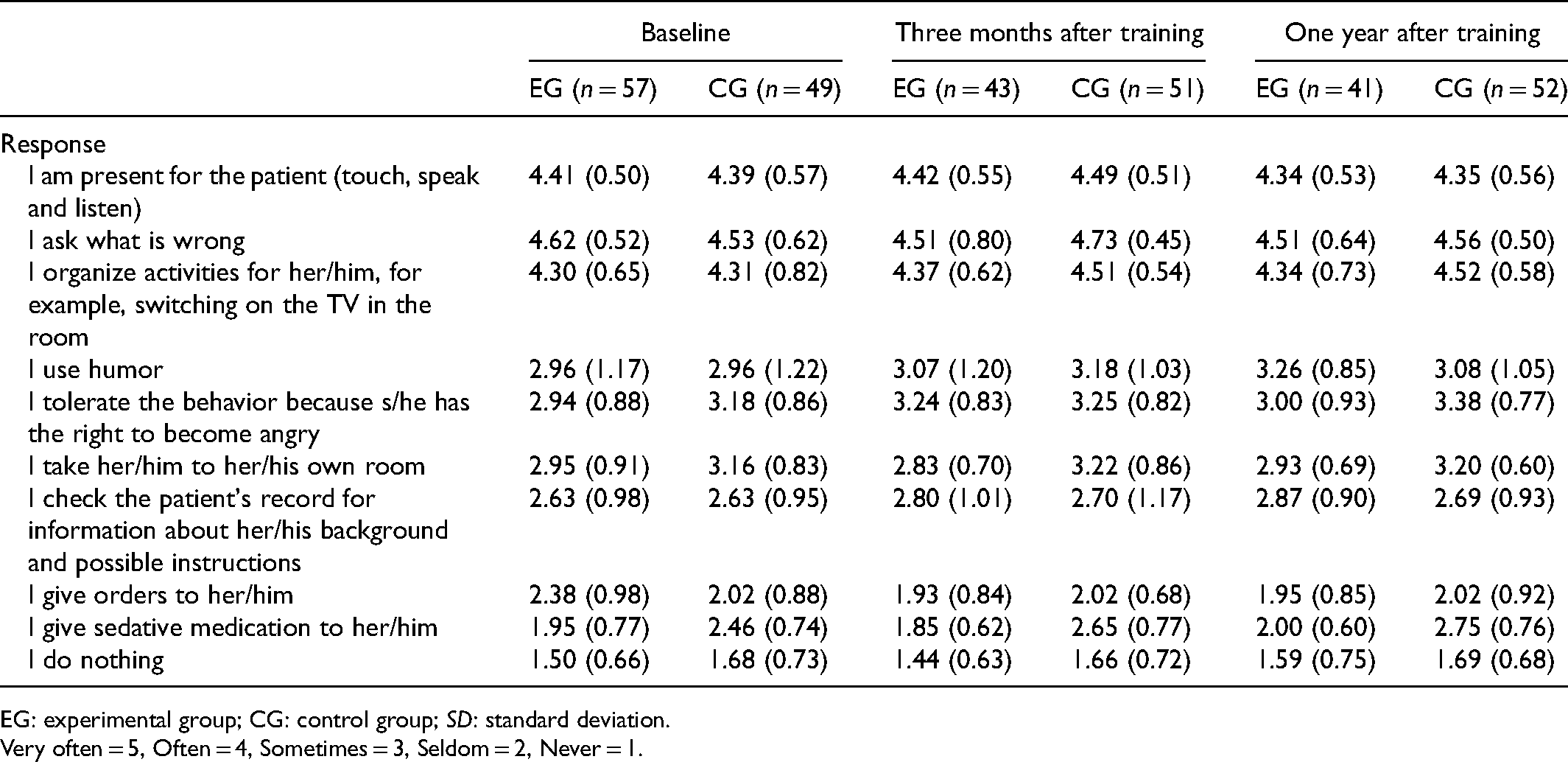
EG: experimental group; CG: control group; SD: standard deviation.
Very often = 5, Often = 4, Sometimes = 3, Seldom = 2, Never = 1.
Self-assessed competence among nursing staff
Respondents rated their current competence in dementia care on a scale of 1 to 10, with 1 signifying the lowest level of competence and 10 signifying the highest level of competence. In general, the nursing staff members’ self-assessed competence in caring for older people with dementia significantly improved (p = 0.013) in both groups during the study period. Based on measurements three months after the training had finished, no factor was found to significantly affect the participating nurses’ competence (p = 0.548); moreover, no significant between-group differences were observed (Table 5). The respondents also assessed the current competence in their work unit on a scale of 1 to 10 at each of the measurement points. At the baseline time point, a statistically significant (p = 0.019) difference was observed between groups, with the control group reporting significantly higher competence at their work unit than the experimental group (p = 0.049). In the experimental group, the respondents’ assessments of competence in their work unit significantly improved three months (p = 0.024) and one year after the training intervention (p = 0.023) relative to the baseline time point. No changes were observed in the control group.
Nurses’ self-assessments of competence in caring for older patients with dementia, presented as mean values (SD).

EG: experimental group; CG: control group; SD: standard deviation.
*According to baseline. #According to group.
Respondents were also asked about their competence in utilizing a person's life history when providing care. In the experimental group, nurses’ self-assessed competence in utilizing a person's life history when caring for people with dementia significantly improved three months (p = 0.001) and one year after the training intervention (p = 0.005). No changes in this specific competence were observed in the control group.
The respondents also assessed how leadership influences the implementation of person-centered dementia care. A statistically significant (p = 0.004) change was observed in the experimental group, i.e. respondents estimated that the leadership in their unit was more supportive of person-centered dementia care three months after the training intervention than at the start of the study. Furthermore, a statistically significant (p = 0.049) change in leadership was also observed between the three-month and one-year post-training time points, with respondents feeling that leadership had become less conducive to person-centered dementia care and returning to the levels that had been observed at the baseline time point. A statistically significant (p = 0.049) positive change in leadership was also observed in the control group, but only observed one year after the training intervention had finished.
Discussion
This study evaluated how nurses assess the prevalence of challenging behavior of people with dementia, nursing staff members’ responses to challenging behavior, and nurses’ competence, before the training and three and 12 months after the training. The planning and practical implementation of the training considered several factors that had previously been identified as conducive to dementia education by Surr et al., 15 namely, tailored to staff needs, face-to-face delivery, use of group-based activities and discussion, combining theory and knowledge, longer than one hour in duration, and delivered by an experienced facilitator. Nursing staff were asked about their training needs before the training; thus, they contributed to the content of the provided training. Smythe et al. 39 previously concluded that training should involve all staff members because it is an opportunity to demonstrate the value of the staff. Therefore, the studied training intervention was carried out in a nursing home where it was possible to involve the maximum number of nursing staff and their supervisors in the training. The training was attended by nurses currently on duty who were almost the same at each training session. However, there was some turnover in participants. There may have been turnover also among the residents of the nursing home during the study period, which may have undermined the reliability of the presented results.
Only non-pharmacological methods were discussed during the training, as these techniques are currently recommended for managing the challenging behavior of people with dementia. 40 However, psychotropic drugs are frequently used in long-term care facilities and are associated with the severity of neuropsychiatric symptoms, 41 and this may have undermined the reliability of the presented results.
The results of this study demonstrate that providing nursing staff with education that advances person-centered caring for older people with dementia can reduce the prevalence of residents’ challenging behavior at a nursing home, which corroborates previous findings.42,43 However, according to Surr et al., 32 the findings related to the impact of a training program on resident outcomes, i.e. behavior, are inconsistent due to methodological weaknesses in study designs and the lack of extensive follow-up periods in prior research. The results of this study demonstrated that a training program must be regular and continuous to have a significant and sustained impact on the daily routines of nurses. Clifford and Doody 44 also indicated that nursing staff working with older people with dementia should frequently engage in reflective practices, continuous education, and decision-making.
In this study, neither the experimental nor the control group showed a significant change in nursing staff members’ responses to challenging behavior over the studied time period. This may be explained by nursing staff already using empathic responses in challenging situations (i.e. the nurse is present and asks the person what is wrong) prior to the training. Based on these results, nurses in both the experimental and control groups were competent at employing an empathic response when caring for older people with dementia at the baseline time point. Watson and Hatcher 45 recommend nuanced education for the assessment and management of dementia to better address the unmet needs of older people with dementia, improve staff communication and attitudes, and develop collaboration among frontline staff. Furthermore, Gerolimatos et al. 46 suggest that a successful training program should involve staff members of varying professions in workshop development, assessment, and maintenance. In the present study, supervisors and nursing staff participated in each training session.
The results of this study indicate that the provision of relevant training can improve self-assessed competence among nursing staff working in dementia care. The challenge for further research is to combine the observation of the activities of nursing staff and the behavior of residents. In the present study, self-assessed competence at utilizing the life histories of older people with dementia during care improved among nurses in the experimental group both three months and one year after the completion of training, while no changes in this specific competence were observed in the control group. A prior systematic review identified knowledge as the outcome with the most significant improvement following training. 17 Moreover, Rokstad et al. 47 provided further evidence that a multicomponent training program can positively impact the development of person-centered care. The results of this study showed that a training program did not influence nursing staff members’ responses to challenging behavior; a finding which may be explained by nurses at both nursing homes already demonstrating appropriate responses prior to training.
Challenging behavior can increase nurses’ experience of stress and affect their ability to work. 48 The results of this study have provided empirical evidence that a training intervention can improve coping at work related to challenging behavior among older people with dementia. However, the effect noticed three months after the intervention was no longer discernible one year after the training. This supports previous claims that training should be regular and continuous if a sustained positive impact on nursing practices is desired. For example, Zwijsen et al. 49 stated that nursing staff require support in the management of behavioral problems, especially aggression and apathy.
It is difficult to identify which factors of the applied training led to the observed reduction in challenging behavior among older people with dementia, as challenging behavior is a complex phenomenon that is the product of biological, psychological and social factors. 50 Furthermore, the prevalence of challenging behavior can be dependent on nurses’ understanding of the situation and their experience of what is challenging behavior. However, it is clear that adequately training the nursing staff working in dementia care is relevant to the provision of high-quality, person-centered care on the international level and that further research on the subject is warranted. 32
Limitations
This study shows how training interventions for nurses working with older adults with dementia can affect the occurrence of challenging behavior at nursing homes, along with nurses’ self-assessed competence in caring for older people with dementia. The analyzed data were gathered through a questionnaire that had been validated by an expert panel, while the TREND statement 33 was used to enhance the quality and transparency of the research (see Appendix B). The study had some limitations; notably, the data were collected almost three years ago, sample size was rather small and the questionnaire was developed specifically for this study. This decision was made because no prior questionnaire was available for the study topic (combined questions concerning nursing staff members’ views of their competence as well as the competence of their work community). Although the questionnaire demonstrated strong content validity, construct validity was not assessed; this could have restricted the validity of the questionnaire.51,52 The potential for self-reporting bias should also be considered when interpreting the presented results. To improve the validity of the study, the researchers made sure to select two nursing homes of the same type and size for the study. Although both nursing homes are managed by the same entity, these two nursing homes may still differ in terms of individual practices, which could have affected the research findings. Thus, the presented findings should be generalized with caution. In this study, there may have been some response bias since the author who delivered the training also evaluated it. It is possible that respondents chose to respond positively to please the educator. However, the use of an experienced educator, in terms of nursing education, work experience, and pedagogical competence, increased the reliability of the training intervention. In addition, it should be noted that the intervention was designed in a way that promoted active participation by the nursing staff.
Conclusion
The prevalence of challenging behavior among older people with dementia can be reduced by offering nurses further training at regular intervals. Nurses can only be expected to develop and maintain their competence in providing person-centered care to older people with dementia through continuous education if they receive support from managers and supervisors.
Footnotes
Acknowledgements
Author contributions
Study design: PP, HMP, SE. Data collection: PP. Data analysis: PP. Drafting the manuscript: PP, HMP, SE. Manuscript development with critical intellectual content: PP, HMP, HS, SE. Manuscript final approval: PP, HMP, HS, SE.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Oulu Scholarship Fund.
Appendix A
Encountering a person with dementia in the nursing home
Questionnaire for nursing staff
Your service supervisor has given permission to carry out the survey in your work unit. The survey is personal and your participation is of paramount importance for the development of nursing. The information is confidential; they are not used for any other purpose or released for use by non-researchers.It takes about 15 minutes to complete the questionnaire.
The purpose of the study is to develop a model for training for nursing staff to meet a person with dementia. The aim is also to assess whether the model of training of nursing staff can influence the prevalence of challenging behaviour of people with dementia.
In the study, the second nursing home serves as an experimental group that participates in the training. The second nursing home serves as a control group in the study.
During the study, the questionnaire is filled in three times: before the training and after 3 months and 12 months of the training. You can suspend your participation in the study at any time without penalty.
We kindly ask you to return the completed questionnaire in a sealed envelope.
If you have any questions regarding the survey, you can call or email. Contact information is below.
Please answer the following questions either by choosing the option that best describes your situation or by writing your answers in the space provided.
From: Des Jarlais, D. C., Lyles, C., Crepaz, N., & the Trend Group (2004). Improving the reporting quality of nonrandomized evaluations of behavioral and public health interventions: The TREND statement. American Journal of Public Health, 94, 361-366. For more information, visit: http://www.cdc.gov/trendstatement/
Reported?
✓
Pg #
Title and Abstract
1
• Information on how units were allocated to interventions
✓
1
• Structured abstract recommended
✓
1
• Information on target population or study sample
✓
1
Background
2
• Scientific background and explanation of rationale
✓
2
• Theories used in designing behavioral interventions
✓
2
Participants
3
• Eligibility criteria for participants, including criteria at different levels in recruitment/sampling plan (e.g., cities, clinics, subjects)
✓
2-3
• Method of recruitment (e.g., referral, self-selection), including the sampling method if a systematic sampling plan was implemented
✓
2-3
• Recruitment setting
✓
2-3
• Settings and locations where the data were collected
✓
2-3
Interventions
4
• Details of the interventions intended for each study condition and how and when they were actually administered, specifically including:
○ Content: what was given?
✓
Table 1.
○ Delivery method: how was the content given?
✓
2-3
○ Unit of delivery: how were subjects grouped during delivery?
✓
2-3
○ Deliverer: who delivered the intervention?
✓
2-3
○ Setting: where was the intervention delivered?
✓
2-3
○ Exposure quantity and duration: how many sessions or episodes or events were intended to be delivered? How long were they intended to last?
✓
2-3
○ Time span: how long was it intended to take to deliver the intervention to each unit?
✓
2-3
○ Activities to increase compliance or adherence (e.g., incentives)
✓
2-3
Objectives
5
• Specific objectives and hypotheses
✓
3
Outcomes
6
• Clearly defined primary and secondary outcome measures
✓
3
• Methods used to collect data and any methods used to enhance the quality of measurements
✓
3
• Information on validated instruments such as psychometric and biometric properties
✓
3
Sample size
7
• How sample size was determined and, when applicable, explanation of any interim analyses and stopping rules
✓
4-5
Assignment method
8
• Unit of assignment (the unit being assigned to study condition, e.g., individual, group, community)
✓
4-5
• Method used to assign units to study conditions, including details of any restriction (e.g., blocking, stratification, minimization)
✓
N/A
• Inclusion of aspects employed to help minimize potential bias induced due to non-randomization (e.g., matching)
✓
5-6
Blinding (masking)
9
• Whether or not participants, those administering the interventions, and those assessing the outcomes were blinded to study condition assignment; if so, statement regarding how the blinding was accomplished and how it was assessed
✓
N/A
Unit of Analysis
10
• Description of the smallest unit that is being analysed to assess intervention effects (e.g., individual, group, or community)
✓
6
• If the unit of analysis differs from the unit of assignment, the analytical method used to account for this (e.g., adjusting the standard error estimates by the design effect or using multilevel analysis)
✓
N/A
Statistical methods
11
• Statistical methods used to compare study groups for primary methods outcome(s), including complex methods for correlated data
✓
4-5
• Statistical methods used for additional analyses, such as subgroup analyses and adjusted analysis
✓
N/A
• Methods for imputing missing data, if used
✓
N/A
• Statistical software or programs used
✓
3
Participant flow
12
• Flow of participants through each stage of the study: enrollment, assignment, allocation and intervention exposure, follow-up, analysis (a diagram is strongly recommended)
✓
3-4 Table 2.-5.
○ Enrollment: the numbers of participants screened for eligibility, found to be eligible or not eligible, declined to be enrolled, and enrolled in the study
✓
3-4
○ Assignment: the numbers of participants assigned to a study condition
✓
3-4
○ Allocation and intervention exposure: the number of participants assigned to each study condition and the number of participants who received each intervention
✓
Table 2.-5.
○ Follow-up: the number of participants who completed the follow-up or did not complete the follow-up (i.e., lost to follow-up), by study condition
✓
Table 2.-5.
○ Analysis: the number of participants included in or excluded from the main analysis, by study condition
✓
Table 2.-5.
• Description of protocol deviations from study as planned, along with reasons
✓
N/A
Recruitment
13
• Dates defining the periods of recruitment and follow-up
✓
1
Baseline data
14
• Baseline demographic and clinical characteristics of participants in each study condition
✓
Table 2.-5.
• Baseline characteristics for each study condition relevant to specific disease prevention research
✓
N/A
• Baseline comparisons of those lost to follow-up and those retained, overall and by study condition
✓
N/A
• Comparison between study population at baseline and target population of interest
✓
N/A
Baseline equivalence
15
• Data on study group equivalence at baseline and statistical methods used to control for baseline differences
✓
4-6
Numbers analyzed
16
• Number of participants (denominator) included in each analysis for each study condition, particularly when the denominators change for different outcomes; statement of the results in absolute numbers when feasible
✓
Table 2.-5.
• Indication of whether the analysis strategy was “intention to treat” or, if not, description of how non-compliers were treated in the analyses
✓
N/A
Outcomes and estimation
17
• For each primary and secondary outcome, a summary of results for each estimation study condition, and the estimated effect size and a confidence interval to indicate the precision
✓
Table 2.-5.
• Inclusion of null and negative findings
✓
6
• Inclusion of results from testing pre-specified causal pathways through which the intervention was intended to operate, if any
✓
N/A
Ancillary analyses
18
• Summary of other analyses performed, including subgroup or restricted analyses, indicating which are pre-specified or exploratory
✓
N/A
Adverse events
19
• Summary of all important adverse events or unintended effects in each study condition (including summary measures, effect size estimates, and confidence intervals)
✓
N/A
Interpretation
20
• Interpretation of the results, taking into account study hypotheses, sources of potential bias, imprecision of measures, multiplicative analyses, and other limitations or weaknesses of the study
✓
4-6
• Discussion of results taking into account the mechanism by which the intervention was intended to work (causal pathways) or alternative mechanisms or explanations
✓
4-6
• Discussion of the success of and barriers to implementing the intervention, fidelity of implementation
✓
4-6
• Discussion of research, programmatic, or policy implications
✓
4-6
Generalizability
21
• Generalizability (external validity) of the trial findings, taking into account the study population, the characteristics of the intervention, length of follow-up, incentives, compliance rates, specific sites/settings involved in the study, and other contextual issues
✓
6
Overall evidence
22
• General interpretation of the results in the context of current evidence and current theory
✓
6