
Abstract
Older people’s relatives’ negotiation power potentially influences their access to quality care and treatment after acute hospitalisation. This study aimed to analyse relatives’ purposes and strategies for negotiating with healthcare professionals (HCPs) after older people’s acute hospital admission. Eighteen relatives of older people who were discharged after acute hospital admission in Denmark were interviewed. Qualitative content analysis guided the analysis. We used COREQ as a reporting guideline. Three themes emerged from the analysis: (a) Braiding strings to make a cord, (b) Struggling for responsibility placement, and (c) A twofold agenda. The overall purpose for relatives’ negotiations with HCPs appeared to be a desire to ensure coherence in the older person's life. The strategy relatives used was negotiating the division of responsibility between relatives and HCPs. Relatives’ negotiations proceeded according to a twofold agenda. In the light of the ideas of French philosopher and sociologist Pierre Bourdieu, we conclude that relatives’ negotiation strategies can be understood as a result of their habitus, their social position, and the capital they bring to the specific situation.
Background
Every year, 245,000 older people are hospitalised in Denmark. 1 A large number of older people (aged 80 years or older) are hospitalised more than once and the number of older people who are acutely hospitalised is increasing in regard to both short and longer admissions.2,3 When older people are discharged after an acute admission, they may be vulnerable and experience challenges navigating the healthcare system and negotiating their care and treatment.4,5 Potentially, these older people are dependent on help and support from their relatives if they want to navigate the system successfully.6,7 Therefore, they often involve the support of their relatives.8,9
Quality of care and treatment appears to improve if older people have active, resourceful relatives, compared to that of older people who do not have relatives advocating and negotiating on their behalf. 10 Studies indicate that the involvement of relatives reduces older people’s frustrations and can make their hospital stay and the discharge process less stressful.11–15 Relatives can play an important role as spokespersons in older people's health and care planning meetings before hospital discharge. 16 Furthermore, older people’s relatives can provide advocacy and create a safety net by influencing healthcare management and safety after the discharge of older persons. 17 Some relatives provide practical support and take on the role of advocates or mediators when trying to negotiate care and treatment on behalf of the older person and ensure its quality and dignity. Other relatives act more passively and hesitantly.18–20
Overall, this means that some relatives of older people who are discharged after an acute admission can feel vulnerable and troubled by, for example, the high level of responsibility they carry, and exhibit anxiety and depressive symptoms.21–27
In a previous study, we found that some relatives have strong negotiation power whereas other relatives are less powerful when it comes to negotiations with healthcare professionals (HCPs) concerning older people’s acute admissions. 20 This difference between relatives with strong negotiation power and those who are less powerful can potentially complicate older people's possibilities to gain access to quality care and treatment after acute hospitalisation, and thus can cause inequality in health.
However, knowledge about relatives’ negotiations with HCPs after older people are discharged from an acute admission remains scarce. In this study, the concept of ‘negotiation’ was understood as a social process included in all aspects of life since it is a kind of decision-making related to situations marked by conflicting interests.20,28,29
Aim
The aim of this study was to analyse relatives’ purposes and strategies for negotiating with HCPs after older people’s acute hospital admission.
Methods
Research design
We used the Consolidated Criteria for Reporting qualitative Studies (COREQ) as a reporting guide. 30 Building on a hermeneutic approach, we chose a qualitative design using semi-structured interviews with relatives of older people who had recently been discharged from the hospital after an acute admission.31–33 The focus of the interviews was relatives’ experiences in their role and negotiations with HCPs during the discharge process and the older person's further care pathway.
Setting and participants
We invited relatives of older people acutely admitted to one of two emergency departments (EDs) at a Danish regional hospital to participate. In these EDs, patients are acutely admitted and treated for different somatic diseases and stay less than 48 hours. Those who are not ready for discharge after 48 hours are transferred to a hospital ward, from which they are later discharged. We used purposeful sampling to include participants meeting the following eligibility criteria: relatives of patients aged 75 years or older acutely admitted to one of two EDs between September 2018 and April 2019.20,34 We aimed to include participants of different ages and genders, and with different types of relations with the older person in acknowledgment of modern family structures; thus, relatives encompassed family members and other significant persons as defined by the older person. Participants who did not speak or understand Danish sufficiently to participate in an interview were excluded. Eleven participants were recruited from among the participants of two previous studies on relatives of older acutely admitted patients based on the same inclusion and exclusion criteria as in the present study. The two previous studies used interviews and observations and the same sampling method as the current study.20,35 After participating in the previous studies, the participants were asked whether the researcher could contact them within 2 weeks of the older person's discharge from the hospital to ask whether they would participate in a follow-up interview. If the participants agreed to this, the researcher contacted them to provide further information, collect written consent, and make appointments for interviews. Seven further participants were recruited at the EDs following the described process.
Data collection
Data were generated through individual semi-structured interviews. 36 An interview guide was inspired by recent qualitative empirical studies on relatives’ experiences related to older peoples’ discharge from the hospital18,19,27,37 as well as theoretically based assumptions on client competencies 38 (Box 1).
Examples of questions included in the interview guide
Please tell me about the discharge process and the time right after discharge.
Who was involved in the discharge process?
How did you experience the coherence of care and treatment at the hospital and the care and treatment X received after discharge?
How did you experience your role in the discharge process?
Tell me about how X was transported home from the hospital.
How has your everyday life been affected since X's discharge from the hospital?
The focus for answering these questions was as follows:
What did you do? How did you do it? If possible, tell us why you did it. Probing questions were used.
The first author, who is trained in qualitative interviewing, conducted all the interviews. The participants were asked where and when they would prefer the interview to be conducted. A logbook was used for the interviewer’s immediate reflections after each interview. The interviews were recorded, and the first author transcribed all the interviews verbatim.
Data analysis
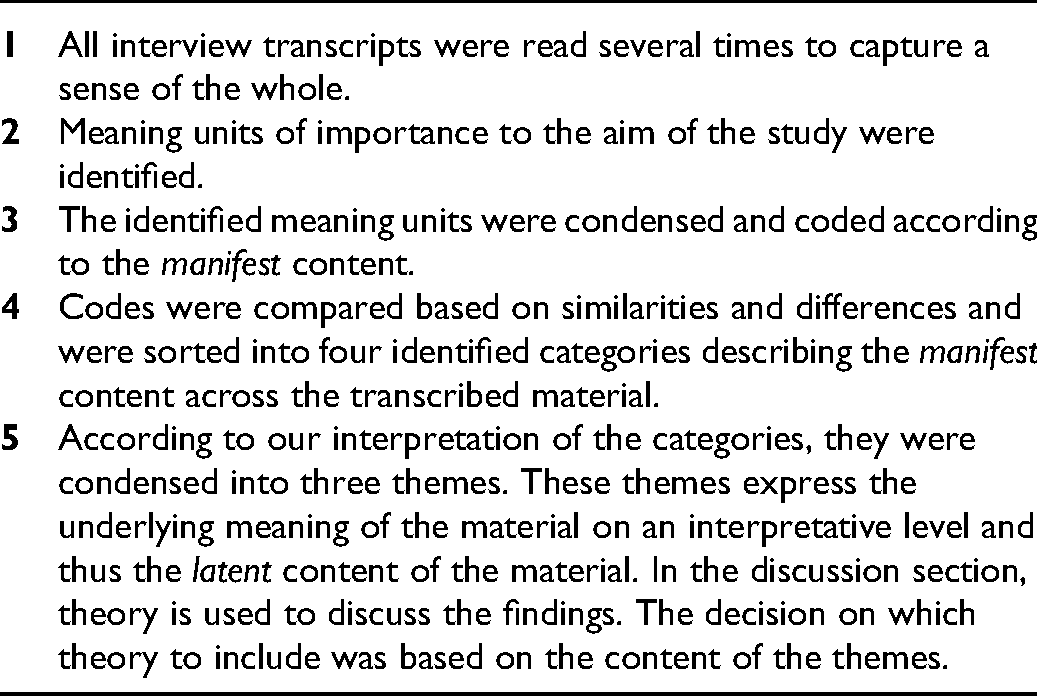
To be able to describe the manifest as well as interpret the latent content of the empirical material, we used qualitative, inductive content analysis. 39 The process to achieve understanding uses a hermeneutic spiral encompassing the researchers’ preunderstandings, the context and interpretation of meaning of the text in a process moving back and forth between the parts and the whole.33,39 The various steps in the inductive analysis process are described in Table 1.20,35
The software program NVivo supported the analysis. Although the analysis process is described as linear, the process included iterations working forward and backward between the parts and the whole. An example of the analysis process is presented in Table 2.
Examples of the analysis process.

*A metaphor describing relatives’ attempt to ensure coherence.
HCP: healthcare professional.
Ethical considerations
All participants signed a written informed consent form before participation. 40 To ensure confidentiality, no names or other personal sensitive information are shown in the findings section. The local regional ethical committee was informed about the study but decided that formal approval was not required (Ref. ID 20182000-88). Storage and management of data were registered under the Danish Data Protection Agency (Journal number 18/33143). Data were stored and analysed in OPEN Analyse, a safe environment that complies with the European General Data Protection Regulation and Danish law for data protection. 41
Findings
A total of 20 relatives accepted the invitation to participate. As described, 11 of these were recruited from among participants of two previous studies. Two relatives who agreed to be included in the study later cancelled their appointments. One could not find time for an interview because of a heavy workload; another cancelled because the older person's situation became critical. All participants were family members. The interviews were conducted 2–4 weeks after the older people's discharge from one of the two Danish EDs. The interviews lasted from 24 minutes to 1 hour and 17 minutes.
Characteristics of the participants.

Three of the interviews were conducted by telephone because the participants preferred this. Face-to-face interviews were conducted in a place chosen by the individual relative. Some were conducted in the relative's own home, some in a quiet room at the hospital and one interview was conducted in the interviewer's home for practical reasons. Three of the interviews included two participants (a sister and a brother, a daughter and a son-in-law, and two sisters, respectively). The remaining 12 interviews were conducted with one relative. The older person was not present during the interviews. Thus, in total, 15 interviews were conducted with 18 participants who were relatives of 15 older people who had been acutely admitted (Table 3).
Three themes were derived from the analysis: (a) Braiding strings to make a cord, (b) Struggling for responsibility placement, and (c) A twofold agenda. These themes are presented in the following section and illustrated by selected quotations from the interviews.
Braiding strings to make a cord
The acute hospital admission was a break in the coherence of everyday life, and some participants tried very actively to re-establish some sense of coherence after the discharge by negotiating with the HCPs. One relative expressed his struggle to make ends meet in his father's care pathway by using the metaphor of braiding strings to make a cord. We [relatives in general] are supposed to braid a string of the strings we get [shows some moves with his arms and hands visualizing that he is braiding a cord]. (Hector, son, 49 years old)
After the acute admission, adjusted services from the municipality, medicine, disability aids, or outpatient appointments had to be implemented in the older person's everyday life. In most situations, the older person's care pathway included contact with both the hospital and HCPs outside the hospital, which could make navigating the healthcare system complicated for the older person as well as for the relatives. Relatives also experienced unsatisfying care and service from the HCPs. These experiences contributed negatively to the relatives’ experience of security and led to distrust in the system and motivated some relatives to negotiate with the HCPs.
How the relatives tried to ensure coherence also seemed to be individually determined, and they played different roles in this process depending on the older person's health condition, the older person's mental and physical condition, the relatives’ mandate from the older person, and the discharge process. Some participants acted passively and hesitantly, whereas others were very active trying to negotiate and create a sense of coherence in the older person's care pathway.
Participants who actively aimed to ensure coherence in the older person's life contributed different kinds of help and support. Some participants helped the older person with practical tasks, such as cooking and cleaning. Other participants (also) helped with organisational tasks such as remembering appointments, calling the general practitioner, and negotiating with the municipality for additional services.
Some participants tried to be at the forefront to detect even the smallest coherence breaks in the older person’s life. When detecting these coherence breaks in the older person's life, some participants acted proactively. They considered themselves to be contributing positively to the quality and safety of the older person's care and treatment by trying to solve the problem themselves or by trying to involve the HCPs. They considered it necessary to keep an eye on the HCPs and act as the older person's safety net: It is because in her care plan there was often a message – ‘Everything fine’ and ‘X [patient's name] is well’. And I thought, ‘Why the hell do you [healthcare professionals from the local municipality] write that? I mean why do you write the same thing every day and yet when I visit – I can certainly see that she is not all right’. (Hannah, daughter, 56 years)
Experiences from former hospital admissions, the current admission, or other contacts with the healthcare system seemed to affect how alert the participants were to detecting lack of quality in care and treatment and how eagerly they negotiated with the HCPs. Some had lost trust in the HCPs and the healthcare system along the way: They [staff at the nursing home] are not competent. They can’t spot someone who's sick, they can’t write a journal note, they can’t communicate across sectors, there is no communication between the first and second shift, and when they don’t even read [in the healthcare reports], they have no idea what is happening. And even the most basic things they are unable to carry out. Yes, the most absolute basic things. Shit under fingernails and greasy hair and yet when you go in and look, they have checked off that she has been showered. So it's at this level, it's easier to check off and document that you’ve done something without actually having done it. (Alex, son-in-law, 65 years old)
Some participants considered themselves to be a sort of ‘glue’ ensuring that the older person's health and everyday life did not fall apart, and that the older person's life did not become unworthy. This experience of lack of trust in the HCPs and the healthcare system linked to the participants’ feeling of responsibility. Relatives experienced these loose ends in the older person's life in different ways and considerations about the older persons’ situation appeared to be related to the relatives’ expectations of themselves and their own resources and their expectations of the HCPs. This encouraged some relatives but not others to try to ‘braid strings to make a cord’.
Struggling for responsibility placement
The participants had very different perspectives on their responsibility for the older person. Some considered it to be their main responsibility to help and support the older person. Others felt they had to take this kind of responsibility because they considered the professionals failed: Yeah, it's becoming more and more [that as a relative they need to help with practical things] because they do less and less [voice becomes higher and more strained]. Yeah, and we have extra cleaning help once a month because they don’t do it. (Emma, daughter, 55 years old)
Some participants played a vital role in the older person's discharge process and their everyday life after the discharge. A daughter-in-law (with a health-related background) told how she and her daughter (who was a nurse) had influenced the older person's pain therapy positively: Our daughter is also a nurse, and she said ‘Why not just use pain relief patches?’ It was because they couldn’t get her to swallow tablets. She just spat them out. (Diana, daughter-in-law, 58 years old)
Some participants accepted that the HCPs controlled the older person's care pathway whereas others negotiated to gain more influence in the older person's care and treatment and to make the HCPs involve them in decisions. They explained that they felt responsible.
Thus, some negotiations between the HCPs and the participants concerned the distribution of responsibility among the two parties. The participants’ narratives about the discharge and their role in the older person's everyday life after the hospital admission showed that they had different experiences of their own and the HCPs’ roles in the older person's care pathway.
The participants told of experiences of unsatisfying care and poor-quality service (e.g. in cleaning the older person's home), failures (e.g. the HCPs forgetting to do things they were supposed to take care of), or unempathetic or undignified care (e.g. not talking properly to the older person or not taking time to listen or to recognise the older person's well-being). In some situations, the participants described themselves and the older person as victims or as heroes who were defending the older person's dignity and reacted if they found the quality of care to be poor: So each time I threaten them with calling the municipality [when the care is inadequate]. You know that they can’t be so stupid that they don’t notice that he's wet the bed. They just shake the pillow and put the duvet over it. (Béatrice, sister, 70 years old)
Some participants defended or protected the older person, whereas others actively tried to take responsibility and improve the quality of care on a general level: Also, I think that is what I wrote [in a complaint to the municipality]. We can see the difference between the good and the bad and we just want to lift the level of the bad carers to the level of the good carers. (Alex, son-in-law, 65 years old)
Some participants negotiated strategically and were aware of the strategies they used to be in successful contact with the HCPs and make them listen to their messages, whereas others did not. Some participants negotiated with the HCPs in a confronting way, whereas others negotiated more diplomatically.
The participants negotiated at different organisational levels. Some negotiated only with the frontline staff, whereas other participants negotiated on the management or political level. Some relatives addressed their dissatisfaction with the quality of care and treatment to named HCPs, whereas other participants expressed their dissatisfaction on a more general level and, for example, blamed ‘the system’.
A twofold agenda
The older person's acute hospital admission appeared to be an extraordinary experience for all the participants. The acute admission represented a state of emergency that activated a kind of ‘all hands-on deck’ attitude among the participants. They put their lives on hold during the acute admission and focused primarily on the well-being of the older person. When the older person was discharged from the hospital and returned to their everyday life, a new era started and the participants gradually became aware of their own needs and desires, and occasionally the desires and needs among other relatives. This meant that after the discharge, some of the participants were negotiating not only the older person's agenda but also their own. Some were aware of this twofold agenda and expressed their concerns, needs, and wishes in the interviews: I was there for about three-quarters of an hour, and I met my sister out in the parking lot. I said, ‘Oh my god, I have a bad conscience. All I want to do is cry’. My parents’ house was a mess. I could have cleaned up but then no one would know how bad it actually was. Yes, we need to [order private cleaning services] because I can’t stand this anymore. I am simply too exhausted to go there and clean the bathroom and all that. (Fiona, daughter, 57 years old)
In other situations, the participants seemed to act altruistically or expressed their own needs and wishes more implicitly.
And occasionally, I think, ‘Well, if they won’t take care of him [the older person], I will’. I reckon the carers also think, ‘She is moaning a lot’. I would rather that they didn’t think that. But occasionally [rolls her eyes] I count to 10 and I think, ‘I could just do it myself as long as my brother is happy’. (Béatrice, sister, 70 years old)
Some participants were aware that they needed to negotiate with the HCPs to be able to defend their own needs, health, and quality of life and to be able to carry on as relatives in the longer term.
Discussion
This study aimed to analyse relatives’ purposes and strategies for negotiating with HCPs after older people’s acute hospital admission. Loose ends appear to be a common element of relatives’ experience of older persons’ acute hospitalisation. Lack of continuity, coordination, and quality of care appears to be related to both the organisation of the healthcare system and the HCPs. To experience these loose ends makes relatives more alert to HCPs’ actions. Furthermore, it appears to negatively affect relatives’ trust in the healthcare system and the HCPs when relatives experience a lack of quality. It encourages them to take the role of ‘watchdogs’ and inspectors and to negotiate with the HCPs. Findings from another Danish qualitative study confirms that relatives who do not trust HCPs watch and check the HCPs to ensure they perform their job adequately. 42
Moreover, our findings indicate that relatives seem to be troubled and overwhelmed when they experience having the overall responsibility for the older person's situation after the acute admission and thus some relatives try to negotiate the distribution of responsibility with the HCPs. Other studies have also found that being alert is a very stressful and frustrating state of mind, and relatives experiencing this potentially seem to find this challenging physically, socially and mentally.24,43
Some relatives seem to respond to the lack of quality and coherence in older people’s care pathways by trying to make loose ends meet and to re-establish coherence, safety, and dignity in the older person's life. Other relatives seem to act more passively and hesitantly. Bendix Andersen found that relatives can be ‘significant actors’ who make it possible for patients’ care pathways to progress as intended. 44 Similar studies confirm that relatives take on different roles of mediators, intermediaries, and advocates to ensure quality and continuity in older people's lives after discharge from acute hospitalisation.10,18,23
According to the French philosopher and sociologist Pierre Bourdieu (1930–2002), human strategies are related to a person's habitus, position in the field and capital.45,46 People’s strategies are based on individual dispositions, which means that relatives’ strategies are a result of (a) their habitus (their predispositions acquired through earlier experiences, e.g. their upbringing), (b) their position in the field (their social position as a relative to an older person in the Danish healthcare system) and (c) their capital (their assets in the forms of economic, cultural, social and symbolic capital). According to Bourdieu, people will always act strategically to optimise their situation. 45 Thus, to act strategically, according to Bourdieu, is not a rational trade-off between pros and cons. 45 This selected part of Bourdieu's theory of practice can help explain why some relatives actively try to negotiate the distribution of responsibility whereas others do not, and why relatives who negotiate use different strategies when negotiating the distribution of responsibility.
Human strategies are influenced both by external structures (e.g. laws, policies, organisational structures, etc.) and subjective experiences (e.g. relatives’ experience of the world). 46 This means e.g. that if and how relatives negotiate the distribution of responsibility, will be influenced by the actual discourses about relatives within the present political vision of involvement of relatives in the Danish healthcare system. 47 Stie et al. analysed eight policy papers by Danish healthcare authorities, institutions and patient interest groups published from 2014 to 2018. 47 Their study revealed three discourses about relatives: 1) the rational relative, 2) the responsible yet subordinated relative, and 3) playing the role of a resourceful relative. Stie et al. argue that these discourses affect how HCPs meet relatives and how relatives are positioned. 47 According to Stie et al., the discourse describing relatives as rational and responsible but in the ‘second row’, is the most prominent. This means that HCPs primarily consider relatives to be resourceful but secondary to the patient. If HCPs primarily consider relatives as resourceful it can cause a lack of concern for their well-being and the relatives’ potential own need for care and information. 47 This can potentially make it more difficult for relatives, who feel overburdened to stand up for their own needs and wishes and negotiate these needs and wishes with the HCPs. Our findings indicate that when relatives negotiate with HCPs after the older person's discharge from the hospital, their negotiations seem to be based on a twofold agenda including both the older person's needs and wishes and the relative's own needs. The dominant understanding of relatives as resourceful may explain why some relatives unconsciously cover their own needs by mixing them with the needs and wishes of the older person in a twofold agenda. Relatives who feel overwhelmed by a heavy responsibility may find it difficult to put their feelings into words and negotiate the distribution of responsibility between themselves and the HCPs because it could be experienced as a defeat and as a sign of inadequacy by the HCPs and the healthcare system in general.
In this study, some of the participants’ narratives seem to refer to the older person, and occasionally themselves, as victims of the HCPs’ mistakes and of HCPs not meeting their expectations and taking sufficient responsibility. Others seem to refer to themselves as heroes defending the older person against the HCPs’ failures and criticisable care. This analogy of victims and heroes may reflect the different ways relatives position themselves to the HCPs.
Drawing on Bourdieu's concept of strategy, Guldager et al. identified three positions among relatives: the warrior, the observer and the hesitant. 48 These positions illustrate how relatives position themselves in different ways and how their dispositions influence their strategies. 48 According to Guldager et al., the three positions differ in their need for support during a rehabilitation process. 48 These differences may refer to Bourdieu's perspective on human strategies as being conditioned by habitus, position in the field and capitals. 49 Relatives’ strategies will be a result of the possibilities they have for affecting and controlling the situation and their expectations for how they will accommodate their own needs and wishes and their expectations for what is possible in the specific situation. The division of relatives into ‘active’ and ‘passive’ groups is well known from other studies.48,50
Methodological strengths and limitations
To improve the reliability and validity of the study, we aimed to present the analytical process as transparently as possible. 31 We consider that individual, qualitative interviews proved to be a suitable method to answer the aim of the study through rich and nuanced data. 36 Eleven of the 18 participants also participated in two previous studies on the role of relatives in relation to older peoples’ acute admissions.20,35 The established confidentiality and relation with these 11 participants affected the quality of data positively and contributed to rich data. We used the concept of information power to reflect on and guide the sample size. 51 The number of participants seemed suitable to answer the aim of the study in a qualified way. Two relatives accepted to be included in the study but later cancelled our appointment. This also means that the relatives who were included in the study may be more resourceful than other relatives. The gender imbalance among the participants is not addressed since we did not explicitly focus on gender-specific issues. Since gender may have influenced relatives’ aim and strategies for negotiation, this may be considered a limitation of the study. The analysis and interpretation of the empirical material were based on reflections and discussions between the authors throughout the process. These ongoing reflections and discussions strengthened the validity of the findings. 31 The findings from this study are nuanced and reflect different kinds of relatives’ experiences, and are suitable to be transferred and used in other contexts.
Conclusion
This study aimed to analyse relatives’ purposes and strategies for negotiating with HCPs after older people’s acute hospital admissions. Based on our findings we can conclude that the overall purpose of relatives’ negotiations was to ensure coherence in the older peoples’ lives. The relatives negotiated the division of responsibility between relatives and HCPs and proceeded on the basis of a twofold agenda (the older person’s and the relative's agenda). In the light of the ideas of French philosopher and sociologist Pierre Bourdieu, we conclude that relatives’ negotiation strategies can be understood as a result of their habitus, their social position and the capital they bring to the specific situation.
Implications for practice and suggestions for future practice
To gain trust from the relatives, HCPs have to minimise the number of loose ends in the older persons’ care pathways by delivering high-level care, treatment, and services to the older person.
Furthermore, HCPs need to facilitate a transparent distribution of responsibility between the HCPs and relatives after an older person's discharge from the hospital. A transparent alignment of expectations is important on both a political and organisational level as well as a practical and individual level for relatives to feel trust in the healthcare system and the HCPs.
Our findings underline the importance of paying attention to relatives’ reactions, needs, and preferences and supporting the relatives not as an appendix to the older person but as independent individuals with their own needs, wishes, and challenges. Furthermore, our findings underline the importance of HCPs acknowledging relatives’ twofold agenda to negotiate both the older person's well-being and their own. In future research, it would be relevant to include older people's relatives as co-designers in, for example, action research studies to develop cooperation opportunities and strategies to ensure quality, continuity, and coordination of care when older people are discharged after acute hospital admission.52,53 Findings from this study could guide this kind of action research.
Footnotes
Acknowledgements
The authors would like to thank the relatives who spent their precious time participating in the interviews and making this study possible.
Ethical approval
According to the current Danish legislation, the study did not need formal ethical approval from the Regional Scientific Ethical Committee. Storage and management of data are registered with the Danish Data Protection Agency. The study complied with the Helsinki Declaration and the Ethical Guidelines for Nursing Research in the Nordic Countries.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Region of Southern Denmark, Hospital Sønderjylland, University Hospital of Southern Denmark, University College South Denmark.
Conflict of interest
The authors declare that there is no conflict of interest.