
Abstract
With the growing demand for primary care, provision needs to be efficient, yet retain person-centred and integrated care. Digital communication is suggested as a way to settle these aspects, although there is insufficient knowledge regarding the end-user's perspective. The aim of this study was to describe patients’ experiences of digital communication in their primary care contact, while considering aspects of person-centred care. A purposeful sample of 16 patients (aged 28–85 years) was interviewed via telephone in a qualitative design, and verbatim transcripts were analysed using inductive thematic analysis and a subsequent deductive approach in relation to a person-centred care framework. The study was reported following the COREQ guidelines. The findings indicate that, from a patient perspective, digital communication enables independent contact where one crafts one's medical history at a time and place convenient for oneself, providing opportunities for the primary care triage to consider one's individual input. These aspects of digital communication serve person-centredness, although they were less suitable for certain health issues, but a human interaction was most appropriate when health concerns were ambiguous or complex. Thus, digital communication may serve patients in primary care, but the development and implementation of such services must move beyond technical and professional perspectives. In order to facilitate integrated care, further emphasis is needed on both patients’ experiences, and the principles of person-centred care.
Introduction
New digital innovations and e-health have been proposed to meet many of the challenges of contemporary primary care.1,2 The introduction of digital communication tools (that is, online communication and/or the exchange of information using digital means) can benefit the individual patient, that is, the end-user, for example by reducing geographical barriers and increasing access to healthcare. 3 Furthermore, digital services like health apps and web-based intervention programmes can aid individuals in activities such as chronic disease management, 4 putting the individual in control of his or her healthcare and expanding their opportunities for self-care management.5,6 Nonetheless, the digitalisation of healthcare runs the risk of producing services that focus on organisations rather than end-users such as patients.7,8 To provide sufficiently integrated person-centred care, a deeper understanding of patients’ experiences of digital communication is needed.9–11
Studies on digital health services in primary care often focus on staff experiences.12–16 In general, digital innovations are favoured by end-users if they are easy to use and have clear instructions, and where patients themselves can decide if and when to use them.6,17,18 However, a sense of mistrust can develop if the implementation of digital tools suggests a reduction in healthcare resources, 17 or if they replace face-to-face meetings. 18 In addition, patients’ technological self-confidence and know-how can influence their ability to employ and benefit from digital healthcare communication services. 18
Both patients and healthcare professionals are aware of and concerned about the risk that new digital innovations may negatively affect interpersonal relations.18–20 Thus, the current progress in person-centred care needs to be reinforced by digital communication processes in such a way that the provision of such services aligns with patient preferences and a holistic approach to patient needs and experiences. 21
Person-centred care does not have a universally accepted definition.22,23 Yet, a common framework suggests that person-centred nursing is promoted by the professional (that is, the registered nurse), the context in which care is delivered, and the processes focusing on the delivery of care in a person-centred mode, 24 facilitating person-centred outcomes. The prerequisites for person-centred care are nurses who are professionally competent, with interpersonal skills and commitment to their jobs, who have clarity of values, and know themselves. Contexts facilitating person-centred care are recognisable by: an appropriate skill-mix; strategies for shared decision-making; working relations among staff, including the sharing of power; and supportive organisational systems, with opportunities for innovation and thus a certain level of risk-taking while recognising the need to perform nursing in accordance with evidence and best practice.
Person-centred interventions often emphasise extended and/or recurring healthcare contacts.25–28 Primary care typically represents such interactions, suggesting that person-centred care can be established. However, there are demands for a more efficient use of resources in primary care, and this is increasingly addressed by means of digital communication. Such innovations may suffice to provide both efficient and person-centred primary care,29,30 in situations where they recognise the individual's needs and resources. To date, very little is known about patients’ experiences of digital communication,31,32 although these perspectives on its functionality in relation to person-centred, integrated primary care are indispensable prior to a more extensive implementation. 33 The aim of this study was to describe patients’ experiences of digital communication in their primary care contact, while considering aspects of person-centred care.
Methods
This qualitative study comprised semi-structured telephone interviews which were transcribed verbatim and analysed abductively, that is, initially by means of inductive thematic analysis 34 and subsequently by employing a person-centred care framework to develop the understanding of patient perspectives.35,36 The study was reported following the COREQ guidelines.
Setting
The study was performed in a healthcare region in southeast Sweden, where five primary care centres had agreed to take part in a pilot test of a commercial digital communication system. This included both smaller and larger centres in urban and rural areas. While an independent team of researchers was appointed to appraise all end-users’ experiences of the system, including those of healthcare staff, managers, and patients, this article represents the primary patient interviews. During the test (launched in April 2019), patients were offered the digital communication system as an alternative to their regular contact with primary care. Information about the availability of this alternative was advertised on the general healthcare website and as an automatic voice message on the phone service of the primary care centres . Normally, to sign up for a primary care appointment, a patient would have to phone early in the morning and agree to being called by a triage nurse later in the day. For the test period, a voice message offered the digital communication service as an option for the further primary care contact. Another route to making patients aware of the digital communication alternative was through posters displayed in the waiting rooms of the primary care centres. Patients received no further guidance about how to use the new digital communication system prior to entering the service.
The system was designed to aid in the construction of a medical history and appointment, to support the assessment and triage conducted by the primary care centre. Patients entered the system by identifying themselves via their electronic ID. Once signed in, they were provided with standardised, tree-structured templates, as a response to the primary reason for contact stated by the patient. These templates included a set of multiple-choice and open-ended questions. In addition, the system included self-assessment scales, linked to previous responses.
When the patient had concluded a registration, the information was presented as a medical history to the primary care centre. This was assessed in a triage process by a registered nurse (RN) within two hours (during office hours, approximately 08.00–16.00, Monday to Friday). The RN's response to the patient was also digital, suggesting self-care, referral, or a medical appointment. If further information was needed at this point, the nurse would reply within the digital communication system by initiating an online, asynchronous chat with the patient, 37 during which the RN had a two-hour limit for the response, while the patient was expected to reply within a three-day limit. It was anticipated that patients would report information about themselves in the digital communication system, but it could also be used by parents for paediatric enquiries.
Recruitment of study participants
For this study, during the first six weeks of the pilot period, a query appeared in the digital communication system asking all patients who used the service (n = 572) at the five pilot primary care centres whether they would agree (or not) to take part in a study regarding the digital communication. A total of 183 individuals agreed. A strategic selection of 30 patients was made, based on diversity of gender, age, and primary care centre at which they were registered. These 30 individuals were contacted by phone, given further information about this study, and asked again if they wanted to participate. If they still agreed, written information was emailed and a date and time for the interview was set up. Inclusion was based on ‘being a patient who had used the digital communication system to contact the health centre’, and the single exclusion criterion was a non-health-related reason for contact (that is, an administrative issue which did not comprise full use of the system, and/or triage by an RN). A total of 16 individuals matched the criteria and provided written informed consent to take part in the study.
Data collection
An interview guide was constructed by the research team for this project. It consisted of open-ended questions designed to stimulate a narrative, 38 with follow-up probes; the probes were only used if a patient did not spontaneously expand their response. The issues embraced were the patient's experiences of: a) establishing digital contact with their primary care centre, b) coping with the digital communication system, and c) interacting digitally with the healthcare professionals. Only once the patient had replied to all queries, and an additional prompt to relay ‘any particular issues’ had been settled, was an inquiry for demographic details framed. The demographics included gender, age, residence, duration of symptom(s) or issue causing the primary care contact, and self-assessed digital literacy. Gender, residence, and digital literacy were the only structured questions, stated along with response alternatives (female/male/other; urban/rural; able to manage a mobile phone or computer well/fairly well/rarely without support).
The interviews were conducted by the first author over the phone during May 2019 at a date and time set by each patient. All interviews were voice recorded and later transcribed verbatim by the same researcher. Duration varied from 9.5 min to 21.5 min (mean 13 min, median 14 min).
Data analysis
Initially, an inductive, data-driven approach inspired by thematic analysis was applied to the transcripts. 34 The first step included listening to all the interviews and reading all the transcripts several times, to gain an overview of the whole data set. Secondly, words, sentences, or phrases corresponding to the study aim were marked as meaning units; every meaning unit was coded, with a brief description as close to the original content as possible. The codes were then organised into potential themes using a mind-map. Thirdly, the codes were formed into themes, consolidating yet considering the entire data set; each theme was defined, and framed to clarify its essence. An example of the analysis is provided in Table 1. Data extracts were selected and used to illustrate the themes. 39 The variation across interviews is indicated by the running number of each interview quoted.
Example of inductive analysis.

To conclude the analysis, the themes (and their content) were analysed in relation to the framework for person-centred care developed by McCormack and McCance 24 in a deductive approach.34–36 This phase included a detailed investigation of whether, and if so how, the themes corresponded to attributes of person-centred care, as well as whether and how the themes informed these attributes.
The first author performed the analysis in dialogue with the research team and supervised by the second author. Trustworthiness was strengthened by a continued dialogue about the emerging findings, particularly on the best understanding of the patients’ experience of the phenomenon. 34
Ethical approval and consent to participate
The study adheres to the ethical principles for medical research described in the World Medical Association's Declaration of Helsinki 40 and was approved by The Swedish Ethical Review Authority, (number 2019/04123). All patients provided individual consent, following receipt of study information in both written and verbal form. Data were stored safely, in accordance with the data management procedures of Linköping University, Sweden.
Results
Of the 16 included patients, seven were men and nine were women, aged 28 to 85 years. They represented patients across all five health centres. The reason for contacting their primary care centre had emerged at times varying between earlier the same day and up to six months previously. All the patients considered themselves able to manage a smartphone/computer well or fairly well. Further demographic details are given in Figure 1.
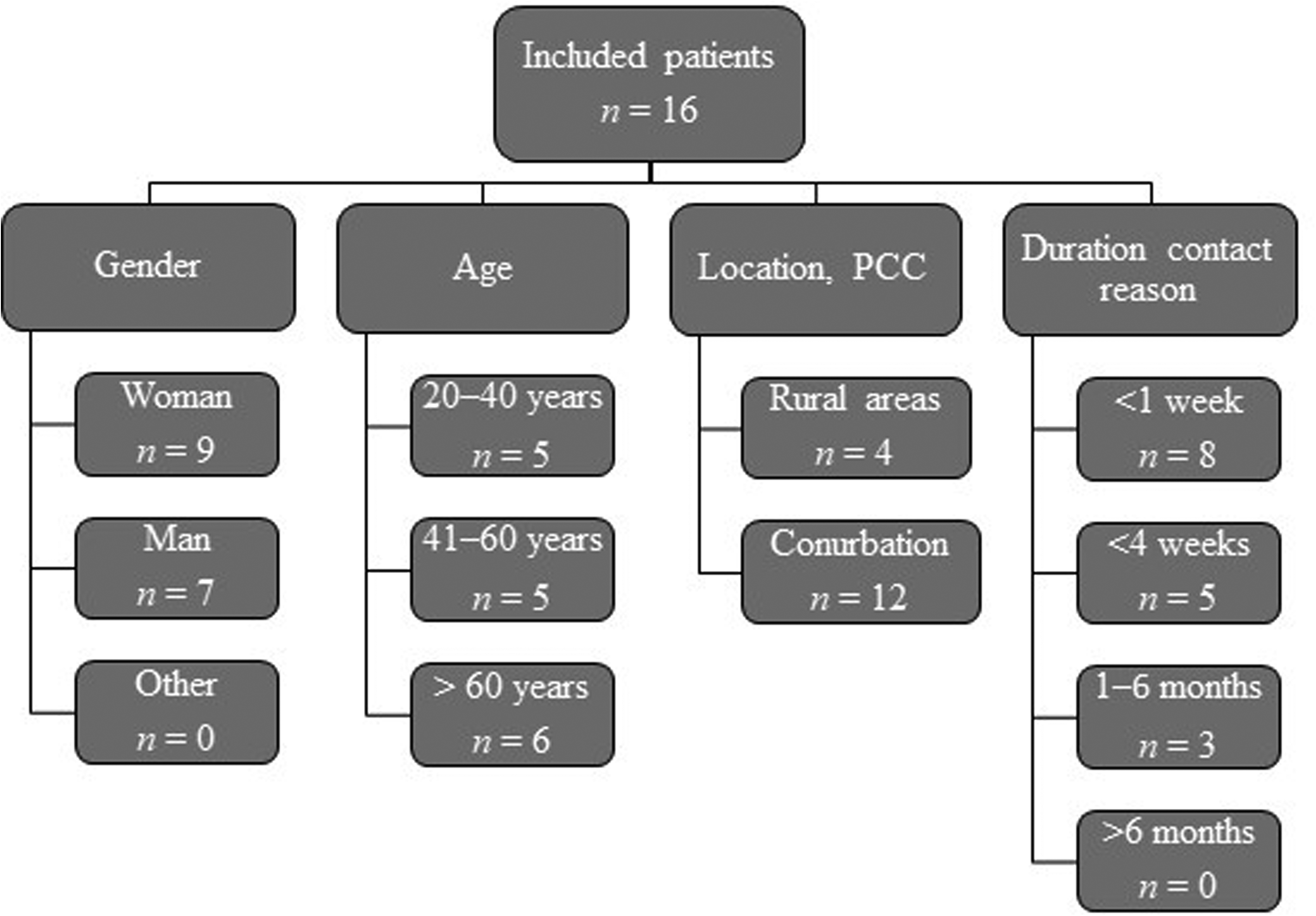
Demographic characteristics of the study participants.
The patients’ experiences of using a digital communication system when contacting primary care formed five themes: opportunities for independence; the significance of the reason for contact; digital communication posing barriers; crafting one's medical history in writing; and meeting the nurse digitally. (NB: the more general concept of ‘nurse’ is used throughout the results section, since the patients referred to the primary care provider as ‘the nurse’ or ‘nurses’ even though all the primary care centres were known to have registered nurses, RNs, conducting triage.)
Opportunities for independence
Digital communication was considered an ordinary part of society today. Thus, the patients anticipated that primary care would offer such a system for contact. The opportunity for a digital encounter with the primary healthcare centre encouraged a sense that the communication was on one's own terms; with the contact being initiated at a time that best suited oneself there was less need to change or cancel everyday activities to gain access to primary care, and there was no need to sit around and wait for a primary care telephone call. Simultaneously, the digital communication led to quicker contact and more prompt management of issues than the regular telephone contact. When the opportunities for contact over the phone were already fully booked for a particular day, the digital communication system still guaranteed contact, providing a sense of security. … I could control more myself than if I had to wait for a phone call … (No. 8)
Nevertheless, the patients had expected a synchronous chat, like the ones offered by their banks or when shopping online, rather than the interrupted sequence of information exchange and the lack of replies outside the primary care centre's office hours.
The significance of the reason for contact
With no information available as to when it was appropriate to use the digital communication system, the patients had engaged with the service for a variety of health issues. They described instances when the system was not very helpful: ambiguous symptoms were difficult to describe using the templates and/or free text, and some issues, such as mental health problems, were easier to describe when speaking to a nurse over the phone. Practical matters were made easier by the digital service, and digital communication was particularly helpful when the contact was due to a known diagnosis, and when fewer contacts were needed because the nurse could consult other staff before responding via the digital tool. … it depends a bit on why you’re contacting care … I just wanted an appointment for counselling. (No. 1)
Digital communication posing barriers
One's ability to write clearly and familiarity with expressing oneself in writing affected whether the digital communication became a support or not, and the potential inequity of the need for fluency when writing in Swedish, as well as having access to a computer or smartphone, concerned the patients.
Human contact was limited when using the digital communication system, and telephone contact was considered to provide more opportunities to ask questions and describe sensations and emotions; over the phone, there was also the opportunity for a mutual appraisal of nuances in the voice. In contrast, with written text the patients sensed that there was an increased risk of misunderstandings, and there were fewer opportunities with the written communication to clarify or confirm whether the nurse had understood or not. Although a telephone contact could be easier when experiencing language barriers, the digital encounter did allow time to use web-based translation tools when writing if Swedish was the patient's second language.
Using the digital communication system sometimes took longer than expected, particularly when it led to a prolonged chat. Participants did not consider the system to have been manufactured to facilitate patient use, but thought it had been designed for the primary care staff. … it’s easier to talk to someone, because they ask [questions] … then you can tell them how it feels and such … – it’s not the same when you write … (No. 16)
Crafting one’s medical history in writing
Once the entry was set up, the digital communication was intuitive, although picking a single reason for contact from the given list was challenging. The questions were sometimes relevant and adequate, and sometimes too numerous, unnecessary, or repetitive. Answering all the questions was time-consuming, although the opportunities to include free text were vital additions to the standard options. Fashioning one's own medical history in peace and quiet was an advantage, allowing enough time to ensure that everything one wanted to share was included. While it was essential to procure an accurate description of the reason for contact, the limit of one reason only for each contact made it difficult to sort out multiple, vague, or complex issues. … with so much free text, you could describe it in a good way, but if the free text hadn’t existed, if there’d only been questions, then I probably wouldn’t have felt comfortable … (No. 15)
Meeting the nurse digitally
The digital encounter with the nurse was simple, concise, and appropriate; the system provided the nurses with opportunities to read the patient's medical history and any previous chat before initiating another contact. Thus, the nurse was better prepared in the digital communication than with a telephone contact. However, a lack of technical skills by either party hindered the further queries needed to highlight vital issues in the digital communication. In general, the assessment or response from the nurse was associated with a sense of trust, even if or when the outcome deviated from what was expected. … one advantage, I think, was the chance to prepare the two-way communication, so the nurse was aware of why I’d contacted them and said more or less straight away that I had to see a doctor … (No. 2)
Patients’ experiences of the digital communication system in relation to person-centred care
The five themes were identified as encapsulating five person-centred processes: working with patients’ beliefs and values; engagement; sharing decision-making; having a sympathetic presence; and providing for physical needs. The five themes informed up to three person-centred processes each, as illustrated in Figure 2 and further described below.

The themes of patients’ experiences in relation to person-centred processes, considering McCormack and McCance’s framework. 24
Working with patients’ beliefs and values
As a patient using the digital communication service, one had opportunities to craft one's own history in writing. This was achieved by means of both structured response alternatives and free text, and constituted a kind of narrative for the nurse to consider. However, because only one matter at a time could be addressed in the digital communication service, this hampered the sharing of one's complete concerns if they were multifaceted. As such, the digital communication might accentuate a fractured vision instead of a more holistic perspective. Only the free text allowed patients to express themselves as persons, and unless they were confident and able to share more extensively in writing, digital communication posed barriers to presenting their beliefs and values.
Engagement
The nurses were thought to be more prepared when engaging in digital communication than when the patients used the telephone services; the nurse had had the opportunity to read their case, and sometimes also consult a colleague or catch up with other parts of their medical record. In this sense, the digital communication service enabled the nurse to fully engage with each patient's case.
Sharing decision-making
The opportunity for independence increased because the communication took place on the patient's own terms. But, because it lacked information about when it was appropriate to use it, the digital communication service did not fully enable a mutual sharing of issues. Rather, a lack of trust in the process provided by the service indicated a feeling that the technology was primarily designed for the healthcare staff, with patients’ need for human contact considered less significant. Yet, the digital service did facilitate the sharing of details considered important for the nurse's decision-making, allowing patients the time to express themselves and their concerns.
Having a sympathetic presence
Despite the lack of human contact in the digital communication, the patients felt the presence of the nurse whom they had met digitally. The nurse was more prepared and up to date than during any telephone conversation, where neither the nurse nor the patient really had time to prepare themselves. Yet, the sense of presence was limited by the asynchronous nature of the chat, and if one's history had not come across or been considered.
Providing for physical needs
Depending on the reason for contact, the digital communication service could constitute an opportunity for autonomy: patients could quickly and safely get in touch, ensuring that their physical needs were managed even when the telephone queue was full.
Discussion
The person-centeredness of this digital communication emerges as ‘what suits me as a person, in my role as a patient’, particularly due to the guarantee that further communication with the RN would take place shortly. In line with the need to better understand the user perspective on digital communication services in healthcare, this study provides a modest yet important illustration of the voices of primary care patients. The results are discussed in relation to the suggested outcomes of person-centred care, in accordance with McCormack and McCance's framework: 24 satisfaction with care; involvement with care; feeling of well-being; and creating a therapeutic culture.
Our findings illustrate that having the opportunity to initiate a healthcare contact at a time and place that suits oneself as a patient comes with a sense of satisfaction with care. Furthermore, the digital communication system provided a timely opportunity to establish a dialogue about one's health issue. Overall, the patients viewed this additional route favourably, but the digital encounter was not deemed a viable alternative to further face-to-face communication with primary care. Even though the digital communication service can serve as a means to easily initiate contact with the primary care provider, it has been found easiest for those with a certain level of digital and health literacy. 41 In this study, the digital communication created an opportunity for patients to think through and articulate both their case and any questions they had without being limited by time. Thus, nothing significant was forgotten and subsequent communication did not stray from the patients’ intended focus. 42
Health literacy means having or attaining a level of comprehension that suffices for involvement in everyday decisions concerning health and healthcare, disease prevention, and health promotion.43,44 Having sufficient health literacy affects patients’ ability to participate in healthcare decisions, and to take responsibility for their own health despite advanced health concerns, and it also provides increased capacity to navigate a complex healthcare system. 45 Consequently, being able to contact care providers digitally requires certain personal traits and competences, as well as technical skills and access to suitable digital devices. The absence of any of these factors will affect patients’ access to care.
Consistent with our findings, earlier studies have identified that the opportunity to tell one's story is influenced by personal circumstances, especially the ability to express oneself in written text. In order to be able to describe health problems and any associated feelings, a certain level of comprehension is required, 17 particularly in terms of mental health issues. 8 A recent study suggests that digital communication enables a full statement of one's health issue, providing for an uninterrupted medical history that cannot be easily dismissed in a further encounter. 41 While the patients in this study talked about difficulties in describing their health problems in writing, they found it particularly difficult to initially choose a primary reason for contact. The difficulty of classifying one's concerns as a patient emerges in other studies too, emphasising the need to adapt text sufficiently into plain language, yet in a precise form that enables patients to describe their issues.8,14
At the same time, the patients in this study struggled to determine how much and what type of information to provide; queries made via the digital communication system needed to match both patients’ needs when describing a health concern, and professionals’ need for an accurate description for triage in primary care. The number of questions asked should be proportionate to the complexity of the reason for contact. 8 Usually, more questions are needed to generate a sense of completion when patients have vague or complex disorders or symptoms, 8 and although free text can pose barriers to those who have trouble expressing themselves, it presents an opportunity for patients to tell their story in a way that fits the individual, in addition to being at a preferred time and setting. 42 Professionals in primary care have suggested that, by using a text written by the patient, they avoid the risk of interpreting or misinterpreting what the patient wants to express.12,14
Our findings, like those of others, suggest that enabling patients to communicate digitally with their healthcare organisation increases the opportunity for independence and enhances accessibility.32,42,46,47 Yet, written communication has been found to work better for facts, such as a reply to the question ‘Do you have a fever?’, while verbal communication is better for more extensive descriptions, such as a reply to: ‘Describe how this affects your situation’. 48 Our study emphasises that further interpersonal contact, and the ability to access non-verbal cues and tone of voice, are largely absent from digital communication systems.17,18,42 At the same time, asynchronous and faceless communication can aid patients to engage in an authentic conversation with their nurse.41,42 Hence, digital communication can be beneficial but cannot entirely replace in-person meetings, which are still needed for human interactions.38,49
Even though the therapeutic alliance may be limited by a mainly digital encounter, 23 digital innovations make it possible to transfer the healthcare encounter from the healthcare service point to the patient's home or workplace. This poses additional challenges to the caring relationship. 50 When using a digital communication system, the dialogue is primarily based on the patient's stance, which is further emphasised because the patient initiates the contact, largely determines its focus and content, and thus in a way controls the communication. 30 As such, digital innovations can promote person-centred care, as in ‘the formation and fostering of healthful relationships between healthcare providers and service users and their significant others’. 51 Nevertheless, our findings indicate that patients may be concerned that a more extensive adoption of digital innovations implies the favouring of non-complex healthcare issues that are easy to resolve, rather than caring for individuals with multiple or advanced healthcare needs, thus facilitating the healthcare organisation rather than the patients. 8 The implementation of digital services in primary care should be carried out with the aim of facilitating more person-centred services, 52 with cost-effectiveness as a secondary benefit.
Strengths and limitations
One benefit of a qualitative inquiry is the access it provides to understanding a common human experience, 53 although this requires transparent sampling, data collection, and analysis to ensure transferability. In this study, the number of participants was limited yet they were typical of general primary care patients, including a range of people of all ages, and both men and women. Telephone interviews are known to enable the inclusion of participants across a larger area, with a broader geographical distribution and opportunities for extensive responses, while preserving a sense of privacy, 54 and they served such purposes in our investigation. While relatively short, the interviews were found to exhaust all elements of the interview guide, and were in favour of the patients’ perspective. Throughout the data collection period, the researchers considered whether or not the experiences shared by participants signified a common illustration of the digital communication encounter. As the two final interviews provided no additional perspectives, but reinforced the existing perspectives and experiences already shared, data saturation was considered to have been achieved. 55 However, as all the participants considered themselves capable in terms of managing their computer or smartphone without assistance, the sample lacks representation of those with lower digital literacy. On the other hand, the sample included patients conversant in Swedish as either their first or second language, representing a more comprehensive experience of the digital encounter with primary care.
Conclusion
A digital communication channel to access primary care can be a good way to initiate healthcare contact, but it also implies certain limitations: patients’ knowledge, condition, and context as well as their sense of trust in the triage nurse's competence and ability to master the digital encounter will affect the outcome. Better, safer, and more person-centred care can be supported by digital communication because it increases independence, accessibility, and continuity. However, this requires the further development of digital communication tools and more extensive structures for understanding them from an end-user perspective, including patients’ experiences and preferences. Our findings show that patients’ experiences can provide an enhanced understanding of digital communication, and that patients are able to voice various nuances of interest to both healthcare organisations and manufacturers of digital communication systems.
Footnotes
Acknowledgements
We are grateful to the participants for sharing their experiences, and their time given in interviews. We are also grateful to the whole research team for engagement in this study and for the valuable input from senior lecturer E-L Nilsson, PhD, on an earlier version of the manuscript.
Author contributions
ES and ACE designed the study; ES planned and completed the data collection and analysis, supervised by ACE. ES drafted the manuscript in collaboration with ACE. Both authors made substantial contributions to the writing of the paper and agreed on the final version submitted.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.