
Abstract
Evidence-based practice (EBP) has been shown to improve patient safety as well as quality of care. Advanced practice nurses (APNs) have a vital role in the implementation of EBP. This study aimed to describe APNs’ experiences of EBP implementation. The study was a descriptive qualitative study and data were collected between May and August 2019 through interviews with APNs (n = 12). The data were analyzed using inductive content analysis. The study was reported according to COREQ guidelines. The responses were divided into four main categories: EBP in clinical nursing; EBP leadership; implementation of supporting structures for EBP; and EBP in APNs’ work. APNs experienced: that the realization of EBP varied in clinical nursing, that there was a need for development in the leadership of EBP, variation in nurse leaders’ competence in EBP leadership, and a lack of resources for EBP.
Background
The aim of evidence-based practice (EBP) is to harmonize, justify and ensure high-quality nursing practices regardless of the care unit, nursing employee, and client/patient. 1 EBP has been shown to significantly reduce healthcare costs2,3 and improve patient safety as well as the quality of care. 1 EBP refers to the judicious use of the best available evidence in decision-making related to healthcare, health promotion, patient care, and rehabilitation.1,4,5 In addition to the best available evidence, evidence-based decision-making takes into account the patient's or their relatives’ preferences, the context, and the professional judgment and expertise of health professionals.1,5 EBP requires a healthcare context in which staff has the competence to search for, synthesize, transfer, and use evidence in the implementation of practical nursing work. 1 Various EBP experts, such as advanced practice nurses, have been educated to perform these EBP tasks.6,7
Advanced practice nurses (APNs) include clinical nurse specialists (CNSs) and nurse practitioners (NPs), with both having distinct roles in the implementation of EBP. 6 EBP-related tasks of CNSs cover evidence transfer and implementation, harmonization of practices, development and support, monitoring the use of evidence on units, and immediate patient care. 8 According to the International Council of Nurses (ICN), CNSs lead in advancing nursing practice by teaching, mentoring, consulting, and ensuring that nursing practice is evidence-based. 9 NPs, on the other hand, have comprehensive nursing skills which enable them to independently examine and assess a patient's need for care, start treatment, and monitor both acute and chronic health issues. 6 The ICN has stated that NPs are mainly responsible for immediate patient care within diverse clinical settings, while CNSs perform indirect care and support clinical excellence through a systems approach.9 A master's degree is the minimum degree requirement for becoming an APN. 10
In addition to the utilization of experts or mentors in EBP,1,11 evidence-based activities can be promoted through interaction, communication and networks,10,12 via strong leadership,10,13,14 through feedback, monitoring and evaluation, 10 through an open organizational culture that supports learning and values, and by having adequate financial and human resources along with a reward system for nursing staff involved in the development of the EBP. 1 The knowledge and skills of healthcare leaders is a crucial factor in the creation of a culture and environment that supports EBP.1,13 This responsibility of healthcare leaders is important because it significantly impacts nurses’ adherence to EBP. 7 Clarification of the roles of experts in EBP facilitates the building of a culture and environment that supports EBP. 1 Work units should have EBP mentors who provide ongoing and personal support in addition to hands-on exercises that promote the adoption of new practices. 15 EBP is promoted through the development of EBP expertise of nursing staff.1,16 Structures that support EBP include regular research meetings and updates, support of leaders, and resource allocation. 15 Leadership plays a major role in EBP implementation, as EBP can be most effectively influenced by individuals with the greatest authority over the pillars of EBP, such as nursing, education, resources, and leadership. 16
Barriers to the implementation of EBP in clinical nursing practice include nurses’ work overload,15,17 unwillingness to change practices, insufficient understanding of research methods, 17 weak collaboration between physicians, nurses, and nurse leaders, along with a lack of appreciation for employees and organizational support. 18 Another obstacle to the implementation of EBP may be the insufficient use of different organizational support structures, such as training, dissemination of information, and integration of evidence. 12 Nurses play a key role in the implementation, development, and use of the latest evidence in clinical environments.18,19 Research has found that although nurses have high levels of positive attitudes towards, knowledge about, self-efficacy, and skills in EBP, their level of EBP behavior has been low. 20 Most nurses consider their existing EBP competence to be insufficient.7,21
According to a WHO report, 5 the EBP Action Model of Expertise (FinAME) has been created to strengthen EBP implementation and clarify the roles and responsibilities of various experts in the development and implementation of EBP in Finland. The FinAME model divides EBP experts into four different groups based on tasks, the scope of tasks, and competence: nurses in clinical care; specialized nurses in clinical care; CNSs; and specialists in clinical nursing science. 5 Certain competence criteria have been identified for CNSs,5,6,22 but these criteria have not been validated in the Finnish context. 11 Furthermore, there are inconsistencies in the work descriptions for CNSs. However, the FinAME model has not yet been sufficiently implemented, and up-to-date information about implementation of EBP is needed to introduce this model.
In this study, the APN is represented by CNSs whose work description include immediate patient care and the development of EBP in the organization. Certain competence criteria have been identified for CNSs,5,6,22 but these criteria have not been validated in the Finnish context. 11 Furthermore, there are inconsistencies in the work descriptions of CNSs. This study focused on APNs due to their responsibility in promoting and supporting EBP implementation at the work unit and organizational levels. 11 Hence, they are capable of assessing EBP implementation and related factors. This study was performed because research on this topic is limited in Finland, and EBP implementation varies on an international level.
The aim of this study was to describe APNs’ experiences of EBP implementation in the Finnish hospital setting. The objective was to gain information for the development of EBP, APNs’ work descriptions and competence, as well as for competence development in hospitals. Study results can be used to develop EBP activities and competence of APNs, to clarify the work descriptions of APNs, and to further develop the Action Model of Expertise in social and healthcare organizations.
Methods
A qualitative, descriptive approach was used to both obtain information into APNs’ experiences and generate a comprehensive summary of the collected information. Data were analyzed using inductive content analysis. As this research was based on the interpretive paradigm, findings were identified through the researcher's values and interpretation in a particular context and moment.23,24 The Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist was used for reporting. 25
Participants
Study participants were selected through purposive sampling to ensure informants were relevant for the study. 26 The inclusion criteria included being a full-time or part-time APN in a hospital and having at least one year of work experience as an APN. The study was conducted in two university hospitals. 27 The study included a total of 12 volunteer interviewees who met the selection criteria. Two men and ten women participated in the study. The average age of the participants was 47.5 years. Three of the participants had a master's degree from a university of applied sciences, seven had a master's degree in nursing science, and two had a doctorates in nursing science. The participants had an average of 3.25 years (range 1 to 7.5 years) of work experience as APNs. In the APNs’ work descriptions, the proportion of immediate patient care varied; three participants worked 50% of their time in immediate patient care, three worked 10–30% in immediate patient care and six did not work in immediate patient care at all. The leadership of APNs was organized in different ways in the two studied organizations. In one organization, all of the APNs (n = 6) were managed by the same nurse leader, while APNs from the other organization (n = 6) had different nurse leaders.
Data collection
Data were collected between May and August 2019 through face-to-face thematic interviews. The themes of the interviews covered the implementation, pre-conditions, and development of EBP. This study reports findings related to the implementation of EBP. The themes and prompts were pre-tested on one APN prior to the actual interviews.26,27 This interview was not included in the research data. No changes were made to the interview themes and prompts based on the pre-interview.
The interviewees were recruited with the help of contact persons from the participating organizations. No participant refused participation in the study. Interviews were arranged in advance and conducted during the interviewees’ working hours in a quiet place at the hospital to minimize distractions and interruptions. Only the interviewee and interviewer were present during the interviews. The interviews lasted from 28 to 85 minutes and were audio-recorded with the interviewees’ consent. No field notes were taken during the interviews. The recorded data were transcribed by the interviewer and resulted in 153 pages (12-point font size, 1.5 line spacing) of text. The transcribed text was checked by comparing the text with the recorded interviews.
Data analysis
The analysis proceeded systematically and objectively. 27 Data were organized, structured, and reduced without changing the meaning of the information.23,24,26,27 The researchers read the transcripts through several times before starting the analysis in order to become familiar with the data and obtain an understanding of the entire data. Data analysis was conducted by three researchers and guided by the purpose of the research and the research question. Only the manifest content was analyzed through the researchers’ interpretation. A sentence was chosen as the unit of analysis.
The original quotations were coded as open codes (n = 237). Open codes with similar content were grouped using an Excel table and divided accordingly into sub-categories (n = 36). The sub-categories were combined into categories (n = 10) based on similarities in content, and – in the last step of analysis – main categories (n = 4) were formed from the categories. The main categories were thus derived from the data and answered the research question. Saturation of the research material was achieved after ten interviews. The inductive analysis proceeded on the basis of the information provided by the interviewees towards a common perspective of the interviewees.23–25 Table 1 provides an example of how the various categories were formed.
An example of how the categories in this study were formed.
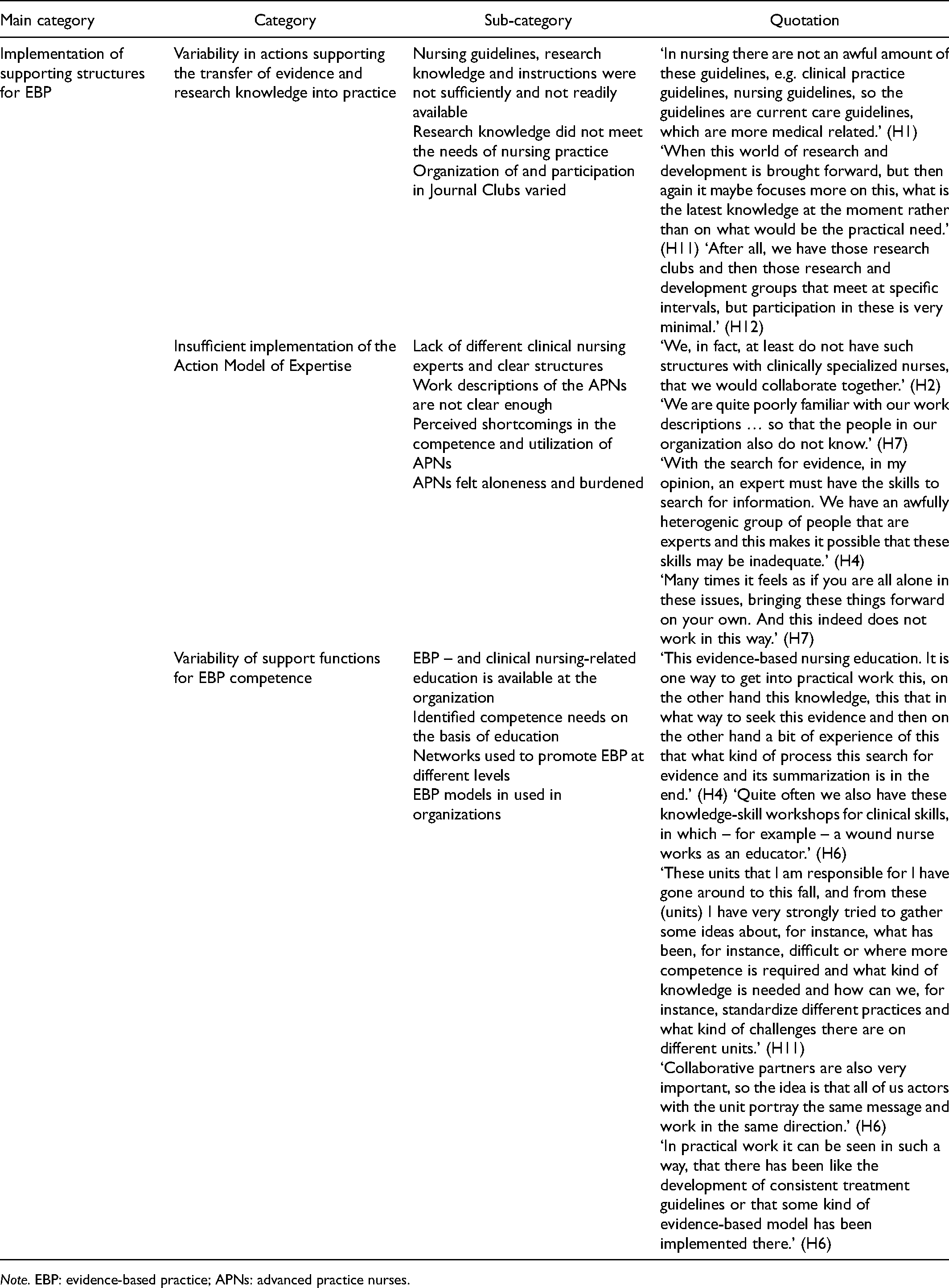
Note. EBP: evidence-based practice; APNs: advanced practice nurses.
Ethical considerations
The research followed the principles of good scientific research, which included applying for a research permit, accurately describing the entire research process, appropriate citation of references, stating important conflicts of interests, and clarifying the rights and obligations of the research parties. 28 Research permissions were obtained from the head nursing officers of the hospital districts. Interviewees who met the inclusion criteria were contacted via email and all interested participants were included in the study. Each interviewee was informed of the purpose and objective of the study, as well as their right to withdraw from participation at any stage, both verbally and in written form. 28 In addition, the anonymity of interviewees was ensured throughout the study. Interviewees gave written consent to participate in the study.
The researchers ensured that possible adverse effects for study participants were minimized. The collected data were stored as protected files in accordance with the provisions of the General Data Protection Regulation, 29 and were preserved based on the principles of scientific research. 30 The results were published openly and honestly. 28 The researchers ensured that none of the interviewees could be identified based on the reporting of the study. 26
Findings
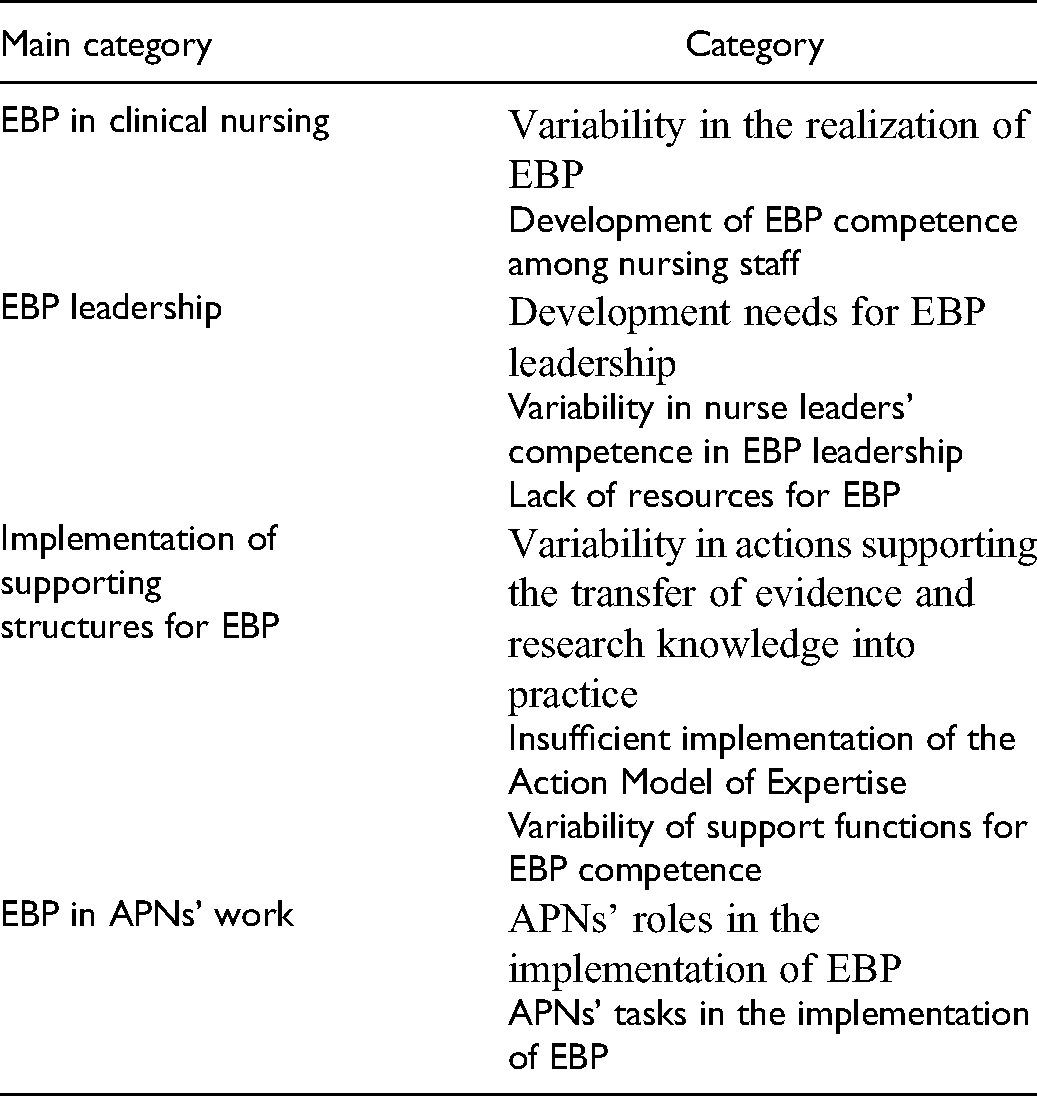
APNs’ experiences of evidence-based practice implementation in two Finnish hospitals were formed into four main categories: EBP in clinical nursing; EBP leadership; implementation of supporting structures for EBP; and EBP in APNs’ work (Table 2).
Advanced practice nurses’ (APNs’) experiences of evidence-based practice (EBP) implementation divided into main (n = 4) categories and categories (n = 10).
EBP in clinical nursing
The main category of EBP in clinical nursing included variability in the realization of EBP and the development of EBP competence among nursing staff. Variability in the realization of EBP described challenges in the realization of EBP, differences in the extent to which EBP had been implemented across units, and the use of traditional action models. Nursing staff also has knowledge on how something should be done, although then it is not always completed in this way on a practical level, but there is variability and inconsistency in nursing care. (H3)
The APNs experienced that the EBP competence of nursing staff had developed. More specifically, awareness of EBP had increased within clinical nursing, but in-depth EBP understanding still varied between nurses. Attitudes of nursing staff towards EBP varied and skills in utilizing evidence were insufficient. Indeed, people’s awareness has increased of this that care must be based on research knowledge. (H7)
But then this who understands how deeply the meaning of the term varies in my opinion. (H6)
EBP leadership
The APNs experienced that the main category of EBP leadership comprised the development needs for EBP leadership, variability in nurse leaders’ competence in EBP leadership, and a lack of resources for EBP. The category development needs for EBP leadership included descriptions of how leadership is not evidence-based and insufficiently supports EBP. In addition, according to the APNs, nurse leaders were involved in the development of EBP in various ways, the division of work descriptions and roles related to the development of EBP was varied and unclear, and monitoring information that had been collected could not be sufficiently utilized. The development of EBP lacked planning and was not systematic. In my opinion, like in nursing practice, evidence-based practice is many times considerably ahead of for example evidence-based management. (H4)
There is a lot of monitoring information, but then whether or not this monitoring information is utilized is yet another issue. (H10)
According to the APNs, the category variation in nurse leaders’ competence in EBP leadership described how there are differences in the understanding of EBP as a concept and the need for development in competence in EBP leadership. For the most part, nurse leaders had a positive attitude towards evidence-based action. That at the management level there still certainly would be the need to fix this, that the understanding would be more, that evidence-based nursing and evidence-based management could be able to be differentiated and in this way the levels are a bit different. (H4)
According to the APNs, one category was a lack of resources for EBP, which was described in several different sub-categories. Nursing staff did not have time to find out about evidence-based treatments; there were shortcomings in human resources; unit-specific development activities were reduced; and financial resources were not sufficient for development activities. The possibilities for completing things varies considerably. For nursing staff it is the most challenging because work contains a fairly small amount of such time, that you can find out things. (H5)
… development is then like the first that is eliminated, if there is no time for something. (H9)
Implementation of supporting structures for EBP
The implementation of supporting structures for EBP was identified as a variety of actions supporting the transfer of evidence and research knowledge into practice, insufficient implementation of the Action Model of Expertise as well as variability of support functions for EBP competence. Variability in actions supporting the transfer of evidence and research knowledge into practice showed that nursing guidelines, research knowledge and instructions were not sufficiently and easily available, research knowledge did not meet the needs of nursing practice and that the organization of and participation in Journal Clubs varied. People do not read guidelines, they cannot find them. They are somehow not easily accessible in practice when you need the information about how do I do something. (H10)
We have not had this kind of Journal Club activity. (H6)
Insufficient implementation of the Action Model of Expertise (FinAME) was experienced to be due to a lack of different clinical nursing experts and the lack of clear structures in the FinAME. In addition, the definition of the work descriptions of the different clinical nursing experts was not clear enough. There were perceived shortcomings in the competence and utilization of APNs, and APNs experienced that they felt alone and were burdened. I believe that we still have those who do not know that we even have clinical nurse specialists or what their work description is. (H8)
Our research competence, that which we have, we should be able to also do a little more of in this work. (H3)
Variability of support functions for EBP competence included the varied use of different supporting structures to develop EBP competence. These supporting structures consisted of education in EBP and clinical nursing in the organization, identified competence needs on the basis of education, networks used to promote EBP at different levels (organization, national and international), and EBP models used in organizations. In this organization we hold (evidence-based practice) education. (H3)
We have this kind of network of contact people whom we educate. We inform them on these new guidelines and then distribute these to them and then also to leaders. (H10)
EBP in APNs’ work
EBP in the APNs’ work was identified as the roles and responsibilities of APNs in their work. APNs played significant roles in the implementation of EBP at the unit, organizational, national, and international levels. Their main role was the promotion of EBP, but they also had advocacy, coordination, and consulting roles in relation to EBP. They were involved in organizational, national, and international research and development work as well as networks. The role of our experts is like perhaps more of this kind of coordinating and consulting overall. (H1)
Yes, it is exactly this, that in my opinion it is at such a national level this promotion of evidence-based nursing and specifically nursing. (H7)
The APNs had different tasks in the implementation of EBP. Tasks were divided into tasks related to critical review of nursing activities at different levels of the organization; to finding and producing evidence; to disseminating evidence and to preparing, planning, supporting, implementing and evaluating the implementation of EBP policies. After all, we use a lot of these kind of models, that have already been compiled from nursing guidelines. We bring them and prepare for implementation, so we make plans, schedules and this education and then we mentor alongside (staff), and monitor what problems there might be and help with these and with solving them together with the people (staff). (H6)
Discussion
In this study, APNs experienced that EBP was implemented in a varied manner and clinical practices were still partly based on traditional practices and models in the hospital setting. The EBP competence of nursing staff had increased, although it varied. A new finding in this study was that the gap in competence was related to the in-depth understanding of EBP. The finding that the implementation of EBP in clinical work varied was consistent with what has been previously reported.7,20,21 This may be influenced by reluctance to change practices; overload of nursing staff;15,17 lack of EBP mentors; 15 lack of employee appreciation and organizational support; poor cooperation between nurses, physicians, and leaders 18 as well as lack of competence in EBP among leaders. 7 Indeed, EBP leadership is a key factor in the implementation of EBP.10,13,14,16
In this study, the APNs experienced that leaders’ EBP leadership competence needed further development, and leadership did not support the implementation of EBP. The result is significant because leaders’ EBP management competence affects the creation of an EBP working culture and environment, and the resources needed to develop the supporting structures in EBP.1,15,16 APNs also estimated that healthcare organization leaders need to develop their evidence-based healthcare competence to support the implementation of EBP in the organization. APNs identified specific management challenges, which included a lack of clarity about the EBP roles of APNs, registered nurses (RNs), and nursing leaders; the fact that development was not planned and systematic; and that there were insufficient resources for EBP implementation and development. Leaders of healthcare organizations should work to overcome the above-mentioned barriers identified by the APNs to enhance the implementation of the EBP.
This study found education to be the most commonly used supporting structure for EBP. This is a relevant finding as previous research has found education to play an important role in the implementation of EBP.1,12,16 On the other hand, the identification of competence needs, the network cooperation used to promote EBP and the EBP models of organization were also support structures for EBP dissemination that emerged in this study. However, the challenge was the difficulty of implementing and utilizing evidence-based information, which was partly due to the lack of different nursing professionals (APNs, specialized nurses, RNs). The lack of different nursing experts was also reflected in the shortcomings in the implementation of the developed FinAME model. For example, nurses did not have time to look for EBP models they needed in patient care alongside practical nursing. In addition, the APNs did not have enough time or there were not enough APNs, so they were not able to discuss EBP models with other nurses. These shortcomings will weaken the use of the best available evidence in clinical practice.4,5 EBP mentors should be utilized to provide ongoing and personal support, which would help garner acceptance for new ways of working.5,15
APNs experienced EBP promotion as a lonely and burdensome task. The interviewees mentioned a lack of an identified nurse practitioner and a collaborative network that included the nurse practitioner. In addition, half of the APNs had clinical responsibilities in addition to the promotion of EBP, which increased their workloads and proved challenging. A new finding was that the loneliness experienced by APNs was exacerbated by the lack of collaboration with other APNs in the same organization. The work tasks of the APNs were to apply scientific knowledge, disseminate evidence, 6 guide EBP implementation at the work unit level and measure the results of EBP processes.1,6 However, guiding and controlling the implementation of EBP at the work unit level would be the task of the EBP mentor,5,6 while nurse leaders should support the implementation of EBP in the work unit. 15 However, this study revealed that nurse leaders were involved in EBP development to varying extents because a significant share of their working time was spent on administrative tasks. It should be noted that this study contained solely the APNs’ experiences on the subject.
In addition, the work of APNs was characterized by wide areas of expertise and unclear work descriptions in organizations. Unclear work descriptions for APNs may cause an accumulation of tasks that are unrelated to their work and do not meet the target of EBP development.6,8 The work descriptions of APNs vary; for example, the Canadian Nurse Association and the International Council of Nurses had defined their own competence criteria for both CNSs and NPs,9,22 while the European Federation of Nurses Associations had determined common competence criteria of APNs. 31 The APNs interviewed in this study were heterogeneous in terms of age, education, work experience, working hours and duties. According to an ICN report, the complexity and variability of APNs’ tasks and education have also caused confusion about APNs’ work. 9 The ambiguities and variability of the assignments may have been due in part to the different educational backgrounds of APNs that resulted in different abilities to perform their tasks. In this study, it was found that some of the APNs were experienced in conducting research and producing research information, but they had very limited possibilities to conduct research during working hours.
APNs felt that, in addition to their broad EBP promoting roles, they also had an advocacy, consultation, and coordination role. A notable finding was that the participating APNs did not strongly identify their leadership role, even though the promotion of leadership competence and the integration of research competence has been emphasized as a key area in the education and work descriptions of APNs. For example, education for APNs in the United Kingdom includes four coordinated approaches: clinical practice; leadership; education; and research. 10 According to this study, the clarification of the work descriptions and competence criteria for various EBP experts and the harmonization of education must be developed further if EBP is to be successfully implemented in Finnish healthcare organizations.
Limitations and strengths
The validity of this study was assessed based on dependability, credibility, transferability and authenticity. 32 The dependability of the study was enhanced by the use of a qualitative approach and methods that generated a comprehensive summary of APNs’ experiences and which were appropriate for the purpose of the study. The research process was carefully described, the results objectively reflected the information provided by interviewees, and an example (Table 1) of the analysis process was shown so that the research process can be evaluated and reproduced by other researchers. 26
To improve credibility, the research team members checked the analysis results and referred to the original data several times during the analysis to ensure that the results remained unchanged, and the results reflected the interviewees’ opinions and statements. 27 The researchers had no previous interaction or relationship with any of the participants before commencement of the study, nor any preconceived notions of the phenomena of interest, both of which circumstances facilitated objective data collection and analysis. 25 Nevertheless, it is important to state that it is impossible to achieve complete objectivity in content analysis. For this reason, original quotations from the interviewees have been included so that readers can assess the consistency between the original data and the researchers’ interpretations of APNs’ experiences. This choice was made to increase the authenticity of the study.26,27,32 One limitation of the study is that the data were not returned to the participants following data analysis. The EBP experiences reported by the participants in the interviews reflect the experiences of the implementation of the EBP at the time of the interview, which might have been changed afterwards due to the continuous development of EBP in the organizations. The quotations were translated by a native English speaker with competence in the Finnish language. Some nuanced meanings expressed in the APNs’ original statements may have been lost during the translation process.
To improve transferability, the context of the study, including background information of the interviewees, was presented in a sufficiently broad and detailed manner while still maintaining interviewee anonymity.27,32 The researchers make no claims about the generalizability of the findings as the study included a limited number of Finnish APNs and leave it to readers to determine whether the research results are applicable to other contexts.
Conclusions
The results suggest that Finnish healthcare faces similar challenges as healthcare internationally. The main challenges in Finnish healthcare are the lack of EBP skills among staff and leaders, unclear roles of different professional groups in developing and implementing EBP, and the lack of support structures and resources for EBP. Other challenges included the variability of APN education and the scarcity of APNs in healthcare organizations. However, the EBP skills of healthcare staff have improved, although a deep understanding of EBP is lacking. This is a positive finding, although much remains to be done to promote EBP. Leaders of healthcare organizations should understand the context of evidence-based healthcare as a whole and identify and systematically develop factors that support the promotion of EBP.
The roles of EBP leadership, supporting structures, and APNs need to be further developed to ensure the systematic development and implementation of EBP. Adequate resources should be effectively allocated to improve EBP competence among nursing staff and leaders. Developing appropriate supporting structures (such as adequacy of CNSs and nurse practitioners and work descriptions of EBP experts) is crucial to meeting this objective . In addition, to ensure the implementation of EBP, close and effective cooperation is needed between the different levels of the healthcare organization. Further research is needed to clarify the roles and competence criteria of the various EBP experts and to determine which EBP supporting structures are most appropriate for healthcare organizations.
Relevance to clinical practice
In social and healthcare organizations, it is important to identify gaps in the EBP competence of nursing leaders and nursing staff. Clear roles should be created in organizations for different experts for the implementation of EBP, and plans developed for further education based on the competence gap in EBP. In addition, organizations should ensure adequate resources, cooperation networks, and operational support structures are in place for the implementation of EBP. Implementing EBP requires systematic action to which all members of the organization should commit. The results of this study can be used to develop EBP activities and competence of APNs, to clarify the work descriptions of APNs, and to further develop the Action Model of Expertise in social and healthcare organizations.
Footnotes
Acknowledgements
The authors would like to thank the APNs who participated in the study and the associated contact persons for their identification of eligible interviewees.
Author contributions
SY, MK and A-MT made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data. All authors were involved in drafting the manuscript or revising it critically for important intellectual content. All authors have given final approval of the version to be published. Each author has participated sufficiently in the work to take public responsibility for appropriate portions of the content. All authors have agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of Finland and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. 28 Participants were informed that they could stop the interview at any time. Enrolled participants provided written informed consent for participation and publication. Under the guidelines of the law of medical research, an approval of an ethical committee was not required in this study.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.