
Abstract
Colorectal cancer affects a large number of people aged ≥80 years. Little is known about how they manage after discharge from hospital. The aim of this study was to explore the experiences of individuals aged ≥80 years recovering from surgery for colorectal cancer, and the challenges they may encounter after discharge from hospital. Data were collected between January and March 2016 through in-depth interviews with ten participants approximately one month after surgery. Inductive thematic analysis was employed to analyse the data. The COREQ checklist was used in reporting this study. Two themes were identified: Managing the recovery from CRC surgery, and Insufficient follow-up from the healthcare services after CRC surgery. The findings indicate that older people treated for colorectal cancer manage surprisingly well after discharge despite challenges in their recovery; however, there are seemingly areas of improvement in their follow-up healthcare.
Colorectal cancer (CRC) is one of the most frequent malignant diseases worldwide with approximately 3.5 million people affected annually, including a large number of patients aged ≥80 years. 1 Surgery is the mainstay for cure, occasionally together with neoadjuvant therapy, and may sometimes involve the creation of either temporary or permanent stoma.2,3 During and after treatment, disturbing symptoms can occur caused by the treatment itself or the cancer, and older people are particularly susceptible.2,4 As the proportion of older people in Western populations is growing, the prevalence of CRC survivors is expected to rise during the coming decades. 3 Furthermore, according to national guidelines in Norway, the postsurgical care of patients aged ≥80 years after curative CRC surgery is determined individually outside of systematic follow-up programmes, 5 resulting in limited knowledge of their recovery process. Greater knowledge about the recovery process of older CRC survivors in primary healthcare is essential for facilitating optimal recovery after discharge.
Because of the advances in diagnosis and treatment in addition to greater public awareness, more people are living with cancer as a chronic condition. It is estimated that 40% of cancer survivors in Norway are people aged ≥80 years. Most people in this age group have at least one chronic condition and are susceptible to age-related impairment of cognitive and physical function 6 in addition to the impact of the cancer treatment. The members of this heterogeneous group range from individuals with good health to those with increased vulnerability in terms of treatment and complications. 7 A study from 2019 showed that postoperative complications such as anastomosic leak, delirium and septicaemia occurred in a third of older people surgically treated for CRC. 8 Half of older patients reported a decrease in physical functioning after surgical treatment for CRC. 9 Nevertheless, Devon, Urbach and McLeod 10 found that 78% of older CRC surgery patients returned home after discharge. Nearly half of the older patients were in need of care when discharged from hospital compared with their younger counterparts, where only 20% required assistance. 11 Younger people treated for CRC received homecare nursing, while older people treated for CRC also needed assistance with household tasks and care from multiple professions. 10 Nearly half of all CRC survivors were found to have unmet supportive care needs after discharge. 12 In their study, Samuelson et al. pointed out the lack of knowledge about the oldest old with CRC. 13 They found incomplete information and confusion regarding which section of the healthcare service was responsible for follow-up. 13 Hence, the knowledge regarding older patients’ experience of recovery after discharge from hospital is limited. How older people treated for CRC experience challenges after discharge is little explored and understood. The aim of this study was to explore the experiences of individuals aged ≥80 years recovering from surgery for CRC and the challenges they may encounter after discharge from hospital.
Method and design
This study employed an exploratory qualitative design 14 as a qualitative inductive approach was considered appropriate for exploring older individuals’ experience of postsurgical recovery. 15 The study adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist 16 (see online supplementary material, file 1).
Participants and recruitment
The participants were recruited from a gastrointestinal surgical department in Western Norway. Purposive sampling was used to obtain maximum variation regarding type of cancer, functional status and gender to capture a wide range of experiences. 17 The inclusion criteria were elective curative resections for colorectal cancer stage I-III and age ≥80 years. Exclusion criteria were cognitive impairments and being unable to speak and read Norwegian. A member of the healthcare personnel not affiliated to the project identified and recruited eligible patients during admission for surgery and provided them with written and verbal information regarding the study. Patients who considered participating gave permission to transfer their contact information to the researchers. The first author contacted the individuals in question to provide more verbal information, including information pertaining to their rights as participants, to obtain consent and to arrange an appointment for the interview one month after surgery. No relationship was established between the researcher and the participants prior to study commencement. Although 12 participants were recruited, the medical condition of two participants deteriorated, resulting in cancellation of their interviews. The final number of participants interviewed was thus ten. One week before the interview, the participants received a phone call from the first author to confirm the appointment.
Data collection
Data were collected by the first author (KSE) from January to March 2016 through individual in-depth interviews. The interview guide was developed by the research group based on the research objective and relevant research18–21 (see online supplementary material, file 2).
Nine of the interviews took place one month after recruitment, while one was conducted after two months. The duration of the interviews ranged from 48–80 minutes and all interviews took place in the participants’ homes. During two of the interviews a spouse was present in the room but did not participate. The interviewer presented her clinical and academic background before the interview started. The opening question was ‘How did you experience coming home from the hospital?’ Follow-up questions were posed to gain a deeper understanding of the participants’ statements. The interviewer made field notes to navigate through the interview, but the notes were not included in the analysis. The first interview functioned as a pilot, but as no major changes were necessary it was therefore included in the data analysis.
Data analysis
All interviews were recorded and transcribed verbatim. The audiotape was then compared to the transcripts to ensure accuracy. The transcripts were returned to one participant on request, which resulted in no comment or correction. The empirical data were analysed in accordance with thematic analysis by Braun and Clarke, 22 a semantic analysis that identifies and provides a rich description of patterns across the dataset. The analysis consists of six phases: 1) Familiarizing oneself with the dataset, 2) Generating initial codes, 3) Searching for themes, 4) Reviewing themes, 5) Defining and naming themes, 6) Producing the report.
A research team consisting of the first author (KSE), second author (SIEH) and last author (KL) conducted the analysis. Two of the researchers (SIEH and KL) had experience of qualitative research methods and worked as academics, while the first author (KSE) was a doctoral fellow at a university. At the beginning of each phase a team meeting was held to develop and maintain a shared understanding of the dataset, coding, themes and the next phase of the analysis. Subsequently, KSE conducted the analysis accordingly.
In phase one, the transcripts were subjected to repeated reading to become familiar with the width and depth of the dataset and ideas for coding. In phase two, the initial codes were generated and systematically ordered into a coding manual linked to the appurtenant data extract. In the third phase, codes and the corresponding data extract were sorted into initial themes in a new document grounded in patterns in the dataset. A preliminary thematic map was generated to provide a visual impression of the findings and inherent relationships. 22 In phase four, all data extracts were re-read to ensure a consistent pattern within the different themes. Two themes were downgraded to sub-themes, two themes were reorganized to attain heterogeneity and one theme was removed. The themes were systematically ordered into new documents and revisions were subsequently conducted in the thematic map. In phase five, the names of every theme and sub-theme were refined and adjusted to capture their essence. The findings were written down and the refinement of the themes was again critically assessed so that, together, the themes told the tale of the dataset as a whole. 22
Ethical considerations
The study was approved by the Regional Committee for medical and health research ethics (REK Vest 2015/1500) and the hospital. Eligible participants received verbal and written information about their right to decline participation without any repercussions; that participation was of a voluntary nature thus they could withdraw from the study at any time and that all information they provided would be treated confidentially. Written informed consent was obtained from each participant before enrolment in the study.
Results
The participants were equally distributed between males and females and aged between 80 and 85 years. Seven out of ten had colon cancer and four received a stoma. To further characterize the participants: one received neoadjuvant treatment. Four were diagnosed with an unrelated disease during the presurgical examination; one was sufficiently covered with new medication, and two received further examination after the CRC surgery and recovery. Two had additional surgery, one before and one after the CRC surgery. Additionally, one was re-admitted shortly after returning home due to a serious postsurgical complication that required a lengthy hospital stay. A majority managed without a mobility aid, lived in urban areas and four lived with a spouse, while the rest lived alone. Participant characteristics are presented in Table 1.
Characteristics of the participants, n = 10.
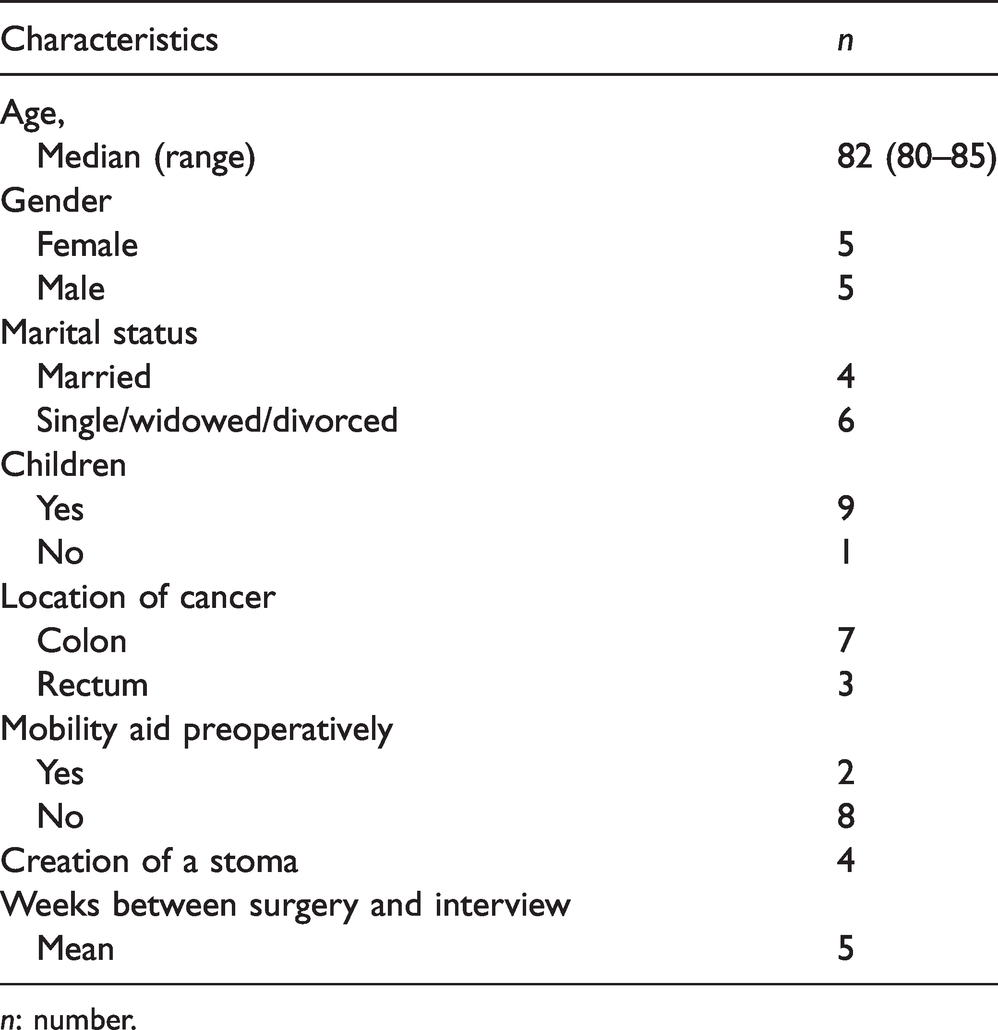
n: number.
At the beginning of the interviews, the participants reported that their recovery from CRC went quite well and described few challenges in their daily life. However, during the interviews a more detailed story emerged about situations that had been difficult to handle. Two themes were identified through the analysis: Managing the recovery from CRC surgery and Insufficient follow-up from the healthcare services after CRC surgery based on four and three sub-themes respectively (see Table 2).
Overview of themes and sub-themes.
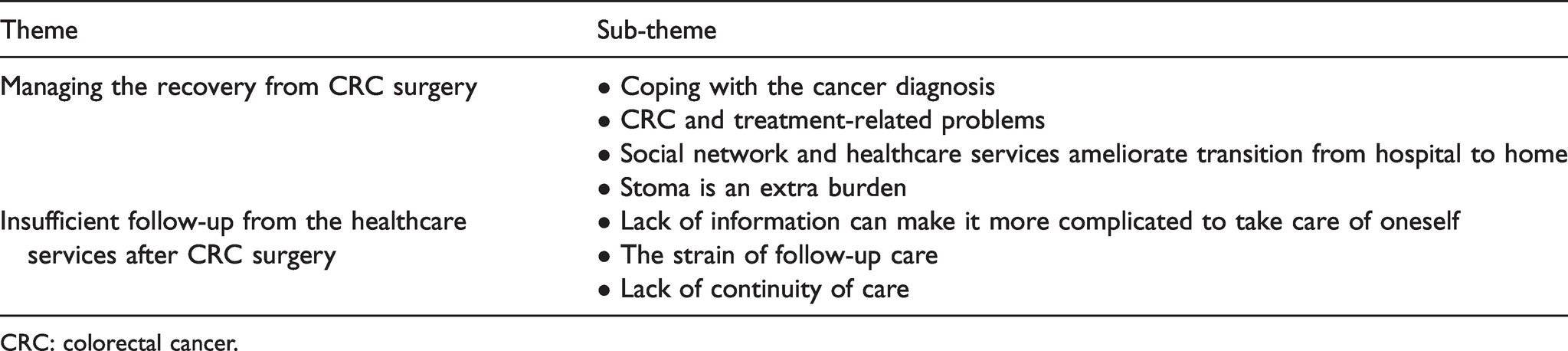
CRC: colorectal cancer.
Managing the recovery from CRC surgery
This theme describes how the older participants experienced the recovery process, how they coped and which resources they used to manage. An overall impression was that they exhibited an inherent resilience gained through life experience in the way they coped with the challenges of cancer and recovery. This theme consisted of the following sub-themes: Coping with the cancer diagnosis, CRC and treatment-related problems, Social network and healthcare services ameliorate transition from hospital to home and Stoma is an extra burden.
Coping with the cancer diagnosis
As already mentioned, in the beginning of the interviews some participants expressed that they handled the CRC diagnosis surprisingly well and considered CRC a consequence of being old. When describing physical as well as psychological challenges such as sleep deprivation, anxiety or insecurity regarding their recovery, they seemed to downplay them by minimizing the experience. One participant expressed ‘I asked for sleep medication because I do not sleep well … I get thoughts, I think about having had cancer, am I more inclined to get it again? … But it does not bother me, no, no way’ (P2). The participants stated that everything was fine, there was little they could not deal with and some instead focused on the positive aspects of the challenging situation. A few participants avoided talking with others about the cancer, altered bowel movements or physical problems in their pelvic area. Others described avoiding thinking about the cancer and recovery altogether. By ending a statement with a small laugh, they downplayed what they had just said by reducing the impact of the burdens experienced, like the following participant ‘The cancer operation itself was terribly painful (laughter)’ (P11). Some described having accepted the situation and were prepared for unavoidable discomfort after surgery as one participant stated ‘I do not have any pain, of course you can feel it from time to time, it is unavoidable, but not more than you can expect when people cut into you’ (P1). Several had experience of cancer due to a previous cancer diagnosis themselves or for their acquaintances. This personal experience with cancer was described as reducing the likelihood of being overwhelmed by the diagnosis: I have had cancer myself and my husband died of it, so I am familiar with it. When I got breast cancer just three years after my husband died, I thought it was a bit much … Had I not been familiar with cancer … I might have lost my balance … (P7)
CRC and treatment-related problems
As the interviews proceeded, the participants provided more detailed descriptions of the problems they experienced such as pain, fatigue, altered bowel function, decline in physical functioning, decreased appetite, urinary retention and infections. There were variations in how the severity of the problems affected each individual’s recovery. For some, the problems were an afterthought articulated in a fact-based manner, while for others they permeated the interviews and were expressed emotionally, but with hope of improvement. Those participants who underwent additional treatment such as neoadjuvant radiation or multiple surgery experienced the most complications and naturally described more challenges in recovery. A participant illustrated in a resigned manner how fatigue limited the activities of daily living: I just do not have the energy. I have enough problems just walking up the stairs to the second floor. I practically have to use the banisters to pull myself up … I cannot do anything like before … (P8)
Social network and healthcare services ameliorate transition from hospital to home
The need for support varied between the participants and changed during their recovery process. Social networks and healthcare services were important resources for managing daily life and challenges after CRC surgery. A short stay in a nursing home or family members staying with them when they returned home from the hospital provided necessary safety and predictability, something that is important for older persons going through major life changes. One participant described how she required a nursing home stay to give her the support she needed to feel safe after hospital discharge: The second day after the surgery they came and asked me if I had thought about going home. ‘No’ I said, ‘I will not go home before I get a place at [name of nursing home]’. That is what I said … I felt safe where I was. I did not have the courage to live alone in my own house. (P7)
Stoma is an extra burden
Having a stoma increased the challenges the participants encountered after returning home. They described difficulties finding suitable equipment and all of them experienced leakage. Furthermore, reactions to the stoma varied from avoidance to acceptance. One participant described with disgust how she recently reacted to the stoma during stoma care ‘Then I saw the stoma and you know what, I almost vomited’ (P4). The need for stoma care from the homecare services varied from dependency to independence. In addition, they had to be creative in learning how to manage and find a ‘new normal’. Some described having to eat at specific times to prevent bowel movements when socializing and they had to spend most of their time at home to avoid embarrassing situations. One participant reported experiencing stoma leakage at night and used towels tucked around the stomach to contain the outflow ‘The towel takes the brunt (laughter) because I just fasten it lightly around [stomach]. They are old towels that I am not worried about and can easily throw away’ (P1). Due to the stoma one of the participants did not feel safe being away from the house for too long: That’s how I act now … I never go out without having (my stoma) cared for and emptied … I feel that when I’m clean and empty I can take an hour and then return home, because then I am safe. (P4)
Insufficient follow-up from the healthcare services after CRC surgery
This theme presents the experiences of several participants who suddenly became responsible for their own follow-up care after having been discharged from the hospital shortly after surgery. There was a feeling of disconnectedness from the healthcare system, where their social network often had to bridge the gap. This theme consisted of the following sub-themes: Lack of information can make it more complicated to take care of oneself, The strain of follow-up care and Lack of continuity of care.
Lack of information can make it more complicated to take care of oneself
Lack of information was a continuous problem and led to worries and unanswered questions regarding, for example, nutritional issues and stoma care. One participant recounted the difference between the expectation based on a presurgical information letter from the hospital and the reality: ‘It was not what was promised in the letter I received that I was going to get some [stoma] education and learn to wash and care for it’ (P11). This lack of information culminated in the participants having to find things out for themselves, resulting in poor compliance with new medication and nutritional regimens, and distressing circumstances around stoma care. One participant received contradictory information that could have led to complications such as the development of a hernia or wound rupture and having to endure prolonged correctional treatment: I asked the nurses (homecare services) – Do you think I can start exercising again? – Yes, of course you can. Then I thought that I should ask the doctor and it turned out that this was wrong. I should take it easy, I am not even allowed to lift a grocery bag. (P4)
The strain of follow-up care
The participants had to take responsibility for all follow-up requirements. One participant explained how she had to make an appointment in her general practitioner’s (GP) office to get a blood test done, which had to be coordinated with the time of her consultation at the hospital: ‘I was at the GP’s office. I only saw the nurse; she was to take a blood sample to send to the hospital so that they would have the result by my follow-up appointment …’ (P1). This entailed organizing and coordinating various follow-up appointments and the logistics involved. Some participants described doing this without modern technology such as apps, the internet or phones, which made access to the healthcare service more complicated. Several participants mentioned seeking medical advice from healthcare personnel outside their healthcare service who they perceived as more accessible. One participant described how she, while worried about her surgical wound, contacted other persons instead of going to the GP because it was hard to get an appointment and because of the time delay before receiving the necessary medical aid: I asked if she [husband’s homecare nurse] could take a look at the [surgical] wound and tell me what she thought. Having to walk to the GP’s office to arrange a consultation and then having to walk back again for the appointment 14 days later, I only wanted them to look. I did not expect them to do anything about it, I just wanted them to check that it was all right. (P10)
Lack of continuity of care
When returning home from hospital some of the participants received assistance from multiple homecare services personnel who were often under time pressure. One participant narrated an experience with a member of the homecare staff that she had appreciated because he took the time to talk to her and make her feel safe: ‘He gave me so much, I felt safe and it means a lot. The others are very kind but they have so little time …’ (P4). In addition, several participants were appointed a new GP, before or during the trajectory of cancer treatment. This resulted in an often-unfamiliar GP at a time when their GP was supposed to be the link between the patient and necessary healthcare services. Only a few had consulted their GP within the month after surgery, with appointments often initiated by the hospital. During one interview, a participant wondered why GPs were involved at all: … Sometimes one thinks to oneself that one could just as well go straight to the hospital … why the GP? I wonder, because I do not talk to her [GP] myself. (P4)
Discussion
The aim of this study was to explore the experiences of individuals aged ≥80 years recovering from surgery for CRC and possible challenges they may encounter after discharge from hospital. As previously mentioned, the participants started the interviews by describing how well they had managed, but during the course of the interviews the challenges became more obvious. Our findings suggest that older individuals treated for CRC varied in their perception of how they managed everyday life after discharge from the hospital. These findings are in accordance with a previous study on coping with the psychological stress of a cancer diagnosis that showed that older people are less psychologically affected by the diagnosis than younger people. 23 However, the study did not discuss the mechanisms behind those findings. The findings in the present study revealed that having the perspective that illness naturally accompanies old age, as well as experiences with cancer, reduced their concern. Our findings were in contrast to a study on older breast cancer patients, where experiences of cancer in others left the participants in fear of recurrence, disfigurement and side effects. 24 In his psychosocial developmental theory, Erikson 25 describes that during a lifetime people experience various life phases dominated by different challenges. In late adulthood people start to experience growing old, characterized by different forms of deterioration. In addition, they encounter personal losses and are faced with the reality of an unavoidable death. Our impression was that the participants’ advanced age, long life experience and knowledge influenced their perceptions. In our study, the participants’ descriptions of problems and complications were mostly physical. However, some psychological and social challenges were expressed, although the participants stated that they had not consulted family or healthcare personnel about these worries and insecurities. Jorgensen et al. 18 suggest that physical complications could be a manifestation of underreported psychological problems due to the participants’ attitudes towards ‘unmentionable’ issues. The participants in our study downplayed the challenges they faced by laughing after mentioning them. This can be understood as a coping strategy or buffer to downplay difficult topics or to avoid becoming a burden19,20,26 and the coping mechanism has been reported in relation to cancer diagnosis in other studies. 27
In the present study, some participants expressed feelings of insecurity regarding what to expect in terms of symptoms when they returned home. Their lack of information and knowledge could hinder their ability to manage self-care, despite being in a situation where it was expected that they assume responsibility for their own health. 28 Receiving written or verbal information is insufficient if the recipients do not understand it and are left uncertain and insecure. 13 The need for information might differ between younger and older CRC patients because of their different perspectives and knowledge regarding cancer and its treatment. 29 A way of giving them a sense of control is to include them in the discharge planning process. 21 However, no such collaboration was described in our findings, nor in another (Norwegian) study by Dyrstad et al. who studied older patients’ participation in admission and discharge from hospital. 30 After discharge the GP is responsible for assisting patients with their follow-up. However, only a few of the participants in our study had consulted their GP after discharge. A previous study found that GPs were more involved in the diagnostic process and less in follow-up. 19 When challenges did occur, patients reported uncertainty about whom to contact in the primary or specialist healthcare service. Additionally, GPs and other healthcare personnel in the primary healthcare service lacked experience of CRC.13,19 To meet the demand for a holistic approach to ensure continuity of care, a specialist nurse-led model for follow-up care was reported to be useful, as nurses are more accessible and have considerable knowledge about living with CRC. 31
The participants in this study experienced various complications. The recovery period was short and uncomplicated for some, while others had to overcome several challenges. A plausible reason for this variation could be that the surgical complications and recovery are dependent on the actual tumour location. 32 We found that the older participants who had a stoma due to the cancer treatment experienced different problems and one can question whether patients with colon and rectal cancer should be studied separately. Research on CRC survivors shows that complications occur, but our study of older persons treated for CRC revealed a more comprehensive set of complications. 33 However, it must be taken into account that older people’s complex health condition entails a higher risk of complications after discharge compared to their younger counterparts. 34 Another possible reason for the variation in our study is that there may be a greater difference in physical and psychological functioning among older patients that increases the risk of surgical complications. Several studies have confirmed that frail older people treated for CRC are especially vulnerable.8,35–37 However, this study found that family was a particularly important resource for managing recovery and vulnerability. The support and care provided by family members was repeatedly described throughout the findings due to their important role after discharge from hospital. Our findings suggest that support from social networks and public services ranged from occasional practical help with everyday tasks to more medically related issues such as stoma care and continuous assistance with the activities of daily living. Although assistance from one’s social network can be a necessity at all ages,38–40 older persons’ need for a social network as a source of security seems to surpass that of their younger counterparts. In our study, these issues were often taken care of by family members but also friends and healthcare personnel. However, Dyrstad et al. 30 found there was no routine for involving older patients’ next of kin in the discharge decision-making and family members were not mentioned in the discharge process. Important relatives were often involved at the last minute and received inadequate information, despite the fact that they had to assume a great deal of responsibility after discharge. 40
Methodological considerations
A methodological strength of this study is the possibility to explore in depth the experience of recovery and possible challenges faced by older people treated for CRC. However, this approach cannot be generalized to all older people treated for CRC. The sample was selected for maximum variation, but we have probably not included the most troubled individuals. Furthermore, the sample consisted of ten participants, which can be considered small. However, the interviews were rich with data, and saturation was believed to be achieved. A further strength of the study was that the researchers endeavoured to ensure trustworthy data by having the first author conduct the data collection to minimize the risk of inconsistency. Additionally, the authors conducted the analysis as a research team and critically discussed each step in the analysis process. Team meetings were held to discuss the generated codes and the content of each theme and sub-theme was rearranged throughout the analysis process. In this process, the authors provided various interpretations of the analysis to ensure the credibility of the results. Quantitative longitudinal studies with a larger sample size should be performed to further explore the symptom burden, coping ability and perceived social support experienced by older people during their recovery from CRC surgery to better determine the need for improved follow-up care.
Conclusion
This study of people aged ≥80 years who underwent curative resections for CRC shows that when they return home they cope remarkably well considering the challenges they face. However, the findings suggest that they downplay their needs and burdens. Healthcare personnel must be aware of this when interacting with this group of patients. Our study indicates that older patients often need help from their social networks for their aftercare and that GPs are scarcely involved. There is a need for recognition of the fact that older individuals treated for CRC constitute a unique group whose current follow-up care from the primary healthcare services seemingly does not address their care needs.
Supplemental Material
sj-pdf-1-njn-10.1177_2057158521994451 - Supplemental material for Experiences of recovery from colorectal cancer surgery after hospital discharge among the oldest old: A qualitative study
Supplemental material, sj-pdf-1-njn-10.1177_2057158521994451 for Experiences of recovery from colorectal cancer surgery after hospital discharge among the oldest old: A qualitative study by Kristina Sundt Eriksen, Sissel Iren Eikeland Husebø, Hartwig Kørner and Kirsten Lode in Nordic Journal of Nursing Research
Supplemental Material
sj-pdf-2-njn-10.1177_2057158521994451 - Supplemental material for Experiences of recovery from colorectal cancer surgery after hospital discharge among the oldest old: A qualitative study
Supplemental material, sj-pdf-2-njn-10.1177_2057158521994451 for Experiences of recovery from colorectal cancer surgery after hospital discharge among the oldest old: A qualitative study by Kristina Sundt Eriksen, Sissel Iren Eikeland Husebø, Hartwig Kørner and Kirsten Lode in Nordic Journal of Nursing Research
Footnotes
Author contributions
Study design: KSE, SIEH, HK, KL; data collection: KSE; data analysis: KSE, SIEH, KL and manuscript preparation: KSE, SIEH, HK, KL.
Acknowledgements
The authors would like to convey their gratitude to the participants for telling their stories.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.