
Abstract
Radiotherapy of pelvic cancers may cause severe tissue injuries, and hyperbaric oxygen therapy (HBOT) is one of few treatment alternatives. As part of a longitudinal, mixed-methods study, this study’s aim was to explore pelvic cancer survivors’ experiences of undergoing such treatment. Using a phenomenological-hermeneutical design, in-depth interviews of 20 cancer survivors were conducted and analysed using systematic text condensation. This study is reported in accordance with COREQ. The informants’ experiences were identified as: Approaching an unknown world, From feeling worried to becoming familiar, A long-lasting treatment course, and The treatment course went better than expected. Despite information prior to the treatment, informants were worried about HBOT but were still motivated to try it. A combination of relevant information, clear routines, person-centred care, peer support, and limited side effects seem to be important factors for patients’ experiences of safety from this treatment.
Introduction
Irradiation is an essential part of the curative treatment of pelvic malignancies, including gynaecological, prostate, and rectal cancers. 1 However, radiation may affect the surrounding healthy tissues and lead to acute or chronic injuries, and 5–15% of patients develop late radiation tissue injuries (LRTIs) months or years after radiation.2,3 These injuries are characterised by poor microcirculation, hypoxia, tissue damage, and fibrosis,3–6 causing symptoms such as increased frequency, urgency, and leakage of urine and faeces, diarrhoea, and pain, which diminish the individual’s quality of life.7–11 Treatment options are limited, but hyperbaric oxygen treatment (HBOT) has shown promising effects in treating pelvic LRTI.1,2,12–14 The aim of this treatment is to increase tissue oxygen concentrations and stimulate neoangogenesis and cellular regeneration, thereby revitalising and healing the hypoxic tissue and alleviating the symptom burden.6,15
Hyperbaric oxygen treatment is a high-technology treatment where patients are enclosed in a pressurised chamber and breath pure oxygen at a pressure of 2 atmospheres absolute or more for 90–100 minutes once a day for 6–8 weeks. 1 Strict safety routines are applied because the ambient oxygen level increases the risk of fire and oxygen seizures. 16 Consequently, HBOT requires specific technical competence and constant and close observation of the patients during the treatment, and this is commonly provided by specialised trained nurses.
Physical side effects of HBOT are usually mild and temporary (e.g. barotrauma and visual changes). 16 Because HBOT is only administrated at relatively few specialised centres, most patients and healthcare professionals are unfamiliar with this treatment. The technical environment, the confining and uncomfortable space inside the chambers, and the exposure to noise and changing temperatures may induce or increase distress, anxiety, and claustrophobia and lead to termination or refusal of treatment. 17
In addition, patients with pelvic LRTI often have substantial and complex symptoms in one or multiple organs (e.g. bladder, bowel, rectum, and genitalia),2–5,10 and this may create concerns when enclosed in the chamber for two hours daily. The nurse’s ability to provide person-centred care based on the individual patient’s needs combined with their technical competence are of crucial importance to minimise the negative impacts of the treatment. 18 However, despite the patients’ multiple challenges, no prior research that has explored how patients with pelvic LRTIs experience undergoing HBOT were identified. This is important knowledge to guide nurses in how to prepare patients for the treatment, to alleviate anxiety and distress, to meet the patients’ needs, and to promote trust and coping ability throughout the treatment trajectory. This study therefore aimed to explore how cancer survivors with pelvic LRTIs experience undergoing HBOT.
Methods
The study was performed in line with the Consolidated Criteria for Reporting Qualitative Research checklist. 19 It was anchored in qualitative methods, using a phenomenological-hermeneutical approach. 20 This approach permits in-depth insights into individuals’ experiences of a topic and provides an understanding of the essential meaning of individuals’ lived experiences of a phenomenon, in this case the patients’ experience of undergoing HBOT. 20 The researchers act as an instrument in a process in which the individuals’ life-world experiences are transcribed into text (phenomenological) and subsequently interpreted (hermeneutical). This leads to a back-and-forth process between the informants’ expressed experiences and letting the phenomenon speak for itself and the researchers’ open-minded and dwelling approach with close awareness of their own preunderstanding and interpretation. This process, also referred to as the hermeneutic circle, generates new insights and understandings about a phenomenon.20,21
Recruitment and participants
This study is part of a longitudinal mixed-methods study of patients with pelvic LRTI undergoing HBOT in monoplace hyperbaric chambers at the Norwegian national centre for HBOT (trial registration: ClinicalTrials.gov. NCT03570229). Participants in the current study were recruited through purposive sampling 20 from the main study, for which the eligibility criteria were a) pelvic LRTI after intended curative radiation for pelvic cancer (prostate, gynaecological, urological, or bowel cancer), b) symptoms of radiation injury of the bowels, bladder or pelvic bones, objectively verified by endoscopy or radiology; c) ≥ 6 months from completing radiation; d) referred to The Norwegian National Unit for Planned Hyperbaric Oxygen Treatment; and e) age ≥ 18 years. Eligible participants were consecutively contacted by a study nurse who gave them written and verbal information about the study. Recruitment was continued until a sample of 20 participants was obtained. The sample reflected a broad variety of demographic and medical backgrounds as required for qualitative research. 20 The participants, 11 women and nine men with different civil status, were between 36 and 77 years of age when interviewed. They had been diagnosed with different pelvic cancers, had undergone pelvic radiation, and had developed different LRTIs (radiation cystitis and proctitis and osteoradionecrosis).
Data collection
To capture the lived experiences of undergoing HBOT, in-depth, individual, face-to-face interviews were conducted at the end of six weeks of HBOT between January and November 2019. The first and third authors performed the interviews in an office free from any disturbance at the HBOT location. The authors had not met any of the informants before the interviews. Before starting the interview, the interviewers introduced themselves and reminded participants of the purpose of the study and the interview, the voluntary nature of participation and their right to withdraw, protection of anonymity, permission to audiotape the interview, and the interviewers’ status as researchers outside the HBOT centre, and they encouraged the participants to speak freely. To ensure that the two authors conducted the interviews in a reasonably similar manner, a brief interview guide with the information outlined above along with some broad topics (e.g. experiences related to information, procedures, follow-up) was developed, pilot-tested, and used without any revisions. 22 All interviews started with the opening question: ‘Can you please describe how you have experienced undergoing HBOT’? The informants were encouraged to tell their own stories as freely as possible, and their stories led to new follow-up questions. The context allowed for an exploration of the individual participants’ experiences where they could direct the course of the interview and identify and describe experiences that were not considered by the researchers. Each interview was audiotaped and lasted approximately one hour. After each interview, the informants had the opportunity to respond to the interview itself. Here, many found it positive to tell ‘the whole story’ to an interested listener, whereby some expressed that the interview clarified what they had gone through. After each interview, the two interviewers discussed their immediate reflections on special themes or nuances or important clues to be followed up on in forthcoming interviews. Data saturation was accomplished around the 15th interview, but we continued up to 20 interviews to make sure that no new topics emerged. 23 The interviews were transcribed verbatim, concealing any identifiable variables, and a pseudonym was given to each participant. 20 Transcripts were not returned to the participants for comments.
Data analysis
The analysis was performed in collaboration by all authors, emphasising the importance of working both systematically and creatively to capture the essence of the informants’ experiences. Here, systematic text condensation was considered an appropriate method because it represents a descriptive and explorative method for thematic cross-case analysis, and is well suited for capturing informants’ lived experiences. 24 This four-step analysis starts with interviewing and then moves into analytic circles, aligning to the study’s phenomenological–hermeneutical approach. 20 First, all authors read the interviews separately to obtain a general overview related to the study aim and then discussed their impressions until consensus was reached. Second, the interviews were re-read, and eight representative units of meaning were extracted. The units of meaning were transferred into NVivo12 software for further coding and sorting of the data (www.qsrinternational.com). All interviews were again re-read and coded in relation to the units of meaning. Third, the coded units of meaning were condensed into abstracted themes, engaging the researchers in an analytic circle between the identified themes, transcribed interviews, and discussions. At the conclusion of this process, four themes were agreed on, each having two subthemes. The analyses were discussed among the authors until all interpretations reached consensus.20,24 With backgrounds in cancer care and qualitative research and experiences as a specialised HBOT trained nurse and a senior neurologist/HBOT physician, the authors’ preconceptions of the topic were made explicit and were critically discussed during the research process. 24 To validate the analysis, the fourth step entailed comparing the findings with the transcribed interviews in order to ensure that we had captured the informants’ expressed and intended meanings (Table 1). The findings were also unanimously validated by the study’s advisory board, consisting of user representatives and healthcare providers with and without experience in HBOT.
The analysis process based on systematic text condensation.
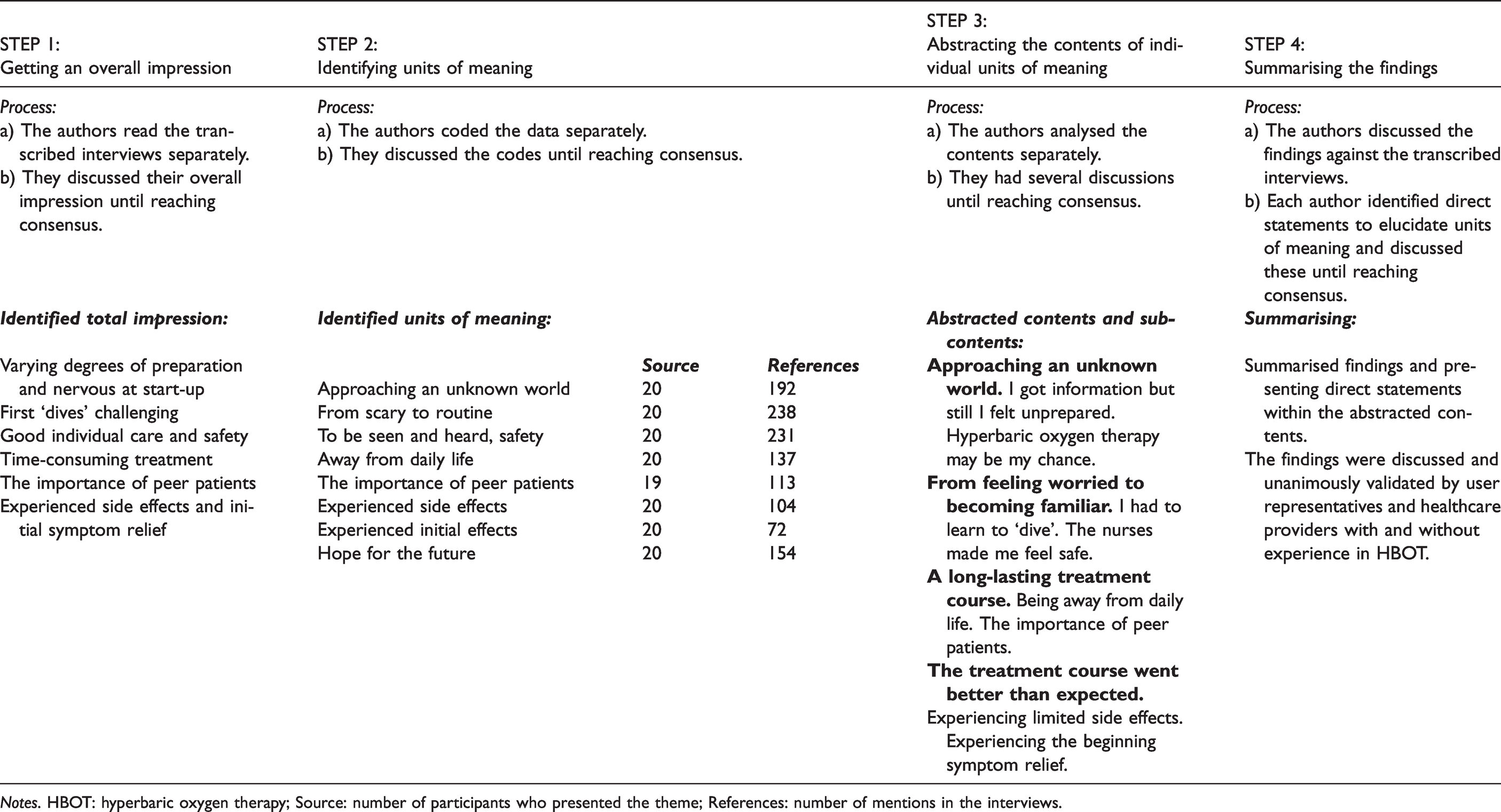
Notes. HBOT: hyperbaric oxygen therapy; Source: number of participants who presented the theme; References: number of mentions in the interviews.
Ethical considerations
Data in the present study were collected as an initial part of the longitudinal mixed methods study Hyperbaric Oxygenation Treatment and Quality of Life, approved by the Norwegian Regional Committee of Research and Ethics (2018/706) and registered at ClinicalTrials.gov (NCT03570229). The study was carried out in line with the Declaration of Helsinki 25 and in compliance with the General Data Protection Regulation (GDPR). 26 All informants agreed to participate voluntarily and gave written consent.
Findings
Four main themes emerged from the analysis of the participants’ experiences of undergoing HBOT: a) Approaching an unknown world, b) From feeling worried to becoming familiar, c) A long-lasting treatment course, and d) The treatment course went better than expected.
Approaching an unknown world
Most participants reported that they knew very little of what to expect when arriving at the HBOT unit. They felt that they had entered a totally unknown and somewhat scary environment that was difficult to imagine prior to arriving at the treatment centre. The analysis showed that there were several facets underpinning this experience.
An important part of this experience was elaborated as ‘I got information but I still felt unprepared’. There was considerable variation in how participants initially had been informed about HBOT as a treatment option for their LRTI symptoms. Most were informed about this option by a physician, but some had introduced this possibility themselves to their general practitioner because they had seen a programme about HBOT on TV or had been recommended to try it by others. Despite these variations, a common experience was that they had received very little information about HBOT from the referring physician. However, all reported that they had received written information about the treatment procedures from the HBOT unit prior to the treatment. Nevertheless, the participants still found it difficult to understand what it really was to undergo HBOT and felt insecure and unprepared for what to expect: I got just a little information (…) I was really tense when I started, because I didn’t know what I should expect (…) when I first came here, I thought they were going to immerse me in water. (Maria)
Another important part of the informants’ experiences of entering an unknown world was identified as ‘HBOT may be my chance’. Even if HBOT was highly unknown and unfamiliar to them, the informants expressed that they were very eager to start the treatment. Prior to treatment, they described vast physical, emotional, and social implications of living with pelvic LRTI over time with limited treatment options. Consequently, they experienced that HBOT was a golden opportunity to finally ease their symptoms. Even if the informants experienced a common hope that the HBOT would decrease their LRTI symptoms, they were very realistic and welcomed any improvement – as illustrated by Julia: I hope this can alleviate some of the pain and nausea (…) Just a few per cent improvement would be better than it is now.
From feeling worried to becoming familiar
The informants described entering the HBOT unit with worries and about how different it was from earlier treatment experiences. In particular, they experienced the high focus on security, precautions, and technical equipment as being unfamiliar and unexpected. Gradually, the informants’ experiences went from feeling worry, towards HBOT becoming a familiar routine.
An essential part of this experience can be summed up as ‘I had to learn to “dive”’. Here, the informants expressed that they had to learn and understand the safety procedures, that they had to wear suitable clothes, that they could not use any ointments, and that they had to go through safety checks before being allowed to enter the chamber. However, they expressed that the nurses’ information about what was going to happen when inside the pressure chamber, how to manage challenges, for example, inner ear equalisation problems, were important in making them feel secure. Still, a common experience related to the first treatment sessions was initial problems with their ears, as expressed by Sarah: I wasn’t prepared that I had to work that hard to equalise the pressure in my ears, I thought I could just relax (…). At first it was scary, because I didn’t know what it was when I got pain in both my ears, it felt like my eardrum was going to burst. The nurse showed me how I could equalise the pressure by holding my nose and swallowing (…). I had to use this technique the first week (…), but now I can equalise just by swallowing, so it goes really well.
Another important facet of the informants’ experiences from being worried to becoming familiar with the treatment was identified as ‘The nurses made me feel safe’. Here, the informants described how the nurses handled their individual needs and arrangements in a caring and reassuring way, as illustrated by Anna: I have a lot of pain in the pelvic area and cramps over my bladder (…) the nurses noticed that, and they solved this issue by piling up pillows under my hips, and they took great care for me to be comfortable (…) I experienced that being in the pressure chamber went surprisingly well.
A long-lasting treatment course
Overall, the informants experienced that the HBOT was a lengthy and time-consuming process because most of them had to stay at the hospital’s patient hotel for the six weeks of treatment because the centre was so far from their homes. This experience had two main facets.
In ‘Being away from daily life’, the informants experienced that the daily treatments and their absence from home greatly affected their everyday life, and they found it difficult to be away from their spouses, families, friends, and pets. Participants who were caring for underage children, especially single parents, experienced concerns and challenges related to childcare and follow-up. Although the informants could travel home every weekend, a common experience was that these journeys were too exhausting or there were concerns related to their symptoms, as illustrated by Joe: I had planned to go home a couple of weekends during the treatment period (…) but I didn’t dare because I was afraid, I would start bleeding from the urinary tract during the trip (…) now I haven’t seen my wife for six weeks (…) it would have been hard without the telephone. It was first when I came here and met the others that I realized I actually have radiation injuries (…) I’m not the only one who has such damage (…) it is a relief to meet others in the same situation and to share experiences.
The treatment course went better than expected
Overall, the informants expressed that even if the treatment course was experienced as lengthy, it went far better than they had expected it to in advance. This experience was based on two main features, identified as ‘Experiencing limited side effects’ and ‘Experiencing the beginning of symptom relief’.
The first facet of the positive experience of the treatment course was that the informants experienced limited side effects of the HBOT. Most common was barotrauma, whereby most handled this by learning how to equalise the inner ear pressure just by swallowing. A few informants needed treatment with nasal spray or tablets, and one needed a surgical intervention with paracenteses.
Several informants experienced significant fatigue both during and between the treatment sessions, and this was especially significant for informants already diagnosed with fatigue: I have fatigue and it is just as it became worse (…), I don’t remember which day it is, I don’t remember if I have talked to those at home today (…) it’ll be tough when I get home again. (Susan)
Although all informants experienced some side effects, these were commonly expressed as tolerable. However, those who experienced adverse events stated that they were quickly seen by a HBOT physician for diagnosis and management.
The second facet of the positive experience was that the informants articulated that they experienced an improvement of their pelvic LRTI symptoms during the treatment course, outlined as pain relief and less bleedings, as well as less urge and frequency of urine and faeces and consequently fewer toilet visits during both the day and night, as illustrated by Eric: The last nights I have only been up once or twice (…) that’s a record (…) usually, I’m up to the toilet at least ten times a night.
Discussion
Although HBOT is an approved indication for several conditions, for example, LRTI, it is not widely established or studied, and it is relatively unknown among both healthcare professionals and patients.1,27 To our knowledge, this is the first study focusing on patients’ experiences of undergoing HBOT. The findings illuminate important aspects of the patients’ own experiences that may provide nurses with important understanding and knowledge in caring for patients undergoing HBOT and other high-technology treatments.
First, the findings showed that even if the patients got information about HBOT and the routines before entering the unit, they experienced mixed feelings of distress and hope. In line with our findings, previous research shows that entering a high-technology treatment may increase the level of distress and anxiety. 28 Because information and knowledge have been documented to be important in decreasing treatment-related distress, 29 our findings highlight the importance of increasing knowledge of HBOT among healthcare professionals in preparing patients for such treatment. However, even though our participants received written information and a link to a video, they still found it difficult to comprehend what HBOT was like in advance. Comparable to our findings, patients with other conditions have described HBOT as ‘a new world’ and call for more information to be provided in advance.30,31 To alleviate distress, in addition to the written information, a phone call from the HBOT unit before attendance may be helpful where patients can air their concerns and clear up remaining questions and misunderstandings. Furthermore, it is important that nurses at the unit are aware of the patient’s level of distress when entering the unit, let them know that this is normal, address the patient’s individual needs, and repeat the information. 28 Even though feeling distressed and anxious, the patients were very motivated and hopeful regarding the treatment. This is an important resource in treatment because hope and outcome expectations play a predominant role in mediating distress and promoting health-related quality of life.7,27
Second, our findings showed that although the patients experienced initial distress and anxiety, they became accustomed to the HBOT after a few sessions. Building on previous research,28–30,32 the combination of psychoeducation, entertainment distraction, and the close follow-up from the nurses seem to be important factors in making the patients feel comfortable and safe. Patients have previously reported discomfort related to the chamber environment30,31 but this was not supported by our informants. This may be due to the use of monochambers in this study, as well as our informants’ indications of the nurses’ ability to make individual arrangements, e.g. with additional pillows, thus making the patients feel as comfortable as possible. An important finding is that the patients’ high symptom burden and concerns related to urgency and leakage of urine and faeces only appeared to be a minor problem. This may be explained by consistent information, clear routines, daily contact with specialised nurses, and the nurses’ constant follow-up and responding to the patients’ individual needs, which are known to be important factors for acceptance and coping during HBOT.30,31,33 Another important factor seems to be that that the patients found relief in distraction, such as watching a movie during treatment. This aligns with earlier findings that patients who are distracted by entertainment during treatment show less anxiety. 29 The development of a trustful relationship, meeting individual needs, and mastering ‘learning by doing’ seem to have facilitated the patients’ coping abilities and a feeling of safety. These findings highlight the importance of predictability and patient-centred care as being essential for positive coping experiences, in addition to specific professional nursing competence as a safeguard for patients in a HBOT environment.
Third, the findings showed that even if the patients experienced the treatment course as long lasting and did not enjoy being away from their everyday lives and loved ones, the absence from home and social relations was acceptable. An important reason for this was the opportunity for patients to socialise, share symptom burdens, and support each other. In Norway, rehabilitation is not an integrated part of the cancer treatment trajectory. Research has shown that patients often feel left alone with their latent affects and cancer-related challenges, and in addition to professional follow-up they often request peer support.34,35 It seems that the opportunity for the informants to share time with other patients with similar challenges allowed for a unique community to develop, and this to a certain degree compensated for being away from family and friends. Peer support is shown to be important for promoting positive changes and improving psychosocial function, empowerment, and quality of life. 36 Consequently, nurses should facilitate and promote peer support as an important part of the treatment course.
Fourth, the findings indicated that the majority of participants had only minor, temporary, and highly tolerable side effects of HBOT, such as mild barotrauma, visual changes, tiredness, and claustrophobia. Most of these are well known and temporary. 16 However, a new finding not previously documented was that most patients reported high levels of fatigue, both during and after treatment. This may be another aspect of oxygen toxicity, and pre-existing fatigue after cancer treatment may be a predisposing factor. More attention and research should be directed to this issue. No participants dropped out, and only one needed anxiolytic medication for more than a few days. In contrast, a study by London et al. 37 reported that nearly one third of patients treated in monoplace chambers required sedative premedication due to claustrophobia. This may again be explained by the specialised nurses’ knowledge of the side effects of HBOT and their ability to perform the high technology treatment procedures while at the same time attending to the patients’ individual needs and thereby preventing serious side effects. An interesting finding is that most participants described initial symptom relief during the treatment course, while symptom effects often do not occur until several weeks after completing an HBOT session. 14 Although a placebo effect cannot be excluded, participants reported rather specific and objective symptom relief, such as fewer toilet visits, which may indicate structural improvement. This beginning of symptom relief promoted the informants’ hope for further symptom relief even if they were very realistic and expressed that they appreciated any improvements of their symptom burden, no matter how small. Experiencing initial symptom relief, having hope, and positive outcome expectancy for further improvements have been shown to be important factors for cancer survivors’ coping and health-related quality of life.7,38,39 This has also been documented in patients undergoing elective HBOT for other conditions, for example, osteoradionecrosis of the head and neck or diabetic foot ulcers.31,33
Strengths and limitations
This study has several strengths. It is the first study that provides insights into how cancer survivors with pelvic LRTIs experience the HBOT trajectory. Another significant strength is the enrolment of a diverse sample from across the country, with varying backgrounds, cancer diagnoses, pelvic LRTI injuries, gender, and age. Furthermore, data saturation, defined as no new lived experiences being outlined, 23 was achieved in the interviews. The study’s analysis process was transparent, performed and validated by all authors, discussed in relation to the authors’ preunderstandings, and validated by illustrative quotations. The elaborated themes were consistent, suggesting that we captured a valid sample of the participants’ lived experiences, thus making the findings valid and transferable to other LRTI patients.20,24 However, the qualitative design and the single-centre approach limit the generalisability of the findings. 20 Furthermore, the sample did not include participants refusing HBOT or study participation, meaning that we captured a sample that was highly motivated for HBOT and positive towards our research. Because we only included participants treated in monoplace chambers, the patients’ experiences may differ in some aspects from treatment in multiplace chambers.
Conclusion
Starting HBOT was experienced as Approaching an unknown world for many patients, and detailed information was needed to prevent distress and anxiety. Clear routines, highly specialised personnel with a reassuring attitude, person-centred care, and distraction during treatment seemed to be important factors to make the patients feel safe and to promote their coping abilities during treatment. The downside of the HBOT course being long seemed to be outweighed by the benefits of meeting peer patients. Overall, HBOT was experienced as a safe treatment with limited side effects, where many patients noticed a beginning of symptom relief. Our findings indicate that HBOT is feasible for patients with pelvic LRTI. More research within this field is warranted, especially longitudinal studies of the development of pelvic symptom burden, late side effects from radiation, and quality of life.
Trial registration
This study is part of a longitudinal mixed-methods study of cancer survivors with pelvic radiation injuries undergoing hyperbaric oxygen therapy and the main study was registered in ClinicalTrials.gov (NCT03570229).
Footnotes
Acknowledgements
The authors thank the study participants for sharing their profound experiences. Thanks to Hyperbaric Medicine Unit, Department of Occupational Medicine, Haukeland University Hospital and Center for Crisis Psychology, Faculty of Psychology, University of Bergen for making this study possible.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The Dam Foundation and the Norwegian Gynecological Cancer Society generously supported the research (Grant number 2019/FO244488).