
Abstract
Hospital nursing shortage is a global problem caused by nurse dissatisfaction with their manager, an extensive workload and a stressful work environment. The study aimed to investigate nurses’ experiences of practices in hospital departments with low nurse turnover rates in relation to culture, work environment, nursing competencies, and nurse management. A constructivist design using a positive deviance approach was used for this study. Four hospital departments with the lowest nurse turnover in the Zealand region of Denmark served as settings. Data were collected from 13 nurses through focus-group conversations and analysed using directed content analysis. The reporting adhered to the COREQ checklist. The three themes – collaborative fellowship, professional pride, and embracing management – revealed a sense of community between nurses and department managers. Even though the nurses’ daily practice was exhausting, they stayed in their positions due to the special culture in the departments, which brought the nurses closer together.
Introduction
The hospital nursing shortage is a global problem caused by nurse dissatisfaction with current positions1,2 or with their manager, 3 extensive workload and a stressful environment. 4 Nursing turnover has a negative effect on healthcare organizations, patients, and nurses. 1 However, human consequences, such as lower patient care quality and patient outcomes, poor continuity of care, as well as poor communication among healthcare providers, medication errors, decreased patient satisfaction, increased morbidity, and caregiver burnout are factors that have all been linked to high nursing turnover as well. 5
Numerous recruitment and retention strategies have been utilized to overcome the nursing shortage and prevent turnover,6,7 with most studies of effective nursing shortage management strategies focusing on offering a high-quality working environment.8,9 In a cross-sectional survey of 45 new graduate nurses, Lalonde and McGillis Hall 6 found a preceptorship programme provided the nurses with low feelings of role ambiguity, role conflict and turnover intent, and high job satisfaction, which prevented turnover intentions. Luzinski 7 found that the Magnet model can create an infrastructure that attracts and retains high-quality personnel through a high level of professionalism. Zamel and colleagues 3 found that stress and being unable to work in a preferred role were major factors influencing nurses’ decisions to leave, but that hospital nurses with co-worker support were more likely to stay. Low levels of job satisfaction are related not only to employee withdrawal and intention to leave but also to employee mental health and burnout. 10 Additionally, job satisfaction in nursing has been found to have a significant effect on patient satisfaction. 11
In Denmark, the highest nursing shortage is found in the Zealand region, where an effort to recruit and retain nurses is urgently needed due to the many vacant nursing positions across hospitals and departments. In order to address the nursing shortage, the Zealand regional council has begun to focus on the recruitment and retention of nurses through developing a strategic perspective and a larger multimethod study, Defining NUrsing CAPacity (NUCAP). Not all departments in the Zealand region are equally challenged despite covering the same broad clinical areas (medical, surgical, acute and psychiatric). Therefore, a positive deviance approach 12 was suggested in order to identify and learn from the departments with the lowest turnover rates in the local context. The literature reveals a wide variety of strategies to prevent nursing shortages, as well as a considerable number of important variables to consider to improve recruitment and retention of nurses and to prevent intentions to leave.6–8,10,11 The present study is a part of NUCAP and the study therefore aims to investigate nurses’ experiences of practices in hospital departments with low nurse turnover.
The research questions were as follows:
How do nurses experience the culture and work environment in their department? How do nurses experience practical nursing in their department? How do nurses experience the meaning, importance, or significance of nurse management?
Methods
Data were collected through four focus-group conversations with 13 nurses in four departments. Data were analysed using a direct content analysis to create a description of data based on predetermined themes in order to investigate certain areas of a problem. 13 The COREQ (COnsolidated criteria for REporting Qualitative research) checklist 14 was used for reporting methods and findings in this study.
Design
A constructivist design 13 was used to explore and gain a broad perspective on the three main research questions of the study. The constructivist paradigm builds upon a theory of how meaning is constructed through social relations and interactions. 15 Data were therefore collected through focus-group conversations to facilitate dynamic interactions between participants.
Theoretical perspective
Positive deviance is an approach that identifies groups or individuals whose behaviours or strategies permit them to find better solutions compared to their peers, despite comparable challenges.
12
This bottom-up approach reverses the common deficit-based approach that focuses on failures and harm, aiming to instead explore and recognize positive practices.
16
Different models of positive deviance have been suggested12,17,18 and all include the following three steps:
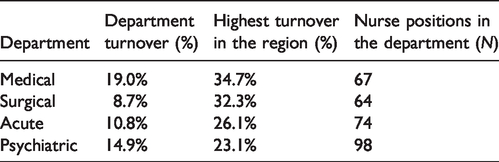
Define the departments. The four departments included in the study came from the medical, surgical, acute and psychiatric areas, as these represent the largest medical specialties and number of employed nurses. A total of 4399 nurses were employed at hospitals in the region, including 1950 in the four specialties. Characteristics of the four departments.
Discover positive deviant strategies using qualitative methods. Qualitative, in-depth knowledge is generated about the practices in the studied organizations 17 in order to generate hypotheses about why and how they perform differently.
Participants
Thirteen nurses in the four departments of acute, surgical, medical, and psychiatric care, participated in this study. They had on average been employed as nurses for 20 years (range 2–38 years) and had been employed in the department for an average of eight years (range 3–24 years). The recruitment process took place as follows: The department head nurses informed the nurses from the four departments about the possibility to participate and the nurses volunteered to participate based on their availability and interest. No references were given as to which and how many nurses declined the invitation.
Prior to the focus-group conversations, head nurses helped us to identify the nurse with the shortest time of employment in the department and the one with the longest for us to accompany for the day. Based on suggestions and recommendations from the lay and professional members of the NUCAP-project reference group and two pilot-group interviews with nurses, the two authors followed a nurse each in the department to get an impression of the setting and atmosphere in the department, prior to the focus groups. The two authors observed the same field, and performed reflective dialogues about what they observed, to provide a broad view and understanding of the field. 19 The observations were not included in the data for analysis; however, they were conducted in order to gain insight into nurses’ context and work atmosphere.
Data collection
Data were collected through four focus-group conversations with 13 nurses from the four hospital departments of acute (N = 3), surgical (N = 4), medical (N = 4), and psychiatric (N = 2) care. The nurses only participated in the focus-group conversations related to their own department. Both authors participated, as interviewer and moderator, respectively. The authors were both educated to PhD level and had no affiliations to the departments where data were collected. Through two pilot-group conversations, conducted in two specialized wards with very low turnover as of 2017, the interview guide was constructed based on the questions in the pilot study, aiming to specify the questions for the interview guide (Figure 1).
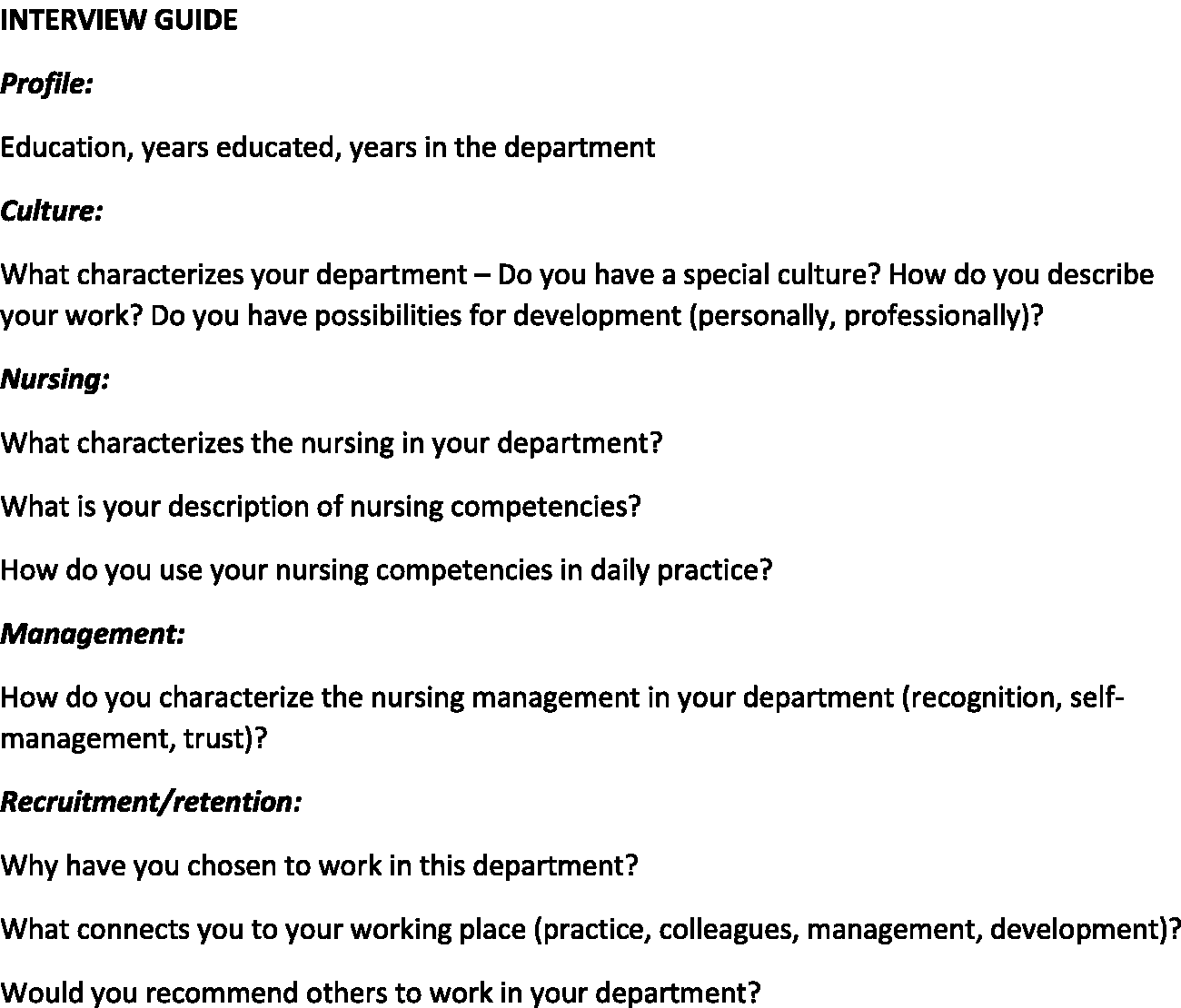
Interview guide for focus-group conversations.
The pilot conversations covered eight questions regarding the study aim and two questions about what we should ask the nurses to understand their recruitment and retention considerations. All focus-group conversations were audiotaped, transcribed verbatim, and lasted from 50 to 60 minutes. The interview guide was developed in Danish and translated into English for the purposes of this article, with both authors agreeing on the translations.
Data analysis
A directed content analysis 13 was used to analyse data from the four focus-group conversations. Directed content analysis creates a description of data based on predetermined themes in order to investigate certain areas of a problem. 13 Both authors carefully read and analysed the transcripts of the interviews. In the second read-through, both authors independently focused on the predetermined themes of the study: culture, work environment, nursing and nurse management. These results were discussed to reach a mutual understanding between the authors on the three themes: culture and work environment, nursing, and nurse management. Participant quotations are included below to support the analysis, not for equal distribution among the participants.
Ethical considerations
All participants were informed verbally and in writing about the authors, the study, their amount of participation, and their ethical and judicial rights to withdraw from the study at any time and for confidentiality, prior to data collection. All nurses who participated in interviews gave written consent and the nurses in the observations gave verbal consent. The study was approved by the Danish Data Protection Agency (REG-074-2018). Approval from the Ethical Committee was not applied for since no biomedical tests were conducted.
Findings
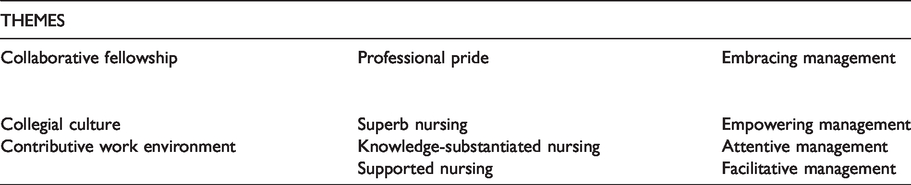
The main findings of the study revealed a sense of community between nurses and department managers. Nurses reported these close relations and the special culture in the departments as the reason they stayed in their positions and it brought the nurses closer together. The findings are presented as three themes: collaborative fellowship, professional pride, and embracing management, which are elaborated below through related sub-themes, and displayed in Table 2.
Themes and sub-themes in the study findings.
Collaborative fellowship
Nurses described working together and being part of a bigger unit when talking about culture and their work environment. The nurses reported that everyone, including all staff positions, with no exceptions, contributed collaboratively to create a great environment and feeling of community in the departments.
Collegial culture
When the nurses were asked if they could describe the culture of their department, the nurses defined their department as very special. Strong collegial bonds and personal connections to the workplace were important retention factors: I mean, retention of nurses? That is clearly our collegiality. I would dare to say so. We are, if you ask me, really good at helping each other. No one here feels overlooked. [Medical department] Yes, you do not feel like it is a finger-pointing culture. Not at all. ‘You should have …’ Or, ‘why didn’t you do this and that?’ It is an attitude thing, well, they probably did what they could. And that is nice. [Medical department]
Contributive work environment
The nurses did not differentiate between the meaning and the content of the concepts of culture and work environment. This became apparent when the nurses only addressed their psychosocial work environment and not the physical work environment in terms of physical strain or correct working positions.
The nurses agreed that the possibility to pursue further education and courses were important for their perception of a good work environment. The nurses described the gathering of knowledge on different levels to be developmental for themselves but also served the purpose of broadening their colleagues’ knowledge: There has been incredible development. With our own doctors, head medical staff and constant training in acute care, in trauma care, in treatment, in skill-stations, and this is offered to everyone. Something that is important here is that we all need to go through those phases. [Acute department] There is flexibility but there are also limits to how flexible it can be. Of course. So in that way I feel I’m being heard. And once in a while things might just not happen. Because the context is what it is. [Medical department]
Professional pride
The nurses described the quality of nursing they provided with distinction and showed a strong sense of professional pride in their nursing and in their competencies, supported by knowledgeable and helpful colleagues.
Superb nursing
The nurses described their practice as having a high degree of professionalism. They were openly proud of their nursing and claimed to have hired the most competent nurses out of the entire hospital. All the talented nurses from the entire place came to us because we have a great work environment. So we have almost depopulated all the medical and surgical department in this house. It is a natural thing that nurses go where it is great to be. [Acute department] I mean we have everything from the 19-year-old patients to patients with full physical support, and everything in between. So we use basic nursing every day. We also inform and guide in nutrition and health. [Medical department]
Knowledge-substantiated nursing
The nurses described how their nursing competencies substantiated knowledge gained from education, courses, and hospital clinical guidelines. They were constantly educated in specialist nursing competencies related to patient care through courses and skill stations, and when asked whether their courses are evidence-based, one participant replied: I think so – it’s developed in Boston, USA, and adapted to the Danish health system. We go through 15 skill-stations – incredible training. It’s a routine deal and everyone participates and learns tremendously. [Acute department] I mean all those nursing theories, right? There’s not even time for basic care. So I really don’t know when we are supposed to be able to use all those fancy theories, at any time. [Acute department]
Supported nursing
The nurses’ professional pride was supported by the comfort and strength of their nurse colleagues, and they described the importance of cooperation in managing daily patient care. The nurses knew their colleagues’ capabilities, directing them to get help from the nurse with the right competencies. It is such a security to know you can get the help you need. You can’t be 100% good at everything. If it’s not your core competency then you know you can walk out and find the nearest colleague who knows. We can always do that. [Acute department]
Embracing management
The concept of embracing management was two-sided, meaning that the nurses described that their leaders gave them a sense of being empowered and were attentive and caring towards the staff. In return, the nurses embraced the nurse leaders with strong loyalty and respect. The nurses primarily referred to the frontline ward manager and not the head nurse, who was regarded as distant.
Empowering management
The nurses described the nurse leaders as their frontline figures and as their protection from the outer world. It provided the nurses with a sense of security to know the nurse leader had their back in all matters. They support us without a doubt. You can count on your leader. And we have a feeling that they always defend our rights outside the department … There you have their complete support, no doubt about that. [Acute department]
Attentive management
The nurses had a positive experience of the nurse leaders’ active engagement in daily clinical work, presence in planning daily care, having lunch and coffee with the nurses, and talking to them about everything. They are present every day. If there were any problems, we told them and they took care of it [snaps fingers] immediately! And that means an incredible lot. It means everything. That means that you can trust your leader, you can talk to them about everything, not just work-related. [Acute department] They see it right away if someone is trying to hide. ‘You are a bit quiet today or something, right?’ … She’s just, really, so attentive. Oh, ‘you look so good, you get a hug today.’ It just the right approach to it. I’m gobsmacked. [Surgical department]
Facilitative management
The nurses described the nurse leaders’ attentiveness to the resources and potential of the nurses as important to balance their private and working life and experienced them as forthcoming and open for suggestions on working hours.
In order to develop and strengthen the nurses and their knowledge, the nurse leaders were very attentive to the nurses’ potential and their need and desire for extended knowledge and education. [X] has an incredible ability to focus on our potential as individuals and no matter what our skills are, she always finds a place one way or another … If there is something you are really keen on she provides you with a specialist position. [Medical department]
Discussion
The findings of the directed content analysis of the four focus-group conversations showed nurses’ experiences of practices in four very different hospital departments with low nurse turnover. A special sense of community in the departments was described: a collaborative fellowship with attentive and supportive colleagues; a strong feeling of mono-disciplinary professional pride; and an embracing leadership with caring and present nurse leaders.
Collegial support was identified as a distinctive part of the nurses’ culture, helping improve collaboration in nursing and patient care. Collegial support as a means for retention overall and position-specific retention is well-known in the literature.3,20,21 Collegial support is often described in turnover literature under the term group cohesion, which characterizes groups according to forces that push the group members closer together. In a systematic review of systematic reviews of interventions to reduce nurse turnover in the adult healthcare sector in the UK, Halter and colleagues 21 found that group cohesion was significantly associated with nurses’ intention to stay. A significant relationship was also found between group cohesion, job satisfaction and intention to stay among newly licensed registered nurses in a prospective cross-sectional design study in Georgia, USA. 21
According to the findings in our study, the nurses’ mutual loyalty and respect for their attentive and caring nurse managers was one of their reasons for staying in the department. Other studies also show that a lower level of turnover among new nurses is linked to the ability of nursing managers to provide support and improve workplace conditions.22,23 In a positive deviance study of nurse managers’ considerations and strategies regarding recruitment and retention in departments with low turnover of nurses, the managers were found to be confident in their leadership roles, targeted towards supporting the special culture in their departments. 24 In a secondary analysis of a cross-sectional survey of newly graduated Canadian nurses, Fallatah and colleagues 5 examined the influence of authentic leadership on new nurses’ job turnover intentions. The study found that authentic leadership plays a paramount role in retaining new graduate nurses due to the leaders’ abilities to raise confidence in nurses’ own abilities to manage work-related challenges, which subsequently results in positive outcomes both for new graduate nurses and the organization. 5
A strong feeling of professional pride gave the nurses in our study the strength to carry on in their jobs. They wanted to provide the best possible care for patients based on the best knowledge. Nurses occupy an in-between position between different practices and responsibilities, and between technology and caring. 25 Sørensen and Hall 25 argue that if nurses perceive that they are focusing their time only on instrumental and technological matters, they also perceive that their pride as nurses is threatened; nurses want to care for the patient’s health and well-being, bringing together different kinds of knowledge. Stress caused by work intensification can also play a difficult role for the nurses’ sense of professional pride. In a survey of 949 Canadian nurses on work experiences and associations between work intensification and job satisfaction, Zeytinoglu and colleagues 26 found that stress caused by work intensification was increased by the nurses’ belief that they were not able to provide what they thought was a necessary level of patient care. The level of patient care was connected to a recent round of budget cuts and subsequent staff shortages, and the full-time nurses appeared to suffer disproportionately from an increased workload as they worked the greatest number of hours. 26
Limitations
In this study, focus-group conversations were used to investigate nurses’ experiences of practices in hospital departments with low nurse turnover. Both authors collected and analysed data together, which supported the establishment of a higher level of trustworthiness, 27 contributing to the credibility of the study. The analysis was further strengthened through discussions with the lay and professional members of the NUCAP-project reference group. Although our focus groups consisted of two to four participants, McLafferty 28 would describe them as mini-groups. McLafferty 28 explains how size influences focus-group discussion and how fewer concepts may be developed. However, smaller groups are easier to manage and there is a greater likelihood that all will participate. 28 Due to the small focus group, transferability could be challenged due to a small amount of data; however, our findings were supported by the literature.
A limitation of our study could be the use of the positive deviance theoretical model, focusing on low nurse turnover and excluding departments with greater turnover problems. The challenge in this case could be that participants might have provided overly positive answers based on their knowledge of being selected for a positive issue like low turnover. However, we were granted positive access to the departments because we came to learn from them instead of focusing on problems. Furthermore, we tried to avoid overly rosy stories by asking focus-group participants about the bigger picture.
Conclusion
Even though the nurses’ daily practice was exhausting, they did not consider leaving their jobs due to the special culture in the departments, which brought the nurses closer together. We encourage others to perform similar local studies to investigate specific turnover strategies, as well as to focus on the important character of nurse management in recruitment and retention of nurses in clinical hospital departments.
In our constructivist study of investigating nurses’ experiences of practices in hospital departments with low nurse turnover, nurses’ reasons for staying were found to be based on a special culture of collegial fellowship, attentive and protective nurse managers, and a strong sense of professional pride. Even though the departments were dissimilar, all the nurses related to the same important practices concerning low nurse turnover. Daily practice was considered busy and exhausting for the nurses and they had considered positions elsewhere, but it was the three main themes identified that required the nurses to remain dependent on each other in many ways, thus bringing the nurses closer together.
There is a considerable range of recruitment and retention strategies to prevent high nurse turnover and address the nursing shortage, and multiple perspectives on nurses’ intentions to stay or leave. The findings of our study are based on a local context and culture of nurses in regional hospital departments; however, our findings are still compatible with the international literature on the subject and therefore have relevance to the wider global clinical practice community. We encourage others to perform local studies to investigate the specific turnover perspectives of nurses, and future research should furthermore be directed towards the development of hypotheses based on the findings of this study and the positive deviance model, testing them in clinical practice settings with larger turnover difficulties.
Footnotes
Acknowledgments
We wish to acknowledge Alfred Deakin Professor Tracey Bucknall, Deakin University, who as adjunct professor at Zealand University Hospital, DK & Institute of Reginal Studies, University of Southern Denmark-DK initially inspired us to study turnover from a positive/best practice perspective. Further, we want to acknowledge our engaged group of critical friends with whom we shared the first analysis of our findings and who helped us understand nursing in the included departments much better.
Funding
This study was funded by grants from The Danish Nurses Organization, Region Zealand and Region Zealand.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.