
Abstract
Nursing is at risk of becoming precarious employment with low wages, poor working conditions, heavy workload and underdeveloped career development possibilities. This study aimed to explore employment precariousness, health and work well-being among permanent and temporary practical nurses and registered nurses. The data were collected from Finnish nurses (n = 5867) using an online questionnaire in autumn 2020. This cross-sectional study was reported by applying the STROBE guidelines. Temporary nurses perceived their health and work well-being as being better than permanent nurses; however, they also perceived higher employment precariousness. Vulnerability, such as being treated in an authoritarian manner, had the strongest negative association with health and work well-being among permanent and temporary nurses. Practical nurses and registered nurses perceived employment precariousness in several dimensions, but this needs to be further studied because the results of this study are somewhat contradictory. Also, further studies are required to survey post-COVID-19 care work, as the pandemic likely affected the study, resulting in higher experiences of precariousness.
Introduction
Fixed-term contracts and temporary agency work are traditional forms of non-standard work, and the number of people in involuntary non-standard work has increased in Nordic countries. 1 Nurses are an excellent example of a professional group in Finland where atypical work, i.e. fixed-term and gig work, has increased. 2 Sweden and Finland are the Nordic countries with the most considerable prevalence of fixed-term jobs; for example, one fifth of Finnish registered nurses work in fixed-term positions.1,3 Also, Finland is among the Balkan countries with the highest share of precarious employment in Europe. 4 Temporary work is one dimension of precarious employment, a concept that lacks a clear definition but refers to insecure, unequal, poor quality and unpredictable employment situations.5–7
Researchers approach precarious employment in two ways: as a narrower classification based on labor market status or type of employment 8 or as a broader societal phenomenon focusing on growing inequality. 9 Problems with precarious employment include ambiguities in the employment contract and its duration, multiple simultaneous employers, lack of social benefits, and legal and practical barriers to trade union membership.10–13 Significant conceptual work and methodological development have been undertaken in recent years in the field of precarious employment.6,14,15 Based on this work, precarious employment is essentially a situation in which several unfavorable work features accumulate and reinforce each other. This study understands precarious employment as a complex phenomenon that is conceptualized by the following dimensions: employment insecurity; individualized bargaining relations between workers and employers; low wages and economic deprivation; vulnerability; limited workplace rights and social protection; and powerlessness to exercise legally granted workplace rights.6,14 So far, the multidimensional approach in precarious employment has not been utilized in Finland, even though it is suitable for quantitative and qualitative research methods and national and comparative settings. 16
Only a few studies have been conducted on employment precariousness in nursing, but they suggest that nursing has features of precarious employment related to austerity measures, staff under-resourcing and increasing workloads.17,18 Precarious employment specifically touches young employees and women 19 and is associated with health, disability, well-being, work motivation, work ability and career and income development.6,8,15,20,21 Precarious work in the care sector is not only harmful for the workers but also for patient safety, and it even increases the risk of death among patients. 22 Nursing is predominantly female-dominated and is at risk of becoming precarious due to low wages, a heavy workload, poor career management and development prospects, limited autonomy, poor quality of management and increased risk of dropping out of decision-making processes.17,18,23–25 Therefore, employment precariousness related to labor policy is not the primary source of precarity in the care sector in Nordic countries because the terms of employment are still negotiated in collective agreements. 10 Also, workers can exercise constitutional labor rights relatively well, and have access to social benefits and protection13,26 that increase the experience of fairness.
Nursing suffers from a severe shortage of personnel due to adverse physical and psychosocial working conditions and heavy workload that may lead to burnout.19,25–27 Care work, in general, is at risk of transforming into a precarious branch of industry. However, the knowledge of employment precariousness of nurses is scarce and multidimensional measurements of precariousness have not been widely used previously. Therefore, we suggest that it is important to study whether problems in nursing are caused by precariousness and what health and well-being consequences this might have. We aimed to explore employment precariousness, health and work well-being among permanent and temporary nurses. Research questions were: 1) How do employment precariousness, health and work well-being differ between permanent and temporary nurses? 2) How are the dimensions of precarious employment associated with health among nurses? 3) How are the dimensions of precarious employment associated with work well-being among nurses?
Method
This is a cross-sectional survey on employment precariousness, health and work well-being among permanent and temporary practical nurses and registered nurses who are working in health and social care in Finland in 2020, and it is reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 28
Setting and sample
This study focused on practical nurses and registered nurses who were members of one of the three trade unions or were working in health and social care workplaces through a workforce leasing company. Trade unions represented the public and private welfare sector's professional workers nationwide, such as practical nurses, registered nurses, social workers, and early education teachers. The workforce leasing company operated in southern Finland, hiring a temporary workforce, for example, for the needs of a large hospital district. Data for this cross-sectional study were collected in Finland between September and November 2020. The researcher (blinded for review ) contacted the human resources (HR) departments of two of the trade unions and a workforce leasing company to send invitations to participate (N = 93,254) and an information letter including a data protection statement by email. One trade union advertised the study in its monthly newsletter. The HR departments sent two reminders, and the invitation to participate in the study was published twice in a newsletter of one of the trade unions.
Data collection
The data were collected using an online self-administered questionnaire. A total of 7925 persons responded, giving a response rate of 8%. Of the total number of participants, seven were excluded because they did not give their informed consent. The sole inclusion criterion was being aged between 15 and 74 years (according to Statistics Finland, the working-age population includes all ages between 15 and 74 years). One participant was excluded because their age exceeded 74 years, and one participant was also excluded because the number of missing values exceeded 50%. This study uses data only from registered nurses and practical nurses and the final sample size was 5817 participants. The sample included principally practical nurses (93%), but we used the term nurse to define the total sample in this study, if not comparing practical nurses and registered nurses.
In the questionnaire, the background variables were age, divided into under 35 years, from 35 to 54 years, and 55 years or more; gender; education, classified as a professional degree and university degree; working sector, divided into healthcare, social services and early education and childcare; and current occupation as a registered nurse or practical nurse.
Employment precariousness was measured using the Employment Precariousness Scale (EPRES). 6 The EPRES contained six subscales, which were coded from 0 to 4; a higher value means higher perceived employment precariousness. Means were calculated for each subscale. The subscale Temporariness included two questions about the current length of employment contract and the time working for the same employer. The Wages subscale asked about the salary level and its adequacy in covering daily and unexpected needs with three questions. There was an option not to give salary information in the Wages subscale, and these non-consenting responses were treated as missing values. The Disempowerment subscale regarded the settlement of working hours and salary with two questions. The Vulnerability subscale included five questions concerning: the frequency of being afraid to demand better working conditions; the frequency of being afraid of being fired; the frequency of being treated in an authoritarian manner; the frequency of being defenseless against unfair treatment by superiors; and feeling easily replaceable. The Rights subscale asked five questions about rights to parental leave, retirement, unemployment insurance, severance pay, and sickness benefit. The last subscale, the Exercise of rights, included five questions about the exercise of the rights mentioned above in the workplace. The total score was a mean of all the subscales ranging from 0 to 4. The data concerning all the questions of EPRES contained 0.2‒1.8% of missing values.
Health was measured on a 12-item Salutogenic Health Indicator Scale (SHIS) that assesses positive health and individual experiences of physical, mental and social well-being and resources rather than illness. 29 Dimensions were perceived stress, illness, energy, physical function, state of morale, psychosomatic function, expression of feelings, cognitive ability, social capacity and self-realization. Each item was scored from one to six, and the total score was the mean of individual scores. The scale has one overall question: ‘How have you felt in the last 4 weeks with regard to the following?’ This question was followed by 12 statements as a semantic differential, options ranging from positive (6) to negative (1). An example of a statement is: ‘In the last 4 weeks, I have felt … felt happy, optimistic (6) … felt depressed, sad (1)’. A sum ranging from 12 to 72 was calculated first, and then it was standardized on a scale from 0 to 100. SHIS contained from 0.3% to 0.6% missing values.
The Work Experience Measurement Scale (WEMS) was used to measure work experience with six subscales, 30 which are: Supportive working conditions (seven statements); Internal work experiences (six statements); Autonomy (four statements); Time experience (three statements); Leadership (six statements); and Process of change (six statements). Each statement was answered on a six-point Likert scale, with options ranging from ‘totally agree’ (6) to ‘totally disagree’ (1). An example of a statement is the following: ‘I feel that my work is meaningful’. A sum for each subscale was first calculated and standardized to a scale ranging from 0 to 100. This was done because the subscales had a different number of statements. Then a total score was calculated as a mean of the subscales. The data regarding WEMS contained 0.2‒2.1% of missing values.
Health (SHIS) and work well-being (WEMS) were measured with instruments that apply salutogenic theory. 31 Salutogenesis involves the idea that an individual's ability to be flexible and to adapt produce health. Flexibility and adaptability are desirable qualities in current working life and are especially needed when faced with insecurity.
The EPRES, SHIS and WEMS scales were double translated into Finnish by the professional translator for this study. After that, the questionnaire was tested before the data collection by ten nurses and nurse researchers.
Data analysis
The data of the current study are derived from the first round of the prospective 36-month follow-up study. The sample size N = 90,000 was based on the following calculations: 95% confidence interval, assumed loss 90% per the first survey round, ten times N was required. We reached a response rate of 8%. We employed a Student's t-test to compare the age, gender and education characteristics between the first (n = 1000) and last (n = 1000) respondents, assuming that the late respondents likely resemble those not responding. 32 Tests were performed because there was a risk that our low response rate, 8%, could lead to non-response bias and non-representativeness of the population of interest. However, there were no significant differences between the first and last respondents.
Characteristics and descriptive statistics of all study variables were calculated as means and standard deviations. We compared background characteristics of permanent and temporary nurses with Student's t-tests and chi-squared tests. Study variable scores, SHIS, WEMS and EPRES subscales were also compared between permanent and temporary nurses with Student's t-tests. Linear multiple regression analyses were applied with the Enter method to examine associations between the EPRES subscales and SHIS and WEMS. Significance was set at the level p ≤ 0.05. SPSS version 27 was used for the analyses.
Ethical considerations
According to the Finnish legislation, this type of study does not need ethical approval. However, permissions for data collection were obtained from the research councils of each trade union and workforce leasing company before the data collection phase. Participation in the study was voluntary, and participants were asked to give their informed consent before completing the questionnaire. The respondents were able to interrupt answering and quit the survey without sending their responses. Furthermore, permissions to use the study instruments were obtained from each of the study instrument authors.6,29,30
Results
The mean age of the total sample of 5817 nurses was 48.3 years (SD 11.03), 14% were under 35 years, 49% between 35 and 54 years and 37% were 55 years or over. Most participants (95%) were women. The participants were employed in the healthcare (38%), social services (35%) and early education and childcare sectors (27%). Among the participants, there were 5453 practical nurses (93%) and 414 registered nurses (7%). Practical nurses were significantly (p = 0.001) older (mean age 48.5 years) than registered nurses (mean age 46.5 years). There were more men among registered nurses (5.9%) than among practical nurses (4.5%), but the difference was not significant.
Table 1 shows the background characteristics of permanent and temporary nurses, which differed significantly. Temporary nurses were younger, more often men, had a higher level of education, and temporary nurses were more often registered nurses than practical nurses. Temporary nurses also worked less frequently in social services than permanent nurses (Table 1). Of the temporary nurses, 306 were so-called ‘gig workers’, meaning that their work assignment in one workplace could be as short as one day. Most of them (85%) were voluntarily working gig-based, but 15% were reluctant gig workers because they had not succeeded in finding any other job.
Background characteristics of permanent (n = 4908) and temporary (n = 909) nurses.
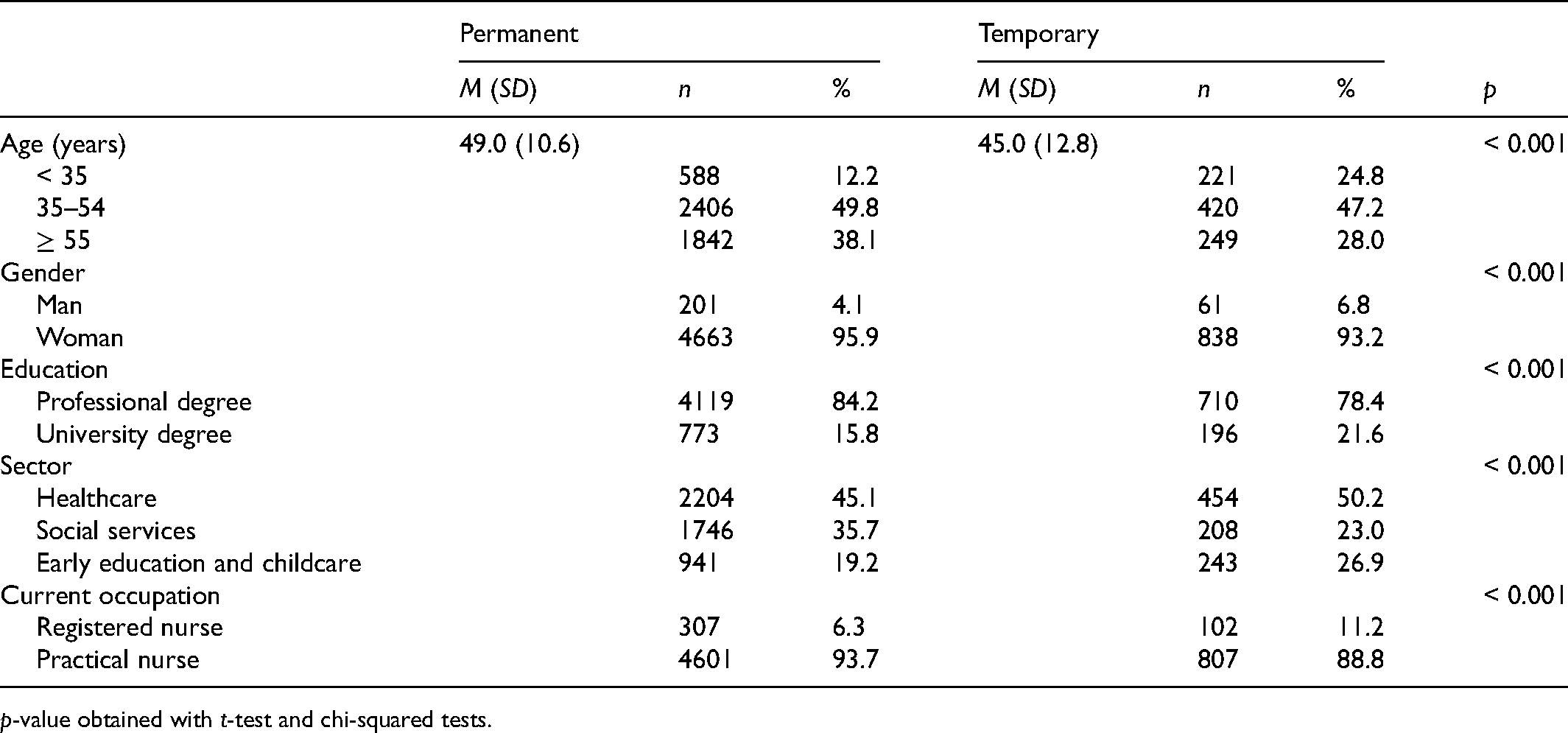
p-value obtained with t-test and chi-squared tests.
Table 2 shows the distribution of SHIS, WEMS and EPRES scores for permanent and temporary nurses. Temporary nurses had a higher score on SHIS; however, the difference was not significant. On the contrary, the WEMS score was significantly higher among temporary nurses. Also, significant differences were found in employment precariousness, measured using EPRES. Temporary nurses perceived significantly higher employment precariousness in every dimension, except for the subscale of Exercise of rights, which showed no differences between permanent and temporary nurses. The Wages subscale showed the highest scores for both groups, followed by the Vulnerability for permanent nurses and the Rights for temporary nurses (Table 2). We further compared SHIS, WEMS and EPRES scores between registered nurses and practical nurses and there was no difference in SHIS scores. The WEMS score, however, was significantly (p = 0.023) higher among practical nurses and the EPRES score was higher among registered nurses (p = 0.005). This indicated that work well-being was lower and employment precariousness was higher among registered nurses.
Means (SD) for SHIS, WEMS and EPRES subscales of permanent and temporary nurses.
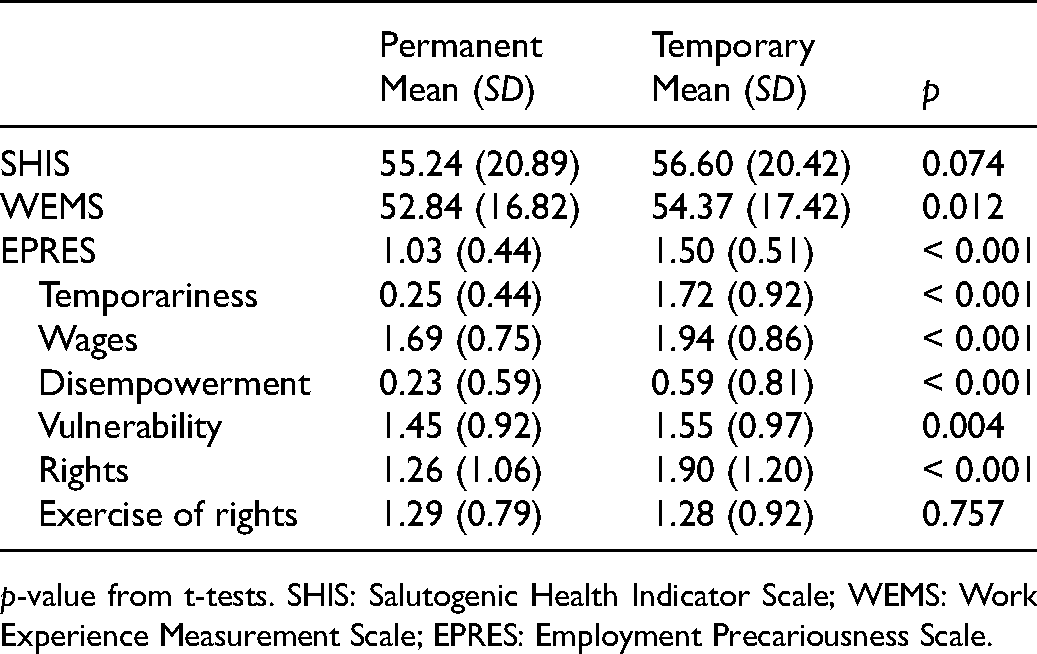
p-value from t-tests. SHIS: Salutogenic Health Indicator Scale; WEMS: Work Experience Measurement Scale; EPRES: Employment Precariousness Scale.
The associations of the EPRES subscales with SHIS were analyzed (Table 3). Results show that the Temporariness subscale was positively associated with SHIS, indicating that shorter employment contracts were associated with better health (β = 1.29). The Wages, Vulnerability, Rights and Exercise of rights subscales had significant negative associations with SHIS, while the Disempowerment subscale did not significantly associate with it. Vulnerability had the strongest negative association with SHIS (β = –7.29). The model explained 25% of the variation of SHIS assessed as adjusted R2.
Multiple linear regression model for associations of EPRES subscales with SHIS among nurses.
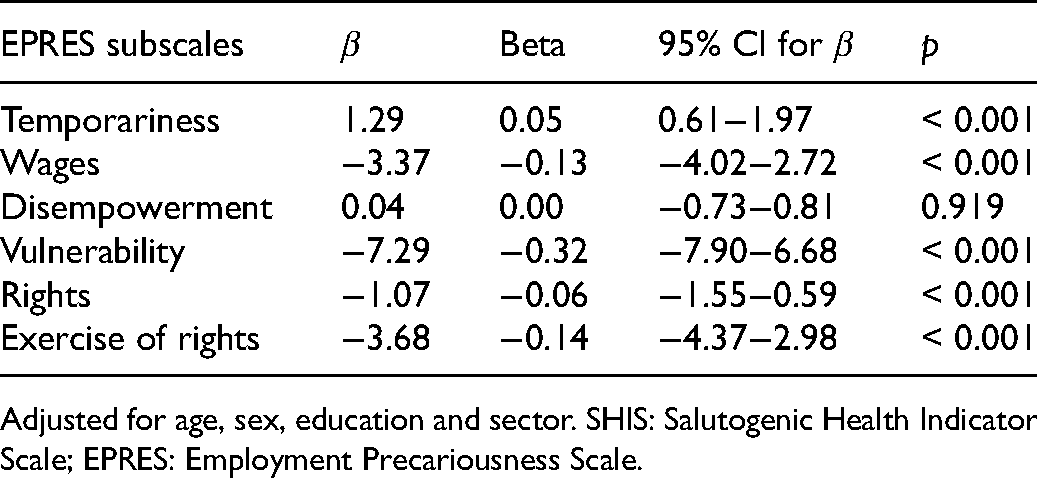
Adjusted for age, sex, education and sector. SHIS: Salutogenic Health Indicator Scale; EPRES: Employment Precariousness Scale.
EPRES subscales were also analyzed in association with the WEMS (Table 4). The subscale Temporariness had a similar association with the WEMS as the SHIS; shorter employment contracts with the current employer were positively associated with WEMS (β = 1.56). Disempowerment did not have a significant association with WEMS; in contrast, Wages, Vulnerability, Rights and Exercise of rights had significant negative associations with WEMS. The most important negative association was between Vulnerability and WEMS (β = –7.96). This model explained 41% of the variation of WEMS (adjusted R2) (Table 4).
Multiple linear regression model for associations of EPRES subscales with WEMS among nurses.
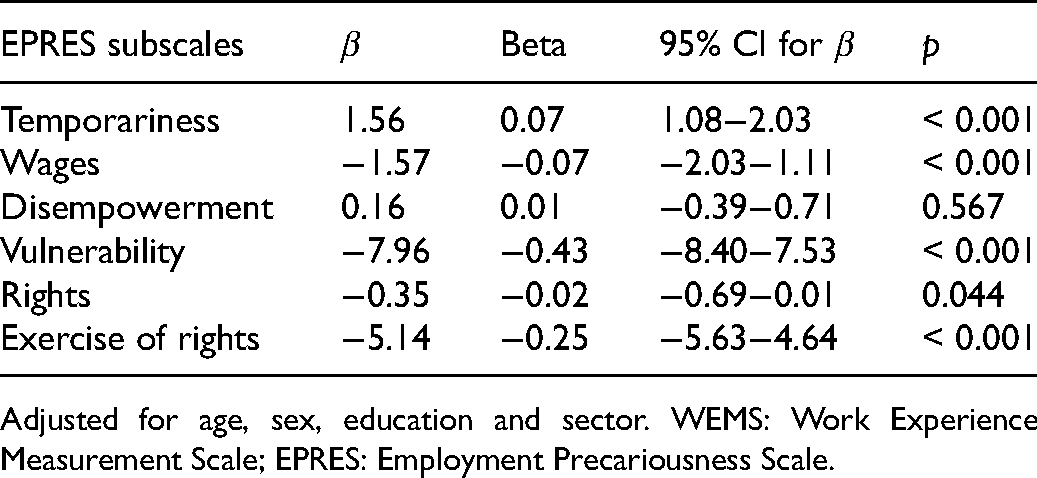
Adjusted for age, sex, education and sector. WEMS: Work Experience Measurement Scale; EPRES: Employment Precariousness Scale.
Discussion
This study showed that practical nurses and registered nurses perceived employment precariousness in the context of a Nordic welfare society that is expected to provide a solid and protective social security and powerful labor legislation. The study assessed perceived employment precariousness with a multidimensional approach among nurses. 6 As far as we know, this is the first study using multidimensional assessment in Finland. Overall, precarious employment among nurses and in the care sector is a sparsely studied area globally. This study principally included practical nurses and a minority of registered nurses, thus, results mainly concern practical nurses. However, our results showed that work well-being was better and employment precariousness lower among practical nurses compared to registered nurses.
Based on our results, employment precariousness seems to be an actual concern in nursing. Precarity was seen in this study's results as dissatisfaction with wages and experiences of vulnerability. Wages are primarily collectively negotiated in Finland, which increases the feelings of fairness but does not prevent dissatisfaction. Vulnerability might, in turn, be a result of an authoritarian leadership that causes fear and feelings of defenselessness. It might also relate to destructive leadership; however, this phenomenon has been poorly identified and has only recently been studied internationally. 33 Vulnerability as a dimension of precarious employment manifests itself as a subordinate position, inappropriate treatment by superiors, and weak autonomy. 6
Temporary workers scored predictably higher in the dimension Temporariness. It is notable that they perceived higher precariousness in all the dimensions of precarious employment. Our finding is consistent with a previous study that showed the higher risk of employment precariousness among temporary workers. 6 Findings from studies on precarious employment indicate that it associates with decreased health.16,20,21,34–36 Still, a Finnish study among healthcare workers showed no adverse effects of temporary employment on health. 37 This association was also found in our research, as temporary nurses perceived better health. They also perceived better work well-being.
Temporary employment in healthcare can be a choice of freedom, as was seen in our results. The reasons for temporariness may be caring responsibilities in the family, but a temporary position is also sought when seeking relief from workload, exemption from duties in the workplace, better earnings, and more autonomy in working shift planning.38,39 Temporary employment might be the only means to regulate stress from work if livelihood is secured, at least to some extent. It might also be that the working conditions of temporary workers are more amenable to the workers. It may be necessary to discuss and prepare for the willingness of nurses to do more temporary work in terms of their career development possibilities, job meaningfulness and well-being at work.
However, a large number of temporary workers might be a burden for permanent employees who must bear more responsibility in workplaces. Currently, there is a labor shortage in Finland's healthcare, social services, and early childhood education sectors, 40 but less permanent employment is available. For instance, according to the job search forum for the public sector, only 47% of the vacancies for registered nurses were permanent. 41 The ratio of temporary and permanent nurses might be an essential issue for further research and nursing management because it concerns the development of nursing and the continuity and quality of care.
When comparing our results with Spanish nursing staff, 17 it is seen that the level of employment precariousness was higher in Finland, somewhat contrary to expectations. In Spain, assistant nurses perceived higher precariousness than registered nurses, but in Finland the results were the opposite. Finnish nurses experienced more significant difficulties living with their salaries, perceived more vulnerability in their workplaces, and were less able to exercise their legal rights. There were slight differences in nurses’ background factors between studies, but the background factors hardly explain all the differences observed in the experiences of vulnerability between countries. Furthermore, in both countries, the participants were mainly practical or assistant nurses.
Also, comparing the employment precariousness with Spanish general workers in permanent and temporary jobs, 6 nurses in Finland perceived more vulnerability, and their assessment of their rights and possibility to exercise their legal rights was worse. Furthermore, when comparing our sample with non-standard Swedish workers, 15 the same elements of precariousness were higher in Finland, namely wages and vulnerability. Interestingly, a European-level assessment of 22 countries 12 showed that Finnish workers in general, alongside those in the other Nordic countries, perceived low employment precariousness.
Strengths and limitations
The strength of this study is that it examined the employment precariousness among nurses in the Nordic welfare state with a relatively large number of participants. Previous studies of employment precariousness in nursing were conducted in Spain, Mexico and Brazil, where labor market conditions and social protection levels differ.17,18,27 Our sample represented Finnish practical nurses well. In this study, 95% were women, slightly more than the percentage in the most powerful trade union for practical nurses. Also, as Finnish nurses, half of the participants were between 35 and 55 years old, but the average age was higher in this study population. Despite the good representativeness, our results have to be considered cautiously due to the low response rate: only 8% of the original sample participated in the survey. Low response rate is recognized to be a growing issue in surveys. Perhaps the low response rate is because we could not send the invitations to the participants directly; the trade unions and workforce leasing company sent them instead. Furthermore, one trade union advertised the study in their newsletter, which possibly did not reach the potential participants. In addition, it is possible that recruiting through trade unions caused selection in responding. The participants active in unions may have been more likely to respond.
To address the potential bias due to low response rate, we tested whether the first and the last respondents differed according to age, gender and education, assuming that the last ones resembled non-participants; 32 however, we did not find any significant differences between these two groups. Furthermore, to promote reliable measurement of precarious employment and international comparability, the employment precariousness scale must be developed to suit the Finnish context better. COVID-19 might partly explain the higher scores in EPRES in our study results since the data were collected during the pandemic, although, at the time of the data collection, the situation was stable and the number of patients in hospitals was low. Nevertheless, some of the registered nurses were transferred from one working unit and task to another without the staff being able to influence it themselves. In addition, the statutory leave and holidays of many registered nurses might have been cancelled or postponed. These measures required by the pandemic might have thus reduced the perceived autonomy experienced by registered nurses. The lower work well-being and higher perceived employment precariousness among registered nurses might result from the abovementioned changes during the pandemic. Therefore, there is a need for further data collection to compare our results with a post-COVID-19 situation in nursing.
Conclusions
To conclude, the detrimental association of employment precariousness with health and work well-being can be seen among Finnish practical nurses and registered nurses, and the association was stronger among permanent workers. In the care sector, temporary employment might currently be one of the means to control the burden of occupation and working conditions if temporariness is a choice of freedom. By developing and studying the leadership at all levels of the organization, and allocating resources for hiring enough permanent staff and developing their working conditions, precarious employment in nursing could possibly be diminished, the well-being of nurses increased and numbers leaving the profession reduced.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Työsuojelurahasto (grant number 200197).
Conflict of interest
The authors declare that there is no conflict of interest.