
Abstract
The number of older people needing care is increasing, and care is often provided by informal caregivers. The mission of family care advisors (FCAs) is to provide them with support; however, whether and how support in existential matters such as existential loneliness is provided is unclear. Therefore, the aim of this study was to describe FCAs’ views on existential loneliness, and existential support provided to relatives who act as informal caregivers to older people. A national survey was distributed to 349 FCAs in Sweden, response rate n = 120 (36%). The STROBE checklist was followed when presenting the study. Existential loneliness was viewed as thoughts about life and meaning (78%). Existential support was provided by dialogues (87%), visits (75%) and support groups (73%); 45% of FCAs stated that they had time to provide existential support and 27% reported having knowledge of how to encounter existential loneliness. FCAs provide existential support, but often lack experience, knowledge and time. Time and knowledge are important prerequisites for acknowledging existential needs.
Background
The number of older people in need of care is increasing, and that care is often provided by informal caregivers, where the largest group comprises relatives. 1 Previous research shows that relatives often experience the caring as stressful, 2 and their own health can be affected.3,4 In addition to stress, research shows that informal caregivers become easily isolated5,6 and may experience loneliness of an existential nature. 7 In addition, research implies the need to focus on and encounter existential matters such as existential loneliness of relatives who act as informal caregivers. 7 A contemporary challenge is, therefore, to discover how to support them so they can continue to provide care for their family members. Physical support or social support are often mentioned, but rarely existential support. 1 To encounter the relatives’ need for support at societal level, new professions and functions have emerged,4,8 for example family care advisors (FCAs). Support, in general, is described as ‘something’ that relatives should have or be given. 9 This suggests that there is a need to ask those who support relatives, such as FCAs, about their views on existential loneliness and existential support provided to relatives who care for older people in their vicinity.
The relatives’ needs can be existential in nature and are often associated with thoughts about the fundamental issues of human life, such as our search for meaning and purpose in life, our need to connect with others and belong, and our awareness of mortality and death. 10 In times of fundamental questioning, existential loneliness can emerge. Existential loneliness is a deeper form of loneliness and is often intertwined with other forms of loneliness. A conceptual analysis illuminated existential loneliness as a phenomenon that occurs when perceiving oneself as disconnected from others, and this may bring out feelings of isolation, alienation, and emptiness. 11 Existential loneliness is also elucidated as a phenomenon that is a part of life, part of what it means to be human, 10 and a part of a process of inner growth. 12 However, spouses who cared for a frail partner late in life experienced existential loneliness as an inner struggle when feeling forced to make difficult decisions regarding their partner's life and when experiencing the loss of the other. 7
To ease existential suffering, it is important to recognize, acknowledge, and share the experience of existential loneliness with others.7,13,14 Existential loneliness can emerge when one cares for a frail older family member – a situation that can be described as ‘double-edged’. The role is considered self-chosen and wanted, 3 but it is also demanding and unavoidable. 6 Having to act as an expert while at the same time be a protector 15 can be rewarding yet difficult.4,5 An empirical study from Sweden that features interviews with significant others who cared for an older family member showed that they viewed their role as that of a devoted companion until the end of life. A prerequisite for being able to be that companion is access to professional care and support when one's own resources and strengths falter. 3 A review of 17 empirical studies showed how people who live in the presence of the death of a family member need continual support in existential matters. In the study, only a few interventions that focused on how relatives’ existential concerns were met were reported. 16 The findings from another review that explored the needs of relatives who cared for an older person living at home reinforced that they needed emotional support from professionals and to develop coping strategies to deal with emotional stress. 17 As similar results were shown in a review regarding spouses in South Korea, 18 this indicates the need for support to be given to informal caregivers.
Informal care involves about 1.3 million people, i.e. 10% of the Swedish population 1 and is primarily a municipal responsibility provided by the 290 municipalities. However, the way in which formal support to informal caregivers is organized and structured differs in different countries. This is shown in a systematic literature review of 44 studies from 17 countries regarding the needs of and support to informal caregivers. The researchers conclude that organized formal support to informal caregivers is urgently required and of high relevance. 19 In addition, a prevalence study regarding informal caregiving patterns in Europe identified variation in how and to what extent informal caregiving is provided, and what different societies and healthcare sectors do to support informal caregivers. 20 One way to organize formal support is to have FCAs. One such example is Canada, where a study that includes interviews with FCAs showed that the advisors saw themselves as a link between the family/relative and the healthcare system. It also showed that they collaborated with many different professionals and that their focus was the family/relative and their needs. 21 Another example from the Nordic countries is Sweden, which since 2009 has had a statutory and tax-financed obligation to provide support to relatives who provide care for someone in their vicinity, 22 and as a solution every municipality is required to employ an FCA. This role is intended to support those who help, support and care for a person in their vicinity. 23 The FCA's role is often twofold – to provide direct support to caregiving relatives and a strategic role to develop caregiver support in their municipality, such as by collaborating with seniors’ organizations, volunteers, and healthcare professionals. Examples of direct support to the caregiving relatives are education, support groups or wellness activities. However, the support can also be indirect, aimed at the older person who receives the care, such as service in the home, daily activities arranged by the municipality, or respite care at a nursing home. The relatives can contact the FCA, but contact is usually established by the FCA getting in contact with the relatives by being present at meetups for informal caregivers. 23 Accordingly, the FCA’s mission is to focus on and encounter relatives’ needs.21,23
From an ongoing debate in Europe about informal caregiving 20 it is easy to presume that support is something that relatives should be given. However, what this ‘support’ entails is unclear. 9 Often physical or social support are identified and determined. 24 By contrast, support in emotional and existential matters is rarely mentioned, despite previous studies indicating a need to focus on and encounter existential needs among relatives who care for older family members. As it is in the FCA's role to support relatives not only in practical but also in existential matters, it is important to understand how FCAs view their mission in relation to existential issues in general and existential loneliness in particular. Such knowledge could be used for developing interventions to support relatives who care for a family member in existential matters. Therefore, the aim of this study was to describe FCAs’ views on existential loneliness, and the existential support provided to relatives who act as informal caregivers to older people.
Method
Design
This current study was explorative, had a cross-sectional design 25 based on a national survey, and is a part of a larger research project about existential loneliness, the LONE study, RR2-10.2196/1307. 26 Using a survey made it possible to explore many people's perceptions of a given statement at a predetermined time. 25 The survey was distributed by email to all FCAs (n = 349) in Sweden whose mission, completely or partially, was designed to provide support to relatives who acted as informal caregivers of older people. The checklist for cross-sectional studies, STrengthening the Reporting of OBservational studies in Epidemiology (STROBE), was followed when presenting the study. 27
The LONE study is in the development phase of designing a complex intervention. 28 One study in the project focuses on experiences of existential loneliness among people who care for a frail spouse (≥ 75 years old) late in life. 7 During the analysis of the interviews with the spouses, a question emerged about what kind of support from the FCA the caregiving spouses receive that is specifically aimed at supporting their existential needs, and this question led us further to the current study.
Sample and setting
The inclusion criterion was FCAs whose mission is to support relatives who act as informal caregivers of older people. The FCAs were identified by searching 290 municipality websites, and a survey was distributed to all identified email addresses (n = 349). Eight (n = 8) of the surveys did not reach any respondents and an additional seven (n = 7) surveys were excluded because the respondents stated that their mission did not concern relatives who provided care to older people. After two reminders, the total number of responses was n = 120 (36%).
Data collection and procedure
A questionnaire was specifically developed for the current study based on pre-knowledge from previous studies in the LONE study regarding existential loneliness and significant others’ need for support, 26 and from available information from the Swedish Family Care Competence Centre regarding FCA's mission. 1 The four authors developed and discussed the questionnaire together and the think aloud method was used to pilot test the questionnaire (see below). The first author had the main responsibility for testing and preparing the questionnaire. The endeavour was to create a questionnaire with a clear structure 29 and therefore it was divided into five parts. The first part involved issues regarding characteristics of the respondents and their public function, such as the age of the FCA, gender, number of years in service, number of inhabitants in the municipality, and perceptions of their public function. The second part included statements about one specific existential concern, namely existential loneliness where the wordings were based on pre-knowledge from the LONE study. The third part focused on statements about who in particular was the focus of the FCAs’ support. The fourth part was based on the Swedish Family Care Competence Centre's recommendations regarding FCAs’ mission 1 and concerned actions and measures undertaken to provide support in existential matters. The fifth and final part was about the FCAs’ prerequisites for providing support in existential matters. For the different parts of the questionnaire see Tables 1 and 2. In parts two to five the FCAs were asked to respond to a statement by rating their answer on a four-point Likert scale 30 ranging from ‘totally disagree’ (rate 1) to ‘totally agree’ (rate 4). The possibility to freely write about other aspects was given for each part of the questionnaire.
Part 1 in the questionnaire: characteristics of the Family care advisors' and their public function.
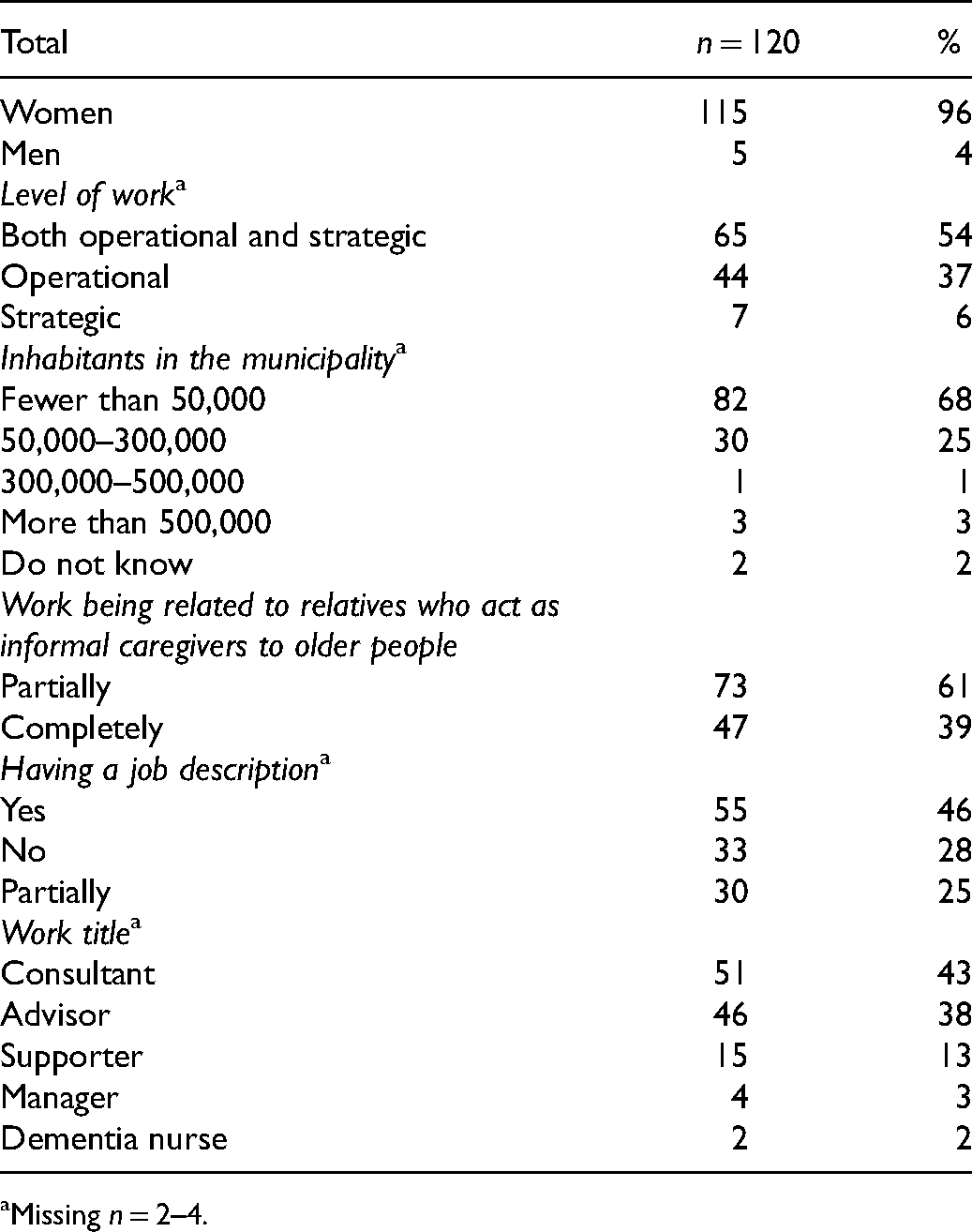
Missing n = 2–4.
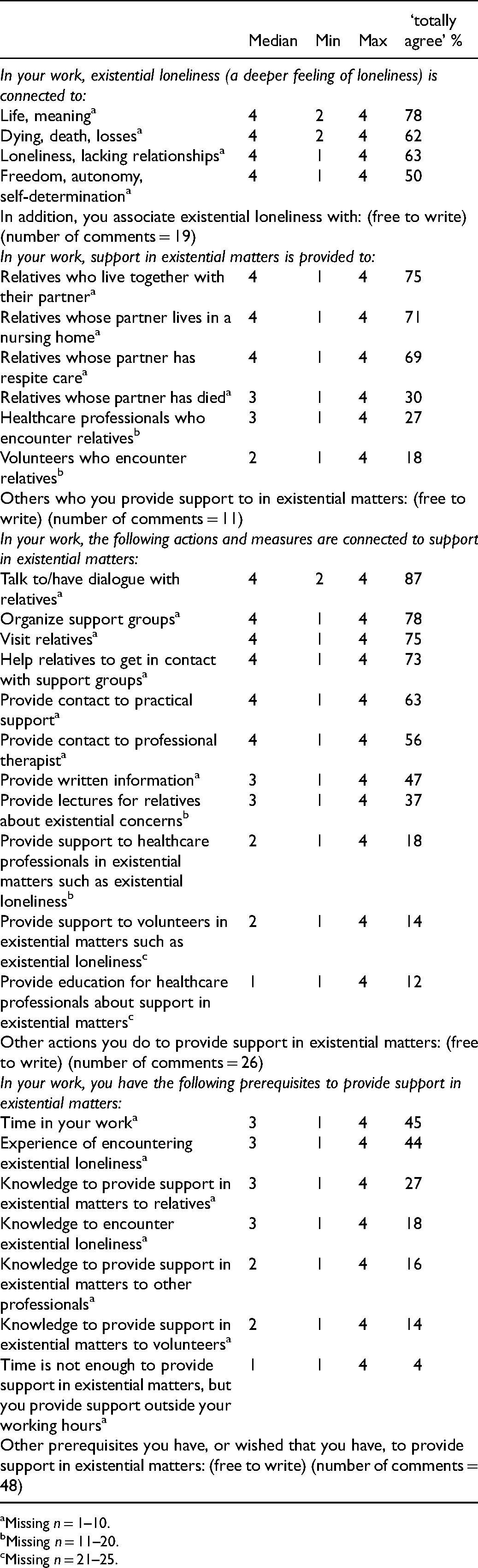
Description of parts 2–5 in the questionnaire; the family care advisors’ views on existential loneliness and existential support.
Missing n = 1–10.
Missing n = 11–20.
Missing n = 21–25.
Attached to the questionnaire was a letter with information about the ongoing LONE study: 26 ‘We turn to you to gain an overview of what kind of support you provide as FCA to relatives of older people regarding support in existential matters in general, and existential loneliness in particular’. Existential loneliness was explained as a deep feeling of loneliness, as in being alone and confined to oneself, and as an experience that seems to emerge when one is in a particularly vulnerable situation and when facing the loss of friends and family members.
Before the questionnaire and information letter were distributed to all FCAs, it was pilot tested in its entirety. 29 Inspired by the think aloud method, 25 the questionnaire was tested by letting one FCA read and reflect upon the statements with the first author present. The FCA read the information letter aloud, shared reflections and then opened the questionnaire, continued to read aloud, and graded the statements. The fact that the FCA read the statements aloud was important, and made it possible to gain an understanding of whether the language was at any point difficult to understand. It was important to listen to the reflections on the statements, especially regarding the topic of the questionnaire, i.e. existential support and existential loneliness. In addition, members in the research team responded to the questionnaire, reflected on, and discussed the contents of the questionnaire, and adjustments were made. When we decided the information letter and questionnaire had been clarified and completed, the survey was distributed through an electronic evaluation system provided by Kristianstad University. The survey was distributed in February 2019 and closed after seven weeks. Two reminders were sent. In order to ensure that the timing was right for the FCAs, and as an attempt to increase the response rate, the second reminder was distributed at a different time and day of the week than the first reminder.
Analysis
The data were processed in The Statistical Package for the Social Sciences (SPSS) version 24.0 (IBM, Corp., Armonk, NY, USA). Descriptive statistics were used, and the median, range and percentages were determined. Inspired by Hsieh and Shannon's description of summative content analysis, 31 the freely written answers in the questionnaire were sorted and counted in relation to each part of the questionnaire and summarized at a manifest level. To illustrate the FCAs’ free writing, statements were chosen from each part of the questionnaire.
Ethical aspects
The study was conducted in accordance with ethical guidelines outlined in the Helsinki declaration, 32 and was approved by the Ethical Review Board in Lund, Sweden (Reg. no. 2018/422). The attached letter explained that participation was anonymous and that their answers would not be possible to track. If they chose to answer the questionnaire, this meant that they agreed to participate in the study.
Findings
The FCAs (n = 120) were five men and 115 women, aged between 34 and 66 years (Md 55 years). Length of time working as an FCA ranged from three months to 27 years (Md 7 years). The FCAs had either no co-workers or possibly one co-worker with similar tasks to them. The FCAs had various formal qualifications: registered nurse (13%), social worker (9%), occupational therapist (7%), behavioural therapist (8%), or other (63%). Other formal qualifications were education in gerontology (43%), communication and support (34%), management and society (9%), psychology and social work (9%), and philosophy and existentialism (5%). The FCAs’ levels of work included both operational and strategic level (54%) or operational level only (37%) or strategic level only (6%). There was a difference regarding inhabitants in the municipalities where the FCAs worked, ranging from fewer than 50,000 inhabitants (68%) to more than 500,000 inhabitants (3%). The FCAs reported that their public function involved providing support by sharing information and providing knowledge (100%), support in everyday life (98%), social support (98%), coordinating support (96%) and providing support in existential matters (95%). For further description of characteristics of the FCAs, see Table 1.
Views on existential loneliness
Of the FCAs, 78% reported that ‘life’ and ‘meaning in life’ had to do with existential loneliness while ‘dying’, ‘death’, ‘losses and loneliness’, ‘lacking relationships’ were reported to be connected to existential loneliness by 62–63%. Fewer FCAs (50%) reported that ‘freedom’, ‘autonomy’ and ‘self-determination’ were connected to existential loneliness (see Table 2).
To summarize the freely written comments (n = 19) in this part of the questionnaire, the FCAs stated that other aspects of existential loneliness were feeling lonely despite having other people around (n = 7), feeling a lack of belonging (n = 5), dwelling on notions of life and existence (n = 5), and feelings of grief and hopelessness (n = 2). The most common comment was that existential loneliness was linked to feeling lonely despite having other people around, for example: ‘If you live together with someone who due to illness has a personality change, for example dementia, then you can experience existential loneliness’. An example of a comment concerning hopelessness was: ‘I associate existential loneliness with the lack of hope, meaning and sense of coherence in life’, while an example of a comment concerning dwelling on notions of life and existence was: ‘Loneliness becomes isolation. Isolation creates confusion—do I exist?—does anyone see me?’
To whom existential support was provided
The majority (75%) of the FCAs provided support in existential matters to relatives who cared for their family member at home, in a nursing home (71%), or in respite care (69%). Fewer FCAs provided support in existential matters to relatives whose partner had died (30%) or to other groups whose purpose was to support relatives, such as healthcare professionals (27%), or to volunteers (18%) (see Table 2).
To summarize the freely written comments (n = 11) in this part of the questionnaire, the FCAs stated that they provided support in existential matters to relatives who needed it, irrespective of the circumstances in their relationship with the person they cared for. An example of a comment was: I provide support to all relatives (adults) regardless of their relationship with the one they care for. They can be adult children to parents, siblings, good friends and so on.
Actions and measures undertaken to provide existential support
The majority of the FCAs provided support in existential matters by talking to and having dialogues with (87%) and by visiting (75%) the relatives. They helped relatives to get in contact with support groups (73%) and organized support groups (78%) for the relatives. Fewer FCAs (37%) offered lectures for relatives about existential concerns. Support to healthcare professionals (18%) or to volunteers (14%) in existential matters such as existential loneliness was rarely given. Offering education to healthcare professionals about support in existential matters was reported by 12% (see Table 2).
To summarize the freely written comments (n = 26) in this part of the questionnaire, the FCAs referred to the fact that they organized courses for relatives that included group discussions about specific topics (n = 15). They collaborated with others (n = 6), used soft massage and meditation (n = 3), and had outreach activities (n = 2). An example of a comment regarding organizing courses was: ‘I arrange study circles for relatives so that they have the opportunity to reflect on their choices in life, recovery, and how everyday life can be managed’. Another comment concerned collaboration and was stated as: ‘I collaborate with many – the churches, the Red Cross, different associations, the library, councils for seniors, health centres and so on’. Another example of a comment concerned using soft massage and meditation: I hold meditation courses, and there, relatives usually come into closer contact with their thoughts and feelings. This in turn usually leads the group into existential conversations, even if it was not intended from the beginning. Relating to pain and suffering is a central part of the meditation course.
Prerequisites for providing existential support
A total of 45% of the FCAs reported that they had time in their work to provide support in existential matters, and 44% had experience of encountering existential loneliness. Only 27% stated that they had knowledge about how to provide support in existential matters to relatives and 18% stated that they had sufficient knowledge to encounter existential loneliness. Of the FCAs, 16% reported that they had enough knowledge to provide existential support to healthcare professionals and to volunteers (14%). A few respondents (4%) reported that they provided support in existential matters outside their working hours (see Table 2).
To summarize the freely written comments (n = 48) in this part of the questionnaire, the FCAs stated that they needed further knowledge (n = 14) and that they wanted to reach out to more relatives (n = 10). FCAs wished that they did not have to be alone in their role (n = 7) and that they could do more for the caregiving relatives (n = 7). They also wanted more time (n = 6) and to collaborate more with others (n = 4). An example of a comment concerning the wish to not be alone in their role was: ‘[I] want to say what I miss: a sounding board, someone to talk to after difficult conversations’. Another example of a comment regarding the desire for more collaboration was: ‘More teamwork! The whole situation around a relative needs much more teamwork to be able to access and help people for change and improvement’. Further, a comment concerning the FCAs wanting to have more time to reach out to relatives was stated as: I wish that I had the opportunity to provide support for a longer time after someone has lost a family member, without being limited to a couple of follow-up conversations. In grief, we refer them to churches or to the Red Cross. Many say, ‘that's when the crisis culminates’, but we have to let go.
Discussion
Even though only a fifth of the FCAs reported that they had the knowledge needed to encounter existential loneliness, the results indicate that the FCAs have an idea of what existential loneliness is. For example, a majority of the FCAs connected ‘life’ and ‘meaning in life’ to existential loneliness. However, less than half of the FCAs reported that they had experience of encountering existential loneliness, even though 95% stated that they provided support to relatives in existential matters. The FCAs had a range of different formal qualifications, which might be one explanation for the discrepancy between their ratings on how they view existential loneliness and existential support. Another explanation could be that this area is not highlighted in the guidelines for the FCAs’ mission; 24 instead focus is placed on physical and social support in everyday life. Even though research claims that existential concerns are a part of everyday life,22,33 support in existential matters is vague in the guidelines. A study in a healthcare context showed that it is demanding for healthcare professionals to encounter existential loneliness, 14 and Udo 34 concludes that practitioners need awareness of the importance of existential issues to be able to provide support in existential matters. Both studies highlight the importance of drawing attention to fundamental human questions, such as those regarding life and meaning, in order to alleviate existential suffering.14,34 It is important to create opportunities for professionals such as FCAs who encounter relatives who care for older people to gain knowledge and experience about how existential loneliness can be encountered and alleviated. This increases their ability to provide support to those caring for older family members, not only in terms of their social and physical needs but also in terms of their existential issues.
The FCAs provided support to relatives by having dialogues with them (87%) and visiting them at home (75%). However, less than half of the FCAs reported that they had enough time in their work to provide support in existential matters, and, in addition, some reported (4%) that they provided support outside working hours. One prerequisite for having a genuine and trustful conversation is to have enough time. Studies both in healthcare and social work fields mention the shortage of time,8,35 effective time, use of time and cost-effective time. 36 This is in glaring contrast to philosophies such as Buber's 37 and to contemporary approaches such as person-centredness 38 reasoning about how time is important for having genuine and present conversations. It is important that ‘talking to/having dialogues with relatives’ becomes a genuine and present conversation – what Buber 37 calls a meeting between I and Thou rather than I and It. Moreover, research regarding alleviating existential loneliness shows that having genuine conversations is key for encountering existential concerns. 13 For further research, it is important to know more about the relation between time and conversations to encounter existential issues among relatives who care for older people.
The results indicate that the focus of the FCAs is often relatives who live together with their partner, and only a third of the FCAs in our study reported that they provided support to relatives who had lost their partner through death. This suggests that relatives who have lost their life-companion may have difficulty finding support for their existential concerns. Moreover, research illuminates the importance of support when losing a life-companion.7,15 However, further knowledge is needed about how and under what circumstances relatives receive support, particularly in terms of their existential concerns when their significant other has died. The results indicate the need for an extended mission so that FCAs, together with other healthcare professionals, can include those who are grieving over a prolonged period. In order to pay attention to and encounter relatives’ existential concerns, their needs must be made visible. A review focusing on person-centredness in care of older persons highlights the importance of looking at the whole context, where the older persons with their significant relationships are the starting point for the care provided. 38 One approach for FCAs would therefore be person-centredness, which involves striving to encounter each person in one's social context and being open-minded to the relatives’ individual needs and wishes. 39
Methodological limitations
There are limitations to this study. The questionnaire was developed only for this study as no existing questionnaires were found. Internal validity, 25 i.e. whether the survey was judged to examine what was intended, was tested partly by members of the research group for the LONE study answering the questionnaire, a form of ‘face validity’, and partly by an FCA answering it using the ‘think aloud method’. 25 In addition, a threat to internal validity is how reliable the responses to the questionnaire were. There was a risk that the FCAs did not understand the attached letter with information or the statements in the questionnaire. To minimize this risk, existential loneliness was described in the information letter. The questionnaire also provided space for free text answers, which was frequently used by the FCAs. This implies that many FCAs who answered the questionnaire found the topic engaging and important. Through the free text answers, we also had the opportunity to assess whether the FCAs had understood the questions and statements in the way intended. In order to reduce the risk that their answers referred to an age group other than older people, only FCAs who focused on providing support completely or partially to relatives of older people were included.
The response rate was low (36%), which is a threat to external validity 40 as there is a risk that the sample was not representative of the entire group of FCAs. However, the response rate is in line with what is expected for an online survey. 40 To achieve a higher response rate, two reminders were sent out to non-responders, the second of which was sent out on a different day of the week and at a different time than the first. However, the composition of FCAs regarding age and gender, and the proportion of smaller and larger municipalities is in accordance with a Swedish national report from 2014, 23 which indicates that a representative sample 25 of FCAs have answered the survey. Still, the result may be difficult to generalize 25 and should be interpreted with caution because of the national healthcare system and the fact that formal support to informal caregivers is organized and structured differently internationally. However, as very few studies with a focus on formal support to informal caregivers exist, this is one contribution of knowledge in a relatively unknown field.
Conclusion
FCAs provide existential support, but they often lack the experience, knowledge, and time. Time and knowledge are important prerequisites for embracing a holistic view that includes acknowledging the relatives’ physical, social, emotional and existential needs. It is thus important to create opportunities for FCAs to prioritize not only social and physical needs but also existential concerns and to collaborate with other healthcare professionals regarding support in existential matters. In addition, the results show that the FCAs want to be able to support relatives who have lost their partner to a greater extent than they do. To provide support in existential matters is important for the existential well-being of relatives who act as informal caregivers, where a person-centred approach could be one feasible way to acknowledge physical, social, emotional and existential needs. Based on the results of this study we recommend that society takes the initiative to provide educational interventions to FCAs about informal caregivers’ existential needs. Such training should combine teaching on existential issues with opportunities for discussion and reflection. To achieve this, the guidelines for the FCAs need to focus more on existential needs and existential support.
Supplemental Material
sj-docx-1-njn-10.1177_20571585211044394 - Supplemental material for Swedish family care advisors’ views on existential loneliness and existential support to informal caregivers of older people: A cross-sectional national survey
Supplemental material, sj-docx-1-njn-10.1177_20571585211044394 for Swedish family care advisors’ views on existential loneliness and existential support to informal caregivers of older people: A cross-sectional national survey by Helena Larsson, Kerstin Blomqvist, Anna-Karin Edberg and Christine Kumlien in Nordic Journal of Nursing Research
Footnotes
Acknowledgements
We are most grateful to the family care advisors who took the time and effort to report their views. In addition, special thanks go to the family care advisor who tested the questionnaire before it was distributed.
Author contributions
HL, KB, A-KE and CK designed the study and developed the questionnaire. All authors were involved in the analysis. HL had the main responsibility for drafting the manuscript. All authors have contributed substantially to, and approved, the final version of the manuscript.
Funding
This study is part of the LONE project supported by grants from the Vårdal Foundation [2014-0127], Crafoordska Foundation [2013-0841], Greta and Johan Kock Foundation [2014-231-401], the Research Platform for Collaboration for Health at Kristianstad University [3/2014] and the Gyllenstiernska Krapperup Foundation [2013-00-16].
Conflict of interest
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.