
Abstract
How to approach adolescents (aged 13–18 years) when their parent is suffering from cancer has become a relevant issue in healthcare, as parental cancer may have an impact on adolescents’ health and development. Nurses are well positioned to identify adolescents’ needs and provide information and support to them but often feel ill equipped to approach them appropriately. The aim of this study was to explore nurses’ experiences of approaching adolescents whose parent had cancer. Interviews with 12 nurses were conducted and analysed in line with a constructivist grounded theory approach. Nurses made efforts to create welcoming environments for adolescents but realised that the contact was unsatisfactory. Primarily, the nurses offered face-to-face conversations with adolescents, which did not correspond with adolescents’ communication channels. To better provide information and support to adolescents, nurses must expand their nursing toolbox so that it is better adapted to adolescents’ communication channels.
Introduction
Parental cancer often affects the family’s everyday routines, and the possibility of the death of the ill parent becomes an imminent threat.1,2 A parent’s cancer may be a challenging experience for adolescents in the family, may have an impact on their healthy development and has been associated with psychological distress such as anxiety and depression.3,4 Consequently, adolescents need extended information about their parent’s diagnosis and emotional support in order to adapt.5,6 Often, they feel that these needs are unmet by family and healthcare professionals (HCPs). HCPs such as nurses and doctors are recommended to directly offer support and age-appropriate information to adolescents regarding their parent’s disease, treatment and prognosis. 7 However, nurses consider adolescents challenging to communicate with. They often feel torn between these challenges and their legal duty to inform and support them.8,9 Consequently, nurses tend to overlook adolescents’ needs, and the adolescents’ healthy development can be at stake. 9 Research on nurses’ experiences of approaching adolescents who have a parent with cancer is limited, however, indicating that there may be some interactional challenges of importance in the healthcare delivered.8,9 Understanding nurses’ perspectives can provide insightful information about experiences that may have potential implications for how professional healthcare is provided. The aim of this study was to explore nurses’ experiences of approaching adolescents whose parent had cancer.
Background
The UN Convention on the Rights of the Child has expanded global awareness about children’s right to be involved in matters affecting them. 10 Norway’s ratification of the Convention has led to legal strengthening of dependent children’s (<18 years) rights and has increased HCPs’ responsibilities when a parent receives healthcare.11,12 Here, HCPs are defined as authorised professionals who perform direct healthcare, such as doctors and nurses. More recently, the UN Sustainable Development Goals have sought to achieve improvement in adolescent health worldwide. 13 Investment in adolescent health confers benefits for adolescents both in the present and in their future adult lives. Promoting healthy development and preventing health problems in adolescents has become relevant to achieve these goals, which calls for particular attention to how health services should tailor their implementation strategies towards adolescents. 14 For HCPs, this involves awareness related to communication skills and supportive environments adjusted for adolescents. The main intentions of improving the quality of adolescent healthcare are to provide easier access to health services and to offer services in ways that adolescents find relevant. 14 To achieve these intentions, health services should become more accessible, acceptable and appropriate for adolescents. It is important for nurses and other HCPs to keep these intentions in mind when creating adolescent-friendly health services.
Adolescence has been characterised as a critical period of transition from childhood into adulthood that involves significant physical, psychological, social and emotional changes. 15 This transition carries a risk for poor health and well-being, as adolescence is considered a vulnerable period of life. Adolescents are, in terms of psychological development, viewed as immature and dependent, not yet fully developed, and they are considered vulnerable to challenging life situations that arise. 15 Thus, they are approached as ‘human becomings’; individuals to be influenced, shaped and changed, with a focus on what they will become in the future. 16 From a sociological perspective, there has been a shift towards viewing children as ‘human beings’ – that is, as active, participatory actors in their own lives. Kjørholt 17 and James 18 argue that the construction of children and childhood becomes constituted within existing laws and policies. In recognition of this view, public authorities are encouraged to consider children’s active citizenship and their voice when creating laws and policies. 18 This idea also applies to healthcare related to parental illness.19,20
Parental cancer has been recognised as a life situation that has significant impact on adolescents’ lives due to their vulnerable phase of life.21,22 Cancer often involves treatments for the patients that cause various exhausting side effects and general discomfort, 23 leaving them with less energy to carry out their parental roles. A parent’s condition throughout the trajectory of treatment, as well as the imminent uncertainty of cancer recurrence, also affects adolescents in the family.5,24 The parent’s frequent hospital visits and repetitive recovery issues become a disruptive part of adolescents’ everyday lives and development. A cancer diagnosis evokes fear, involving worry about the parent’s health and possible death.5,6
A parent’s cancer may lead to personal growth for adolescents, but it may also lead to higher levels of distress, anxiety, poorer quality of life and low self-esteem for some.21,22 These adolescents have a great need for information during their parent’s illness.6,24 They also need emotional support, because they struggle to manage and respond to their feelings connected to the parent’s cancer. These may be feelings that they find difficult to share with parents, close friends or others. Adolescents’ needs have often been overlooked by family members and medical staff, and they have been left to adjust on their own.5,6,21 Negative coping strategies, such as avoidance of discussing cancer-related issues and social withdrawal, have typically been associated with poorer health outcomes for adolescents, whereas positive consequences have been connected to receiving an overview of the situation and having the opportunity to share their thoughts and concerns. 21 Adolescents need to be involved by HCPs with open communication, concrete information and support, but find these needs to be unmet.25,26 Some of them experience being ignored and not having their opinions respected by doctors and nurses because of their young age. Adolescents may also create barriers as to what and with whom they communicate, which can limit their opportunities to be properly informed and to express their needs.25,26 Thus, HCPs need to be proactive in encountering adolescents.
Nurses are well positioned as sources of information because they have the opportunity to create close relationships with the entire family. 27 Previous research has emphasised that nurses must involve both children and adolescents in their parent’s cancer care and provide age-appropriate communication and information.8,9,28,29 However, adolescents have been perceived by nurses as the most difficult relatives to approach. Nurses have reported that they find it easier to deal with younger children because of their more spontaneous responses.9,29 Adolescents were considered more closed and difficult to reach physically and mentally. Although nurses are aware that adolescents may require special attention, research has indicated that nurses may have preconceptions about adolescents, categorising them as challenging interlocutors who are difficult to cooperate with.8,9,29 Encountering adolescents who were silent and withdrawn reinforced these preconceptions among nurses. In addition, nurses have reported that adolescents often exclude themselves from involvement by only making short visits to the parent without requesting any deeper conversations with the nurses.8,9,29 Finally, nurses often feel that their communication skills are insufficient in encounters with adolescents and have struggled with fear of saying or doing the wrong things which could result in rejection or emotional outbursts.8,9,29–31 Consequently, nurses have responded by excluding them from conversations about their parent’s care, 31 distancing themselves from involvement9,30 and leaving the adolescent’s issues to the parents.29,31 Such strategies have been suggested to have roots in nurses’ lack of specific knowledge about how to communicate with adolescents.
Some organisation and counselling programmes have led to improvement in adolescents’ adjustment, emotional functioning and quality of life.32,33 Such programmes are typically facilitated face-to-face by professionals and provided across one or more sessions. In recent years, web-based interventions have proven to be valuable for healthcare support and information. Web-based intervention programmes are easily available for adolescents 24 hours a day. 34 Such programmes provide opportunities for them to anonymously share experiences related to a parent’s cancer, provide and receive support from peers and/or receive regular feedback from professionals. For adolescents, face-to-face counselling and online support are available for them to chat and discuss with peers, volunteers or professionals. 35 It has been suggested that adolescents may benefit from sharing their experiences online with peers with similar life experiences.35
According to Norwegian legislation, those responsible for patients must also ensure that their children’s needs for involvement, information and support are met.11,12 A national guideline has been published to guide HCPs on how to achieve this in practice. 36 HCPs must clarify whether the patient has children, their care situation and need for information and support. Conversations should be conducted with parents about how to best communicate with their children, and also with the children about the parent’s condition. The Norwegian Cancer Society (NCS), a large non-governmental organisation that offers support for HCPs and those affected by cancer, has an extended focus on children’s rights when a parent is ill. 37 Within this organisation, Young Cancer (YC) is run by young people (aged 15–35 years) who themselves have experiences with cancer. Together, NCS and YC offer resources such as digital social media platforms, written information and social gatherings for adolescents who are experiencing cancer in the family.
Global and national statements have specified that adolescents should be involved when parental cancer occurs, and that healthcare services should become more adolescent-friendly. Nurses are required to approach these adolescents, but they perceive a lack of knowledge and communication skills. The aim of this study was therefore to further explore nurses’ experiences of approaching adolescents whose parent had cancer.
Method
Theoretical framework
This article is theoretically framed within the pragmatic constructivist approach of Mead’s symbolic interactionism (SI) to view the adolescents and self.
38
Mead claims: The self is something which has a development; it is not initially there, at birth, but arises in the process of social experience and activity, that is, develops in the given individual as a result of his relations to that process as a whole and to other individuals within that process.38(p.135)
Design and methodology
SI is the theoretical fundament of constructivist grounded theory (CGT) and a CGT approach, as advanced by Charmaz, was used to conduct this study. 39 CGT takes a pragmatic approach to knowledge and emphasises several realities rather than an assumed external reality. The approach is considered useful in analysing the social processes that underlie a studied phenomenon. Thus, a CGT approach is well suited to this study, which examines the shared and constructed realities between the researcher and participants about nurses’ experiences of approaching adolescents who have a parent with cancer.
CGT aims to develop concepts that are analytically generated from the data through a core category. 39 The methodology was guided by theoretical sensitivity and sampling and used inductive approaches to the experiences of nurses, which were gathered through qualitative interviews. The data were analysed through iterative processes by searching for actions and processes to develop substantial categories. By integrating coding, memo writing, sorting of data and comparisons between data, subcategories and a core category were developed. 39
Recruitment and participants
The Central Norway Health region was the target for recruitment of nurses through public hospitals and from municipal healthcare services. Participants were recruited by the distribution of information letters to potential nurses working in hospital wards and outpatient clinics, home care services, school health services and mental health outpatient clinics for children and youth. Criteria for participating were that participants were registered nurses currently employed in healthcare services with experiences in encountering adolescents (aged 13–18 years) with a parent who had cancer during their work. Two male and ten female nurses consented to participate. All the nurses had experiences with adolescents from previous and/or current employment. Brief characteristics of the participants’ education, employment and work fields are outlined in Table 1.
Brief characteristics of the participants’ education, employment and work field.

Interviewed twice.
Data collection and analysis
In CGT, data analysis starts in parallel with the data collection, and categories that emerge from the initial and focused codes together with the memos constitute the first tentative categories. 39 After two initial interviews, the participants’ experiences as they approached adolescents became visible in the data and were further developed as a tentative theoretical category: Nursing tools experienced as inadequate when approaching adolescents. The interview guide was then adjusted to gather more data focusing on the category until saturation was reached. This procedure is in line with Charmaz’ strategy of theoretical sampling. 39 (p.192–193) This meant that more interviews were needed to illuminate and define the properties, boundaries and relevance of this category. Ten interviews with new nurses were conducted and involved more targeted yet open-ended questions to further explore the earlier findings.
Fieldnotes were taken after each interview and included short reflections that served as a starting point for memo writing. 39 Analytical memos were conducted to obtain a deeper understanding about the data, codes, meanings and actions. Follow-up interviews were later conducted with five of the nurses to gather richer data about the category. 39 All interviews were conducted face-to-face, lasted from 60 to 120 minutes and were audiotaped and transcribed verbatim by the first author. Both authors analysed the data and contributed to the construction of categories and writing of the article. The analysis process consisted of initial, focused and theoretical coding, followed by making comparisons between the data, building of subcategories, and finally development of a core category: Nurses’ realisation of an inadequate toolbox. Two categories were constructed to illuminate depth in the core category and each contained two subcategories (Figure 1).
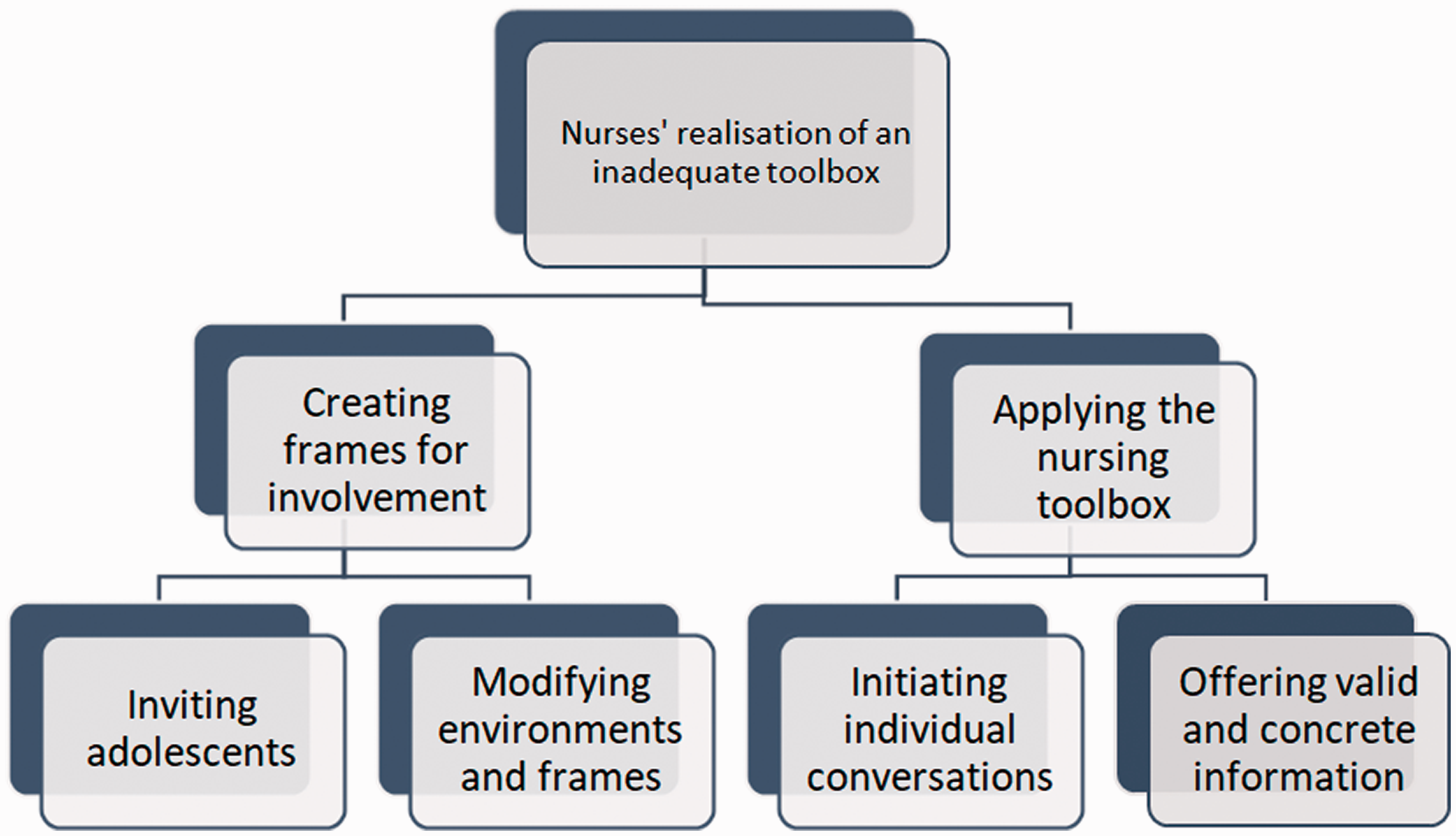
Visualisation of the core category with interrelated categories and subcategories.
Ethical considerations
The study was approved by the Norwegian Centre for Research Data (project number 43985). Information letters were distributed by head managers at the respective workplaces, and participation was based on written voluntary consent. Descriptions of the nurses were kept to a minimum to ensure anonymity. 40 Descriptions of parents, families and adolescents were reformulated to provide privacy protection for third parties.
Findings
Nurses’ realisation of an inadequate toolbox
The core category nurses’ realisation of an inadequate toolbox illuminates how nurses experienced a lack of appropriate tools for approaching adolescents with a parent with cancer. Here, a toolbox is understood as the nurse’s knowledge and communication skills, channels and their ability to provide age-appropriate support to adolescents. The findings were based on two categories: creating frames for involvement and applying the nursing toolbox (Figure 1). All of the nurses were involved in establishing an extended focus on children under the age of 18 years with an ill parent in their work. Although they were beginning to gain some experience in caring for children aged up to 12 years, nurses were less aware of how to approach adolescents. Regarding creating frames for involvement, the nurses’ main tools were to adjust the environments for adolescents, and they distributed written information in the form of brochures and flyers. However, they identified that these tools were inadequate for adolescents, and they also perceived a need for creating more adolescent-friendly environments. In applying the nursing toolbox, which involved offering individual face-to-face conversations, the nurses realised that this was a strategy they preferred. However, this strategy was not always effective for the adolescents, which again made them reflect upon how they could expand it. The integrated categories and interrelated subcategories are based on the nurses’ descriptions.
Creating frames for involvement
The nurses emphasised that children of all ages were welcome to be involved in their parent’s treatment, to take part in family or individual meetings, to obtain information or to attend individual or group sessions with peers and professionals. The nurses had become aware that these approaches should be modified for adolescents. However, they experienced a lack of insight into potential available resources. Two subcategories were created to illustrate this category: inviting adolescents and modifying environments and frames.
Inviting adolescents
Cancer treatment most often took place in outpatient clinics. Nurses usually invited the adolescents by encouraging the parents to bring them to the hospital. The intention was to make them reachable for involvement, information and support. The nurses reached the adolescents indirectly by distributing self-made informational letters or brochures designed by NCS to the parents. By handing out brochures, the nurses hoped that the adolescents felt more seen and included and would have a greater desire to visit the clinic. However, some nurses felt that the language used in these brochures was childish. Nurses were concerned that a lack of focus on this age group could make adolescents feel overlooked. An oncology nurse explained this: Our brochures are a bit general and are more aimed at young children. It would be great to design something for adolescents, not too childish. Not very different from an adult brochure, but something to make them feel that this is actually for them. (Nurse 2) Although we’re open to visitors, the challenge is to meet these adolescents physically. The outpatient clinic is open during the daytime on weekdays when they’re often at school. (Nurse 6) This daughter visited her mother, and I thought this was an opportunity for me to talk with her. When I entered the room, they were lying close together in bed, watching a movie on the iPad. I just greeted her and then of course I left the room. This wasn’t the time for talking. Later I saw her quickly leaving the ward. (Nurse 7)
Modifying environments and frames
Within adult healthcare, nurses illustrated that they had developed more child-friendly environments, such as family rooms with toys and drawing kits and appropriate posters on the walls. The purpose was primarily to develop environments to make children feel welcome. The nurses meant that the environments were less adolescent-friendly. They wished that adolescents would also feel welcome but were unsure of how this could be accomplished. One oncology nurse expressed: Creating environments for the youngest children is the easiest part. These family rooms may be a little childish for adolescents. We could make a room to make them feel more at home. Adolescents like to go to cafés, so maybe we could make a café room for them. (Nurse 2) There are more treatments in homes. In a way, the home becomes the hospital with hospital beds and all the equipment that comes with it. And then we visit maybe three times a day. The adolescents lose their privacy, and it feels unpleasant to bring friends home when mum lies ill in the living room. (Nurse 8)
Some of the nurses had experience in conducting support or bereavement groups for adolescents. The philosophy was to create a supportive framework for adolescents to share their experiences with peers and to obtain support from professionals. Group sessions often included a meal or snack, as well as activities such as table tennis or board games. These group sessions were either conducted at a youth health centre or organised as a weekend camp. However, it was challenging to persuade adolescents to join these groups. Despite several efforts to reach potential participants, only a few adolescents joined. Nurses underscored that the adolescents had to want involvement and to understand the benefits for themselves. One nurse described the challenges of involving adolescents in support groups: Recruiting adolescents has been challenging, but it works well once we make it work. Of course, we ask those we have direct contact with, and advertise in the newspaper and on posters at places we know that adolescents are hanging out. However, it’s difficult. Once, we had to cancel a support group due to lack of participants. (Nurse 1)
Applying the nursing toolbox
The majority of support offered to adolescents was through individual conversations. According to the nurses, adolescents need to talk about their feelings related to their parent’s cancer. However, making adolescents want to talk required the nurses to establish trust and provide valid information. In this category, two interrelated subcategories were created: initiating individual conversations and offering valid and concrete information.
Initiating individual conversations
Nurses emphasised that creating open dialogues with the adolescents was important in order to support them. The nurses offered scheduled meetings with the adolescents or tried to converse where it came naturally. The intention was to help adolescents become aware of their emotions and talk through them to process them. Despite this intention, some nurses found that adolescents were challenging interlocutors; however, a nurse explained how open dialogues could be created: Often, I try to help them during the conversation. I ask something like ‘is this how you feel now?’ and use some emotion schemes with scaling or with colouring of emotions, for example. It becomes clearer to them when they write things down. (Nurse 12)
The establishment of trust was one of the main methods of achieving useful connections, conversations and support. Establishing a trusting relationship with adolescents was considered a difficult task. According to the nurses, building trust was dependent on them having good communication skills and awareness about openness, sensitivity, honesty and genuine engagement with others. Some nurses had developed a repertoire of communication techniques to establish trust with adolescents. Acting interested and being updated could lead to trust. One oncology nurse provided an example of how to build trust in adolescents: You have to find door openers that are not necessarily about the cancer. Ask about what they do in their spare time, then you spin around a bit with things you can see, maybe they play football or something. Then you observe how they respond. And slowly you’re building the trust to make them want to talk about the difficult things. (Nurse 9)
Some nurses expressed that communication with adolescents was an unattainable task for nurses, especially in busy hospital wards. They often felt torn between patient care, competing tasks and requests for follow-up with the adolescents. Occasionally nurses felt that they succeeded in getting the adolescents to talk. These adolescents often asked for a conversation with nurses themselves and were clearly motivated to talk. The nurses expressed that persuading adolescents to talk was part of their job and that achieving these goals boosted self-esteem for the nurses themselves. One nurse explained this experience: It feels good when I get them to talk. This is usually hard, and we really must put in a lot of effort to achieve this. But when I reach this goal, it feels so meaningful to me. I think it’s great to talk with these adolescents, and I’m really surprised about how reflective they are. (Nurse 4)
Offering valid and concrete information
All of the nurses agreed that adolescents should be offered the most valid and concrete information possible about their parent’s condition. Information was provided through a scheduled conversation or continuously during the disease process. According to the nurses, concrete information could provide adolescents with a greater sense of feeling involved. Likewise, misunderstandings could be identified and clarified, as expressed by a nurse: I think it’s important to communicate information that is as valid and concrete as possible. However, we must consider how much information they tolerate, and how to make it comprehensible. Withholding important information is unfortunate, because they can hear it from others, become anxious or develop misunderstandings that might be scarier than the truth. (Nurse 7) The dying mother was laying in the living room. Her 17-year-old daughter was present, but she did not ask me questions directly. But I thought it was important that she was informed about what was going on. It was a bit like I was explaining things that I thought she was wondering about. A little out with my antennas. I became aware of her body language and such. But everything was communicated without questions from her. (Nurse 11)
Discussion
This study illustrated that the nurses were motivated to extend their focus to visiting adolescents at their workplaces. The findings demonstrated that nurses’ dominant toolbox for approaching these adolescents included face-to-face communication and brochures and flyers. However, they realised that they did not reach adolescents in a way they considered appropriate. In outpatient clinics, nurses’ availability did not correspond well to adolescents’ leisure time, while younger children were easier to reach. In addition, home nurses expressed that the parent’s home was often medicalised with equipment occupying the living room, which might have created a foreign atmosphere for adolescents.
The findings are consistent with previous research in this field which has highlighted that nurses are aware that they should involve adolescents, but struggle to communicate with them both through conversations and because adolescents are often not physically accessible.9,30,31 A common view in these studies, however, has been nurses’ implicit understanding that approaches to adolescents should be made through face-by-face verbal communication, and that when they fail this is due to their poor communication skills, lack of knowledge and experience with how to interact with this age group. Whereas previous research has had a dominant focus on how such poor communication affects nurses, nursing and the quality of healthcare provision, this study places greater emphasis on nurses’ attempts to approach adolescents with a parent with cancer.
Developing an adolescent-friendly environment
Nurses in this study made efforts to invite adolescents to talk and to create adolescent-friendly environments to make them feel welcome and acknowledged. However, they found that adolescents did not always make use of the visiting hours, the visiting hours were not always convenient for them, and the adjusted environments and brochures were aimed more at younger children. Even though they knew their toolbox was not adolescent-friendly, they did not actively expand it. Guidelines underscore the importance for adolescents to visit their parents if they are admitted to a healthcare institution, 36 and they suggest that institutional environments should be adjusted with, for example, family rooms, age-appropriate books, toys and informational material. These suggestions correspond with previous research that has recommended creating child-friendly environments, especially in areas that are surrounded by technical equipment.28,29,41 Age-appropriate environments may de-dramatize the hospital, help adolescents to process their emotions and give them a better understanding of the situation. In congruence with the nurses’ experiences in the present study, Holmberg and colleagues 29 noticed that nurses found it easier to adjust environments for younger children than for teenagers. A main focus on younger children might be a reason that nurses overlook adolescents’ particular needs.
Age-appropriate information and adapted support may improve adolescents’ ability to process emotions and to adjust. However, adolescents often experience communication with professionals as limited or constrained. 25 One way to understand these difficulties is to perceive that adolescents may be approached in a state of both ‘being’ and ‘becoming’ in parallel. 18 They are both vulnerable and active actors, which may put nurses in an ambivalent position when approaching them. This requires an individualised and situationally adapted response, while nursing practices are regulated by a limited toolbox and strict time schedule. In line with Mead, 38 it is important for nurses to be aware of the significance of how adolescents’ selves may develop through interaction with their environments. It has been suggested that points of service delivery for adolescents in general should be considered when it comes to developing physical environments and making age-appropriate information available. 14 This could be by means of posters on the wall or relevant official information materials. When a parent has cancer, the nurses become a part of these surroundings. By strengthening collaboration with organisations that offer support to HCPs and adolescents, nurses can offer appropriate informational materials and interact with the adolescents in a manner that suits them and their weekly programmes of activities. In doing so, nurses may indirectly strengthen adolescents’ self-development. If adolescents are not properly acknowledged, they may consequently become invisible in healthcare services and may not be supported in their self-development in a healthy way.
Extending the nursing toolbox
The nurses in this study occasionally approached adolescents by offering them verbal conversations. However, the nurses found this challenging and suggested that adolescents receive less attention, or attention they are not comfortable with. Kazlauskaite and Fife 25 found that adolescents received insufficient or no information from professionals regarding their mother’s cancer, leaving them feeling powerless and withdrawn. These researchers suggested that adolescents must be respected in order to make them feel comfortable. 25 The nurses in this present study might be regarded as somewhat uninventive in approaching these adolescents. Instead of using existing knowledge about the use of digital communication, nurses tried to incorporate even more of the verbal approaches that adolescents did not respond to or withdrew from. Such a mismatch in communication may make adolescents feel less recognised and weaken their self-esteem. 25 Adolescents in general struggle with their selves and self-esteem, 15 and if they are not reached by nurses, they may feel even more vulnerable. Therefore, nurses must be more proactive in seeking out these adolescents and adapting their communication tools to suit them.
Some studies have found that the internet was an important source of information among adolescents.7,42,43 However, it is important that adolescents obtain credible information from websites, and nurses should have a responsibility to remain updated with knowledge about available resources. Organisations such as NCS and others are central providers of information for adolescents.32,33,37 This information includes apps, films, books and hyperlinks to available services. Nurses involved in this study belonged to an age group (40–65 years) that maybe is more accustomed to verbal communication and may not have significant competence around digital communication. It is well known that adolescents communicate much more on social media than middle-aged adults. For example, in Norway 90% of all young people (aged 16–24 years) communicate on social media every day, while the numbers decrease with age. 44 For the age group of the nurses participating in this present study the percentage is down to 60%. Henoch and colleagues 45 found that, even though digital technologies were available, healthcare staff might be in doubt about using them because they were not accustomed to them. In addition, they identified that nurses emphasised the importance of face-to-face meetings with patients and relatives. Support, encouragement and training for nurses is needed so they are able to manage existing digital tools in their workplaces.
It has been argued that services aimed at adolescents should provide information through a variety of channels. 14 Recent research has indicated that available web-based support may be valuable for these adolescents, such as individual counselling and online chatting.34,35 Web-based support is found to allow adolescents to anonymously share experiences and receive feedback and support from peers and/or professionals. A study of adolescents regarding parental mental illness suggested that adolescents sharing experiences in self-help groups online might constitute a ‘communal normalisation’ of their situation as relatives. 46 They felt loss and grief but were able to show their agency and to support others in the same situation. These interventions are in line with a perspective of children as active, participatory actors in their own lives.10,17–19 Consistent with Mead’s 38 perspective on the development of self, nurses should be aware that adolescents can gain this experience in other arenas rather than solely with nurses. If adolescents are more comfortable using digital resources, nurses must be aware of how they can contribute by building a knowledge base about such tools. This also means that nurses must be willing to reduce their control as the main source of support. However, the starting point of their task should be to involve adolescents by providing concrete information about the parent’s present and future situation. Nurses can also benefit from working more closely with cancer organisations to develop a resource bank of digital sources to share with adolescents. Representatives from these organisations could be invited to share information about their work and perhaps participate in workshops with nurses to create a more adolescent-friendly health service. Consequently, nurses can extend their nursing toolbox to disseminate reliable, age-appropriate and relevant information and support in ways that are better adapted to adolescents.
Methodological considerations
Participants in this study were recruited through theoretical sampling with the intention to sample a group of individuals who could best inform about the research issues. 39 Nurses are well positioned to gain experiences about adolescents and were thus considered suitable participants. The nurses were employed within different parts of the health service that provide care for cancer patients and their families in various parts of their clinical pathway. They therefore could have diverse preferences as well as several contextual issues to consider. However, their duty to follow up with adolescents was a common base for their experiences, which were considered comparable throughout the interview and analysis process. Credibility was sought by staying as close as possible to the nurses’ narratives and the methodological principles. 39 Both authors analysed the data separately and contributed with discussions to bring out nuances that led to constructions of trustworthy categories. However, as in all qualitative research the researchers are the research tools and do influence the interpretation process. 39 Therefore, data could have been interpreted differently by other researchers. In line with Charmaz and Thornberg, 47 it is arguable that the findings are transferable to similar parts of the health service and other professionals encountering adolescents in their work.
The nurses contacted the researcher themselves if they wanted to participate and met the criteria. Among the self-recruited 12 nurses, none rejected further participation. The nurses ages ranged from 40 to 65 years, indicating that they were experienced nurses. A broader age range would have been preferable in order to gain stronger theoretical saturation. Younger nurses would have been less experienced but may have been more familiar with digital communication, which might have nuanced the findings. However, in line with Norwegian ethical guidelines, researchers are not allowed to directly contact potential participants. 40 Consequently, the researchers had to rely on those who signed up for participation.
Conclusion and implications
Parental cancer may be a challenging experience for the adolescents in the family. Nurses are required to assess their need for information and support. The findings in this study highlight the mismatch between the nurses’ toolbox and adolescents’ needs, as well as the sparse collaboration with cancer organisations and nurses’ ambivalence in engaging with adolescents. For adolescents to feel acknowledged, communication is important, but information should be more tailored to this age group. The use of available digital resources is recommended. Nurses must become more inventive in their approaches and develop a resource base with information about external support. On the other hand, nurses cannot do everything by themselves, rather, they must organise an adolescent-friendly health service in collaboration with colleagues and cancer organisations.
More research is needed about the adolescents’ own voices and about how nurses experience approaching them, in particular with samples including a broader age-range of nurses. We still do not have a complete picture of adolescents’ preferences for how they prefer to be informed and supported by nurses, which could be an interesting subject for research.