
Abstract
Patients with cancer are expected to call an oncological emergency unit when they are unable to manage symptoms of their disease and side effects from treatment at home. Responding to calls from patients with different problems in a team of registered nurses and medical doctors requires interprofessional collaboration and learning. Therefore, this study aimed to explore conditions for team-based collaboration and learning when responding to calls from patients diagnosed with cancer in a specific setting of an oncological emergency unit. Using a frame of qualitative description three focus groups with 16 healthcare professionals from an oncological emergency unit at a Danish University Hospital were conducted. The verbatim transcribed text was analyzed using content analysis, and reported according to the COREQ guidelines. Two main themes emerged: 1) ‘Availability – a precondition for learning and collaboration’ and 2) ‘Sense of responsibility and distribution of roles’. The study demonstrated that interprofessional collaboration and learning were affected by intra and interprofessional and contextual factors. In addition to an awareness of personal attitudes, the environment and the distribution of responsibility and roles as essential preconditions for accomplishing teamwork need to be explicitly articulated if the team-based learning and collaboration are to succeed.
Introduction
Studies point to the benefit of interprofessional collaboration and the need for interprofessional learning.1–3 Still, there can be barriers to this collaboration in teams. 2 A potential discrepancy in registered nurses’ (RNs) and physicians’ experience of teamwork may compromise collaboration and knowledge exchange when responding to calls in an oncology emergency unit (OEU). Thus, to improve patient care, it seems important to focus on how collaboration and learning take place in a team consisting of RNs and physicians in this setting.
Background
To increase patient survival after cancer, the secondary healthcare sector has undergone an increasing specialization over recent decades which also affects organizing oncology into sub-specialities. 4 The organization may be beneficial to patients and healthcare professionals (HCPs) as it ensures that physicians and RNs possess deep knowledge about treatment modalities and side effects regarding specific patient groups. However, sub-specialties can be associated with disadvantages when HCPs need to support patients outside their area of expertise. 5 Consequently, HCPs may be challenged by a lack of knowledge when they respond to calls from patients with cancer diagnoses that exceed their area of specialization. This underpins the urgency of interprofessional collaboration and learning to support teamwork in OEUs.
Based on a concept analysis, teamwork is described as a dynamic process involving two or more HCPs with complementary backgrounds and skills. 6 Teamwork is achieved through interdependent collaboration, open communication and shared decision-making. Following the interdependency, team members are mutually reliant on each other to accomplish and complete their work.1,3,6 In a team, the members interact to achieve shared goals for the patients and endeavor to make a concerted effort in assessing, planning and evaluating patients’ care. 6 Thus, an efficient team generates value regarding patients’, organizations’ and HCPs’ outcomes.
To improve health outcomes, the World Health Organization (WHO) 7 points to interprofessional learning as a central aspect. Interprofessional learning is ‘when two or more professions learn about, from and with each other’, which requires a willingness to understand one’s own and others’ role and responsibility in the team. 7 Additionally, it requires an ethical practice that involves understanding the views of others and acknowledging that these views are equally valid and important. 7 Thus, interprofessional learning adds to the definition of teamwork as it crosses professional boundaries and requires an ethical attitude in terms of respecting each other’s contributions to the team.
In addition, to support effective, safe and timely care, effective communication is essential.8–10 However, effective communication can be prevented by miscommunication or delayed communication from physicians to nurses, 9 as well as negative attitudes regarding the importance of communication. 11 Moreover, HCPs can have different expectations concerning collaboration and communication, which may influence whether communication contributes to facilitating or preventing high-quality patient care. 9 Thus, potential discrepancies between RNs’ and physicians’ experiences of team collaboration may influence the way they work cooperatively, share responsibility for problem-solving and make decisions for patient care.
Therefore, the study aimed to explore conditions for interprofessional collaboration and learning when responding to calls from patients diagnosed with cancer in a specific setting of an oncological emergency unit.
Method
The study was designed as a qualitative descriptive study 12 and used focus groups (FGs) for data gathering. 13 Within a qualitative descriptive approach, it was possible to stay close to data and interpret it in everyday language to explore everyday events.12,14 Gathering data by means of FG discussions supported participants to share and compare their experiences and create variation in the data. 13 The variation was ensured by conducting two homogenous FGs with, respectively, RNs and physicians and one with a mixed sample, by combining HCPs from in-patient and out-patient units and by including HCPs aligned to different diagnosis groups. Content analytical steps were used to describe the manifest and interpret the latent content of the data. 12 The study was reported according to the Consolidated Criteria for Reporting Qualitative Research (COREQ). 15
Setting
The study took place in an OEU at the Department of Oncology at a Danish University Hospital, between June and August 2018. During the day, Monday to Friday, the OEU is staffed with a team of two RNs from, respectively, an out-patient and in-patient unit with a minimum of two years of experience in oncology. The nurse from the out-patient unit works in a specific diagnosis team and the in-patient nurse takes care of patients with different diagnoses. Additionally, an attending physician with specialist competencies and a resident assistant (a physician in training) staff the unit. To address the callers’ needs, the constellation of the team covers complementary competencies based on the HCPs’ professions, levels of experience and whether they work in the in-patient or out-patient unit. The team varies from day to day and staff do not know who they are going to collaborate with that specific day. The team is confined to the same room and responds to calls from patients and relatives affiliated with the Department of Oncology where they provide the callers with advice and guidance and assess their need for physical examination and/or admission.
Participants
As recommended for descriptive studies, the participants were purposefully included. 12 In total 16 HCPs with different competencies due to their profession, level of experience and daily workplace in either an in-patient and/or out-patient unit were invited from among HCPs who were assigned to work in the OEU on scheduled days. The participants were invited by mail and none declined the invitation. The sample had a mean age of 40.8 years (range 25 to 61 years) divided between nine nurses (mean age 45.9, range 30 to 61 years), and seven physicians (mean age 34.6 years, range 25 to 41 years). Their oncological experience varied as nurses had a mean of 17 years (range 5.5 to 30 years) and physicians a mean of 3.6 years (range 3 months to 12 years) (Table 1).
Participants.

Data gathering
The FGs took place at the hospital in a convenient room set aside for the purpose. The participants and the moderator, an experienced researcher in oncology without daily contact with the participants, were situated around a table. An observer, a development nurse from the department, sat at a distance from the table. The question, ‘How do you experience the opportunity to collaborate and learn as a team?’ was asked to set the discussion in motion. Subsequently, the moderator ensured that the thematic interview questions were covered (Table 2). Probing questions from the moderator or the observer were asked only to clarify and elaborate on what was said during the discussion.
Thematic interview questions.

A debriefing took place at the end of each FG to make sure that the participants had nothing further to add to the topic. 16 The FGs lasted from 69 to 108 minutes (mean 91 minutes) and were recorded using a digital recorder.
Analysis
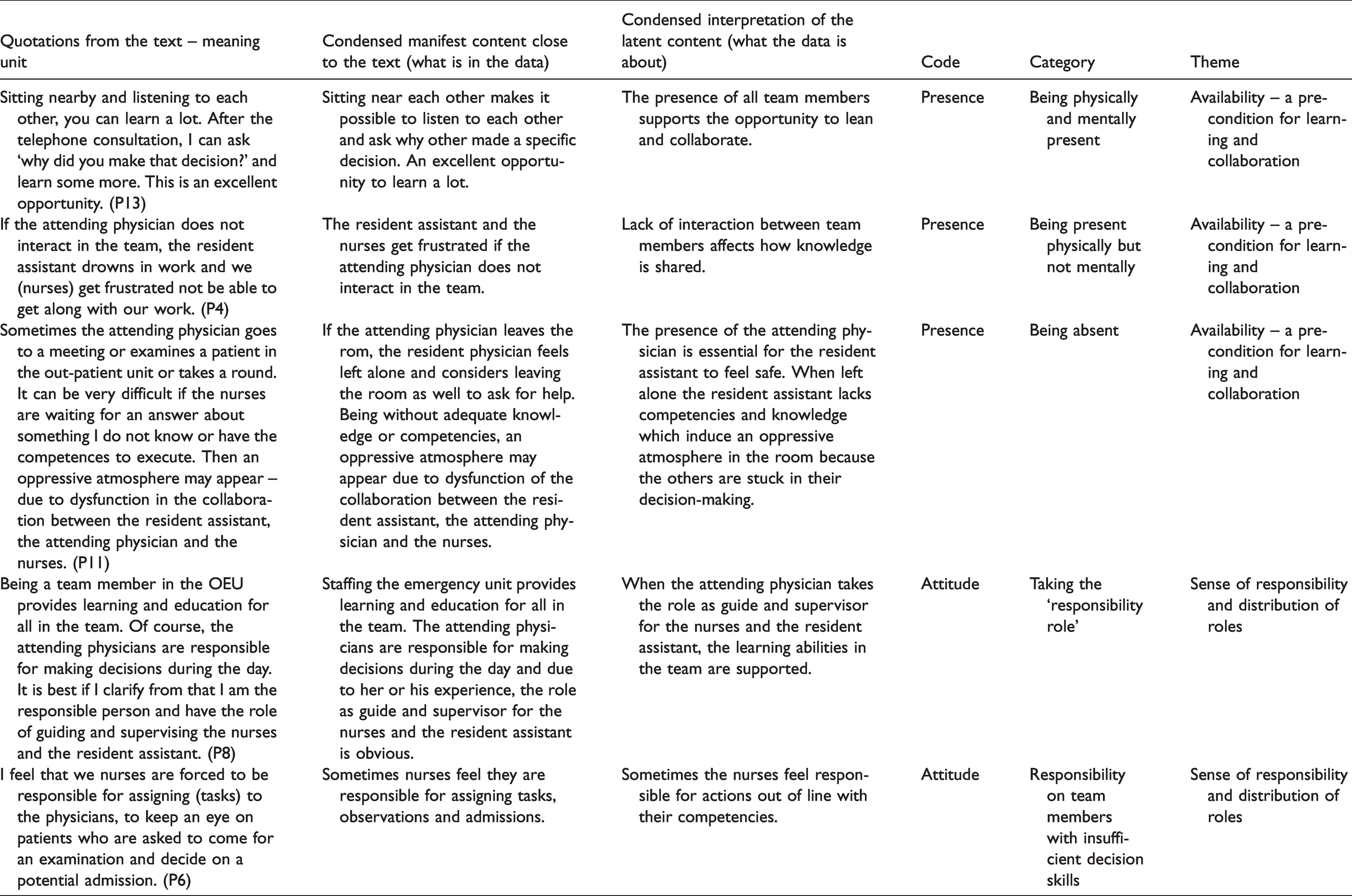
After verbatim transcription of the FGs, content analysis was conducted inductively to understand not only the manifest content but also the latent content of the participants’ experiences of collaboration and learning in the team. 12 Thus, we moved from ‘what was in the data’, the manifest content, to ‘what the data was about’, the latent content. Combining qualitative description using content analytical steps, it was possible to stay close to the data and to interpret the underlying meaning on a low abstract level.12,17 To structure the data, the text was condensed and coded independently by all authors (two RNs with PhDs and one RN with a healthcare diploma). 17 Subsequently, all three authors discussed the coding and proceeded with the analysis by creating categories and looking for recurring themes (Table 3). This process of independent and interdependent analysis aimed to minimize researcher bias 18 and to include the authors’ varied interpretive repertoires. 19
Examples of stepwise analysis.
Ethics
The Danish Data Protection Agency approved the study (ID 2008-58-0028). The participants joined voluntarily and signed an informed consent form after receiving written and verbal information about the study.20,21 Anonymity and confidentiality were ensured by exchanging names for ID numbers. Data were only available to the researchers and stored in a password-protected computer.
Findings
The analysis revealed two themes. The first theme ‘Availability – a precondition for learning and collaboration’ illustrated how availability was described as a continuum from being physically and mentally present, to being physically but not mentally present, and to being absent. The condition of being available led to the second theme, ‘Sense of responsibility and distribution of roles’ that illustrated how responsibility was closely related to the perception of one’s role in the team.
Availability – a precondition for learning and collaboration
Being physically and mentally present represented a precondition for interprofessional collaboration and learning. In addition to being physically present, this also meant mental attention to assignments and potential challenges among team members when they were responding to calls. Physical availability, combined with mental attention to how other team members solved problems on the telephone, was displayed in the following sequence. I am available by being in the room and listening to the conversation although I am doing something else. I sense a lot and consider; is there something we need to discuss? (MD, FG3, P16) Yes, it is unavoidable to listen to each other’s conversations sitting so close. (RN, FG3, P14) I am attentive to the responder’s questions and then I consider; is this a patient who needs admission. (MD, FG3, P15) Exactly, it is possible to sense, do I have to interact. (MD, FG3, P16) Sitting nearby and listening to each other, you can learn a lot. After having listened to a telephone consultation, I can ask ‘why did you make that decision?’ and learn some more. This is an excellent opportunity. (RN, FG3, P13)
In some cases, team members were present physically but not mentally. The discussions in the FGs revealed that some attending physicians paid no attention to team collaboration and effectively resigned from the team when performing other tasks, e.g. following up on delayed office work, visitation of new patients etc. Although their physical presence was pivotal and could provide a safety net for the other team members, lack of communication negatively influenced team collaboration and learning, which appears in the following sequence. A patient needed to be seen by a physician and suddenly she (the patient) had disappeared. In the room, we, the resident assistant and two nurses discussed her disappearance and went out to look for her. Later it turned out that she was sent home by the attending physician. It produces a lot of work if one person does not communicate. (RN, FG1, P2) Yes, we all need to participate, but if three people talk about a missing patient without any reaction from the fourth person in the room … this is not OK if you work as a team. (RN, FG1, P4)
The team members acknowledged the need for accomplishing competing assignments due to a heavy workload, specifically for the attending physician. However, the withdrawal and mental absence of a team member affected the amount of courage needed to ask for help, although all knowledge and competencies in the team were needed. A nurse said: If the attending physician is stressed and snaps – we (nurses) talk to each other (to solve the problem) trying to avoid disturbing although we needed advice from the physician. (RN, FG1, P2)
The advantages of being in the same room were contrasted by some disadvantages belonging to contextual factors that led to physical absence in the room. The environment could be noisy, with telephones ringing and HCPs talking loudly on the telephone at the same time. In some cases, a team member left the room to hear what was being said in the telephone: If the examination room is free, I use this room because it is difficult for me to concentrate if a lot is going on in the office. I need to talk to the patients alone. (MD, FG2, P10) Sometimes the attending physician goes to a meeting or examines a patient in the out-patient unit or does a round. Then I am left alone as the responsible physician. It can be very difficult if the nurses are waiting for an answer about something I do not know or have the competencies to execute. Then an oppressive atmosphere may appear – due to dysfunction in the collaboration between the resident assistant, the attending physician and the nurses. (MD, FG3, P11)
Sense of responsibility and distribution of roles
In all FGs, the participants agreed that collaboration in the team should be founded on a willingness to listen to each other, asking and answering questions, feeling obligated and responsible for each other and for the assignments of the day. Performing these values required a clear vision of how responsibility and roles essential for team collaboration should be distributed among team members. However, it seemed the distribution of responsibility depended on how the team members viewed and executed their roles: Being a team member in the OEU provides learning and education for all in the team. Of course, the attending physicians are responsible for making decisions during the day. It is best if I clarify that I am the responsible person and have the role of guiding and supervising the nurses and the resident assistant. (MD, FG2, P8) It is important to work in a learning environment where you feel safe to ask questions and to have the attending physician nearby to back us up if necessary and explain why a decision is made. It is possible to learn a lot from the attending physician. (RN, FG1, P4) For some physicians taking the lead comes naturally. However, for others it is totally laissez-faire because our expectations of each other are unspoken. (RN, FG3, P14) I can learn a lot from the nurses. They have a lot of experience that I do not have. For example, I ask them questions about medication for nausea. The attending physicians are also often willing to elaborate and explain if I ask them. (MD, FG3, P11) I feel that we nurses are forced to be responsible for assigning (tasks) to the physicians, to keep an eye on patients who are asked to come for an examination and decide on a potential admission. (RN, FG1, P6) Our responsibility is to share our thoughts and observations with the physicians. However, we must be aware not to indirectly become responsible for the decision. To prevent this, I urge the resident assistant to discuss the problem with the attending physician. (RN, FG1, P3)
Discussion
The study aimed to explore conditions for interprofessional collaboration and learning when responding to calls from patients diagnosed with cancer in a specific setting of an OEU. Although other studies about interprofessional learning and collaboration do not describe availability in the same room as a key point,7,8,22 an essential factor for learning and collaboration in this OEU setting depended on every team member being mentally as well as physically available. In these cases, sitting near each other supported interaction and opportunities for knowledge exchange, reflection and feedback in a team of HCPs with complementary backgrounds and skills. 6 However, the interaction was affected if some of the team members were unavailable physically and mentally whether because of contextual factors like environmental noise and competing assignments, specifically for the attending physician.
Lack of support and access to knowledge from medical specialists may contribute to a waste of time and sub-optimal patient care.9,23 This is underpinned by our findings that showed HCPs occasionally were unable to proceed with their work due to lack of support and collaboration. However, except for noise, doing a round or keeping up with other appointments indicate a requirement to be in two places at the same time, which may also prevent the attending physicians from executing their work at the OEU properly.
An additional inhibitor for team collaboration and learning seemed to be the absence of a common understanding of collaboration and learning as a means to integrate effective collaborative practices.3,24 The understanding of the inherent values in team-based collaboration and learning is crucial as this understanding creates a foundation for the execution of a unique team-based interaction. The findings in the present study indicated that the team alternated between an implicit understanding of being an interdisciplinary team and an interprofessional team. In interdisciplinary teams, team members contribute with their knowledge and skills in specific patient cases in a hierarchy based on knowledge and organizational prestige. 24 By contrast, to act as an interprofessional team requires a shared responsibility for the functioning of the team, which means sharing leadership and applying one’s unique and overlapping knowledge and skills, 24 open communication and shared decision-making.1,3,6 Thus, leaving the room, whether it was due to noise or competing assignments, contributed to devaluing availability, and consequently learning and collaboration, as well as the possibility to extend one’s professional boundaries, which is essential for success in team-oriented care.10,25
Absence could decrease the potential benefit of team collaboration including mutual respect for one another and one another’s professions and willingness to participate in a cooperative atmosphere.22,26 The change from a cooperative atmosphere to an oppressive atmosphere appeared evident when some of the team members were left without sufficient skills to proceed with their work. This highlighted the interdependence among team members, and the fact of being mutually reliant to accomplish and complete one’s work 1 was fragile as absence prevented access to adequate support – a precondition for optimizing learning in teams. 27
Another condition that influenced team collaboration and learning could be the organization of the team. The FGs indicated that collaboration and learning opportunities depended on the ‘staff of the day’. Following this, responsibility and role distribution became key points in this current study. An explicit distribution of roles may lead to team members feeling secure and ensure completion of tasks with the necessary competencies being available for the exchange of views and support.8,22 In our study, the participants seemed to be aware of the importance of interprofessional collaboration. They wanted to learn from each other and were aware of their interdependency and the need for executing continuous sharing of information and decisions as required for a team. 28 However, being forced to perform their delegated responsibility independently with minimal interaction with the whole team signaled a potential gap between team members’ interpretations of responsibility and roles.
Role blurring may occur when there is confusion about where one’s practice boundaries begin and end. 29 We found a potential role blurring when some of the HCPs felt forced to make decisions that exceeded their professional boundaries and took responsibility on the edge of their competencies. Bearing this in mind, role blurring may unintentionally compromise high-quality care. In addition, the organization of the OEU with staff that differed from day to day and a heavy workload on staff members may influence a common understanding of how to succeed in collaboration and learning in the team. According to Thies et al., 30 success in collaboration requires organizational support and sometimes redesign of staff roles, responsibility and workflows. Consequently, a lack of these factors may lead to damaged collaboration across professions, and, in the worst case, a non-ethical practice that may influence patient safety as the patients’ healthcare problems are not addressed adequately.
To address patients’ healthcare problems, the benefit of multiple overlapping competencies is evident.2,23 However, about empowering and clarifying interaction and collaboration, every team member is supposed to contribute with their expertise, 3 which requires knowledge of each other’s expertise. This calls for communication between team members 31 that needs to happen in an effective and timely manner. 8 Our findings demonstrated that unspoken expectations about roles and responsibilities occasionally affected the communication between team members, specifically when the learning environment felt unsafe. As communication and reflection are essential to promote the feeling of security in collaboration and decision-making,8–10 lacking communication influenced how it was possible to facilitate a common understanding of each other’s actions and the potential of extending one’s professional knowledge. When the attending physician did not take the expected role as a guide and supervisor, the opportunity to maintain reciprocal interdependency with an exchange of knowledge was put out of play. 1 A vacuum seemed to appear, which called for a shared leadership. 24 However, this was difficult to accomplish due to professional boundaries and competence levels. Consequently, the team-based reflection in an open, honest conversation as the basis for quality improvement was under pressure,7,26,32 which may compromise the patients’ safety, lead to medical errors and delay management of symptoms.
Limitations
To explore collaboration and learning in an OEU, a qualitative descriptive methodology is suitable as this approach captures information from those who directly experience the phenomenon studied. 14 We included a varied sample of nurses and physicians, who were willing and able to contribute with their experiences. Initially, the groups were homogenous in accordance with Morgan 33 who argues against establishing groups that cross status and authority lines. Listening to the two homogenous FGs suggested a safe collaboration across the two professions. Therefore, we decided to conduct a mixed FG to explore whether the heterogeneity could contribute to a more varied perspective that was not expressed in the two homogeneous groups. However, inviting a selected sample of participants may have contributed to establishing groups with participants who were too much in agreement with each other, independent of being homogenous or heterogenous. Thus, it may be questioned whether adding more groups would have contributed to further findings, although we found the credibility of the study was supported by conducting three groups with four to six participants as they were productive and enabled fulfilment of the aim of the study. 17
According to Bradshaw, Atkinson and Doody 14 findings from qualitative descriptive research are constructed by the participants as well as the researchers. We endeavored to reduce the risk of social desirability in the FGs by letting the participants discuss while keeping interference from the researcher at a minimum. 16 However, adding observations in the OEU could have contributed with more angles of the collaboration and learning environment in the natural setting. 12 In addition, the research group was small and consisted of nurses. Although the qualitative descriptive approach required us to stay close to data and confirm our analysis with quotations from the FGs,12,14 including other professions may have added additional views and strengthened the analysis. The transferability of qualitative research findings is dependent on the context. Accordingly, our findings are limited to telephone-mediated care performed in a team consisting of nurses and physicians.
Conclusion
The study demonstrated that several conditions affected collaboration and interprofessional learning in an OEU. Although the dependency on the physical and mental availability of all team members in the room and a clear distribution of roles and responsibilities were essential factors, contextual factors also appeared as inhibiting factors for interprofessional collaboration and learning. Competing assignments and noise required some team members to leave the other team members alone, negatively affecting collaboration and the learning environment. Additionally, the lack of an explicit articulation of essential preconditions for accomplishing teamwork in a team that differed from day to day made it difficult to establish and ensure consensus about how collaboration and learning were a shared responsibility in the team. Lacking the opportunity to share one’s considerations with all team members, interpersonal as well as intrapersonal learning was affected in an inappropriate way that potentially could influence patient safety. To manage these barriers, staff leaders must pay continuous attention to working conditions for all team members in order to develop and maintain a culture in the OEU that supports interprofessional collaboration and learning successfully.
Footnotes
Acknowledgements
The authors would like to thank the participants for their appreciated participation that has contributed with important knowledge about their experiences of collaboration and learning in an oncological emergency unit.
Author contributions
HRJ, BP and LJ designed the original study. BP and HRJ gathered the data. HRJ, BP and LJ contributed all to analyzing the data. HRJ and BP drafted the paper. All researchers revised and approved the paper which presents the results of our original research that is not being considered for publication elsewhere.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.