
Abstract
Nurse managers’ workload is considered overwhelming and the resources and support insufficient. Stress from workload has adverse psychological and physical effects and impedes strategic, visible and active leadership. This study aimed to examine nurse managers’ stress from workload and its associations to overall job stress, job satisfaction and practice environment. A survey comprising the Nursing Context Index was administered to 490 nurse managers in Finnish central hospitals. The study was reported using the STROBE statement. The response rate was 42.7% (n = 209). A statistical analysis revealed that almost every fifth nurse manager experienced high stress from workload with connection to higher job stress overall, higher intent to leave the organization, lower job satisfaction overall, personally and professionally, as well as a more negative perception of the practice environment. Nurse managers’ jobs require adequate resources, clear division of work and better empowering structures.
Introduction
Nurse managers deal with a heavy workload as one of the most frequent stressors.1–3 Nurse managers’ volume of tasks and the stress that comes from this workload is so overwhelming that there is very little time or energy for strategic, visible and active leadership that emphasizes organizations’ values, objectives and mission to the nursing workforce.4,5 This causes a vicious cycle, as nurse managers play an important role in fostering a productive and supportive work environment that in turn decreases nurses’ job stress and turnover intentions.4,6 Nursing turnover adds to the managers’ workload via several disruptive consequences, such as recruitment challenges, loss of experienced workforce, morale and productivity as well as decreased patient satisfaction. 7
A large number of nurse managers are retiring 8 and others are planning to leave their jobs due to burnout and dissatisfaction. 9 Recruiting and retaining trained and experienced nurse managers is also a major challenge, as it appears that the next generation of nurses is reluctant to lead. 10 The training of a nurse manager takes years, since experience is the primary mechanism to build competency in nursing management. 11 Thus, nurse managers’ stress from workload needs to be addressed in order to retain not only the managers themselves but also our trained and experienced nursing workforce.
The work of nurse managers has been of interest from several viewpoints in Finland. Those have been e.g. their competence,12,13 their wellbeing, 14 their job content, 15 how appreciative is their way of acting,16,17 and, further, how they perceive organizational social context 18 and their workplace culture. 19 Lately also their efforts to support evidence-based nursing has been studied.20,21 However, nurse managers’ workload has not especially been investigated.
In Finnish hospitals the nursing management hierarchy typically includes nursing directors (upper level), head nurses (middle level) and assistant head nurses (first level), forming a three-level structure that is typical to any large organization. 22 The titles of nurse managers, however, may vary in each hospital. In this study the term nurse manager refers to a person who has managerial tasks, working in any of these levels.
Background
Nurse managers are moderately stressed,1,2 very stressed 23 or even burned out. 24 Workload1,2,25 and related time-management challenges are major causes of stress.1,24 The volume of tasks that nurse managers are required to handle is overwhelming, and results in managers feeling overloaded and struggling to keep up with the pace. 25
Nurse managers’ work seems like a juggle between several competing priorities, countless interruptions and pressure building expectations from many directions.1,26 Operating in the middle management level can feel like being caught between two fires. 27 The job comes with a stressful demand to be available and responsible for the unit around the clock, which may lead to a sense of imbalance between work and social life.25,28,29
Nurse managers spend a vast amount of time and effort on managing understaffing as a result of staff sick leave. Managers may even fill in themselves if no nursing staff is available, and the managerial work that could prevent the issue in the first place is therefore postponed.1,30 Overall, the lack of proper resources causes stress for nurse managers. 2 Stress from role overload emerges when the role expectations grow bigger than personal skills and resources.23,29 The amount of managerial tasks per nurse manager can increase as a result of healthcare reform that aims to cut back on workforce expenses.5,28 Nurse managers may end up feeling overwhelmed with too many things to do, for too many people in too little time – often without the support they need.25,28 The most pervasive tasks end up taking time and resources from other important tasks such as creating a good working environment, yearly appraisal interviews with the staff and motivating and following up on nurses in daily care. 5
Nurse managers experience stress from their financial accountability. 2 They are expected to monitor the budget and stick to it, often without comprehensive training. 31 Financial insecurity causes worrying, and continuing limitations in the resources challenge nurse managers to balance between finances, quality of care and securing the continuity of operations.26,28 Lack of information and being left out of the decision-making process cause frustration and sense of not being good enough. 27 This relates to the nurse managers’ experience of having responsibility but no power. 24
Workload as a major cause of nurse managers’ stress has several adverse consequences regarding a person’s wellbeing. It has been studied to have a positive association with distress, fatigue, emotional exhaustion, strain, depersonalization, depression, even physical symptoms and global health problems.32–34 Extensive workload may expose nurse managers to a high effort–reward imbalance that is also highly associated with depressive symptoms. 35 According to a previous study, managers’ workload positively predicts the tendency to work excessively, which in turn provokes work–family conflict and lack of psychological detachment.25,36 Work-to-family conflict and family-to-work conflict, as well as role ambiguity and role conflict, are work stressors that are all positively associated with the sense of workload. 33
One might wonder why nurse managers stay in these stressful positions. Interestingly, the nurse managers feel that they also have power and autonomy to solve the issues that emerge in their units. The influence that they have on the staff and patient care outcomes encourage them to stay in their positions.37,38 However, workload is negatively related to a sense of personal accomplishment. 33 Workload should be considered as an important part of retaining managers, as workload is significantly associated with job satisfaction11,25 and intent to leave one’s current position.9,11,33 Thus it is pivotal to examine nurse managers’ stress from workload and its associations to overall job stress, job satisfaction and practice environment in central hospitals.
Methods
This study used a quantitative cross-sectional study design in which the data were collected via an electronic survey and analyzed using descriptive statistics. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement was used as a guideline to report this study (see Appendix S1 in the online supplementary material).
Participants
The participants in this study were selected using stratified sampling within all of the 16 central hospitals in Finland. A central hospital exists in each hospital district. Specialized medical care is provided by hospital districts. The provision of the most demanding medical operations is centralized on the national level to the five university hospitals. 39 The central hospitals were listed by their population size, ranging from 29,000 to 251,000 people. The hospitals were then divided into groups by their population, with not more than 50,000 people range in population within one group. Two hospitals from each group were selected for the study, also ensuring that from each of Finland’s five specific catchment areas at least one hospital was selected and that the hospitals were located geographically as evenly as possible across Finland. One of the central hospitals was excluded because of its exceptional geographical location, language limitations and the lack of a specific catchment area. From the eight selected hospitals all nurse managers in all levels of the organization were invited to participate in the study (N = 490).
The organizational and leadership structures, as well as the titles of nurse managers, had some variation among the participating hospitals. The contact person of each hospital was informed of the inclusion criteria; that potential respondents should be those who held the role of first-level nurse manager such as charge nurse or assistant head nurse, or middle or upper-level nurse manager such as head nurse, nursing director or a similar role with managerial tasks. With this instruction the contact person decided the recipients of the study invitation.
Data collection
The participating hospitals were asked to determine their contact person for this study. The only requirement for the contact person was that they had the means and time to forward the survey to all nurse managers in the hospital. In some hospitals the contact person was the chief nursing director or chief of nursing development, but some hospitals named a nursing director, a secretary or a research coordinator as a contact person. A cover letter containing information about the study and a link to an electronic survey was delivered via email to the contact person, who then forwarded it to all nurse managers in the hospital. Two reminders were sent within the data-collection period. A total of 209 responses were received, yielding a response rate of 42.7% after a four-week data-collection period in each hospital.
Measures
The electronic survey comprised the Nursing Context Index (NCI) instrument in addition to questions about the participants’ demographic and occupational characteristics. The NCI, developed by Slater et al., 40 contains 78 items that generate three constructs and 19 factors: overall job stress, which contains nine factors (of which one is stress from workload); overall job satisfaction, which contains four factors and overall practice environment supportive of person-centered practice, which contains six factors. Items were measured using a seven-point Likert scale. The main outcome variable is stress from workload containing five items. In these items, the participant is asked to estimate how often they, for example, have felt too much pressure at work during the last week, ranging from never to always.40,41
The NCI instrument was originally developed to be used among nurses, and this was the first study in which it was used among nurse managers. The internal consistency of the constructs was verified using Cronbach’s alpha coefficient, and the values ranged from 0.87 to 0.89 in two constructs (job satisfaction and practice environment) and from 0.63 to 0.95 in the 19 factors of job stress, job satisfaction and practice environment. The alpha values corresponded with the previous studies using the same instrument40,42,43 and were considered adequate. 44 The electronic survey was piloted prior to use with four nurse managers and no changes were seen as necessary or applicable, as some of the feedback regarded the validated instrument.
Data analysis
Quantitative data were analyzed statistically with SPSS Statistics 26. Sum variables were formed in line with the instructions of instruments. The data were examined and found to deviate from normal distribution. Therefore median values (Md) and lower (Q1) and upper quartiles (Q3) were reported and statistical testing was undertaken using non-parametric Mann–Whitney U and Kruskal-Wallis H tests. Probability values <0.05 were considered as statistically significant. Nurse managers’ job satisfaction and job stress were interpreted as low with scores lower than three, moderate with scores from three to five and high with scores higher than five. Practice environment was interpreted as not person-centered with scores lower than three, neutral with scores from three to five and person-centered with scores higher than five. High scores in the construct intention to leave were interpreted according to the NCI instrument as positive perceptions of the practice environment and as having little intention to leave the organization.
Results
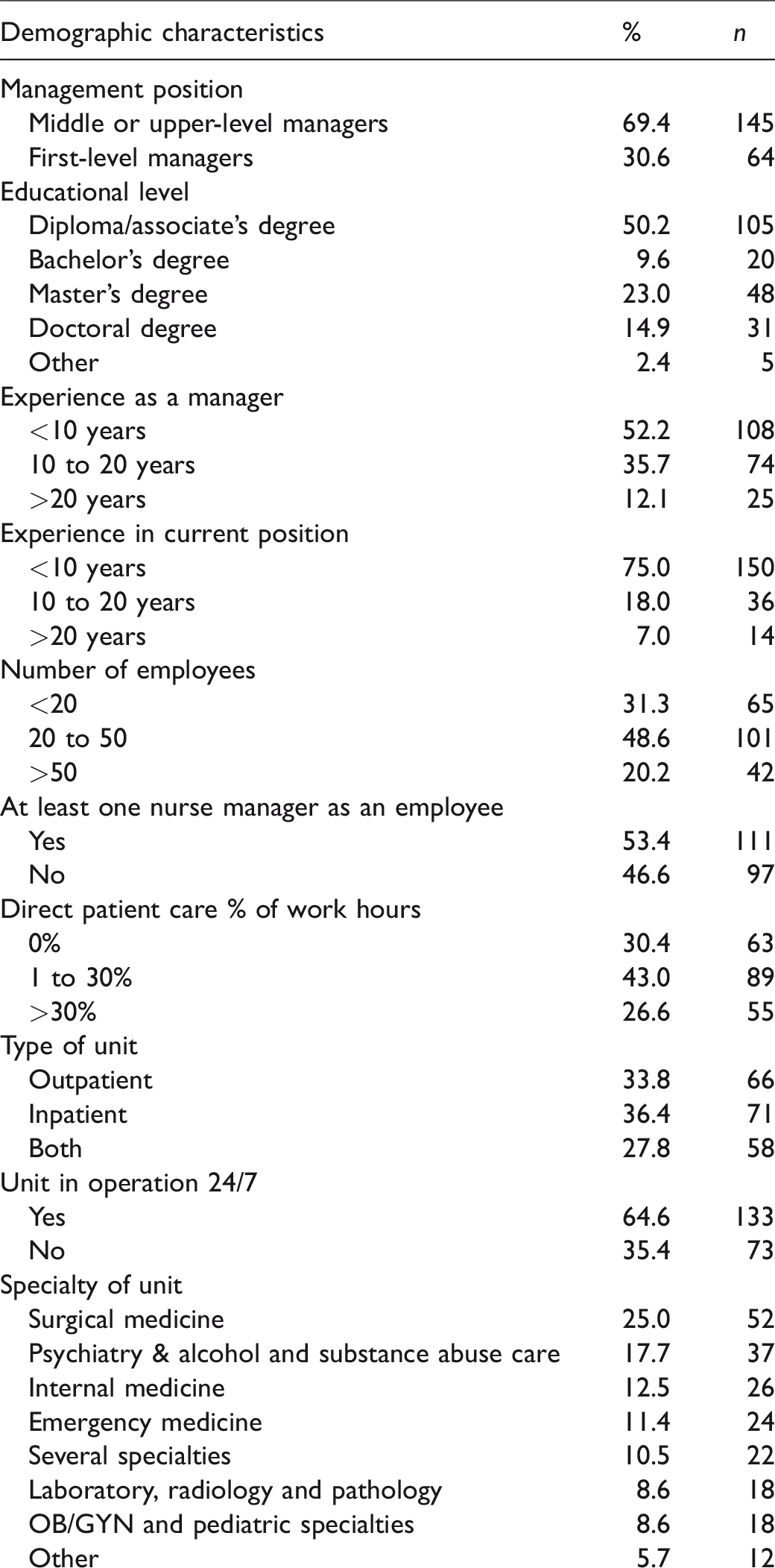
A total of 209 completed questionnaires were received. The respondents were 53 years old on average (Q1 = 47, Q3 = 57), the youngest being 32 years and oldest 63 years old. Of the respondents, 95% were female. The majority (69%) were middle or upper-level managers, such as head nurses and nursing directors, although other titles with similar job descriptions were also in use. Of the respondents 31% were assistant head nurses, charge nurses or other first-level nurse managers (Table 1).
Over half of the respondents (52%) had less than 10 years of experience as a manager. Little over one third (36%) of the respondents had 10 to 20 years of experience and only 7% had more than 20 years of experience as a manager. The average number of employees that a nurse manager oversaw was 28. Approximately one half of the respondents (49%) oversaw 20 to 50 employees, every third (31%) fewer than 20 employees and every fifth (20%) more than 50 employees. Approximately every other nurse manager also supervised another nurse manager (53%, Table 1).
One half of the respondents (50%) had a diploma or associate’s degree as their educational level; 10% of the respondents had completed a bachelor’s degree, 23% had a master’s degree and 15% had a doctoral degree. A few respondents reported complementing their diploma or associate's degree with studies in management (Table 1).
Nurse managers’ stress from workload and its connection to factors of job stress, constructs and factors of job satisfaction and practice environment
Nurse managers reported moderate stress from workload (Md 4.0, Q1 3.2, Q3 5.0) with the highest scores given to the job entailing too much pressure (Md 5.0, Q1 3.0, Q3 6.0). Overall, moderate scores were also given to other factors, such as always being in a hurry to complete one’s work (Md 4.0, Q1 3.0, Q3 5.0) and being asked to do too much (Md 4.0, Q1 3.0, Q3 5.0, Table 2).
Nurse managers’ demographic characteristics.
Nurse managers’ stress from workload.
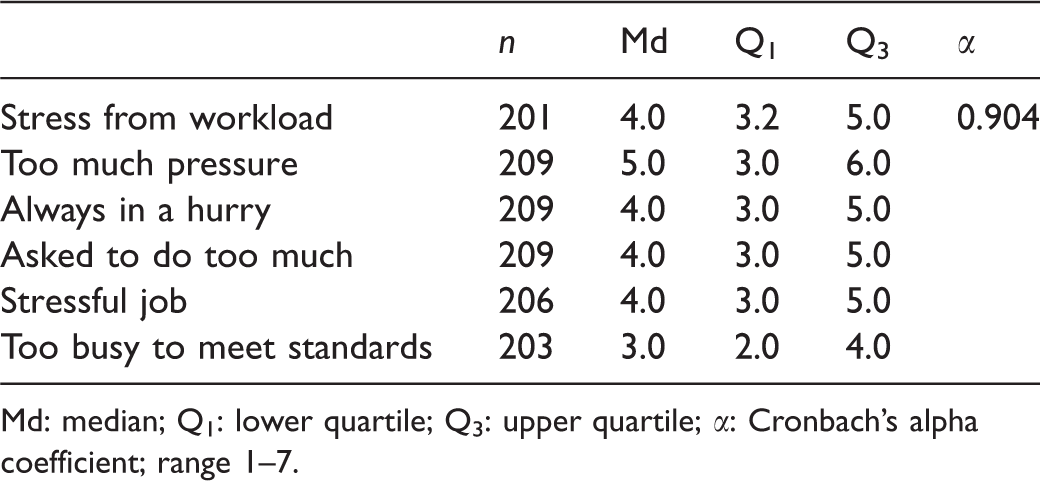
Md: median; Q1: lower quartile; Q3: upper quartile; α: Cronbach’s alpha coefficient; range 1–7.
However, every fifth (20%, n = 40) nurse manager experienced a high level of stress from workload, over half (59%, n = 119) moderate and just over a fifth (21%, n = 42) low. Nurse managers who reported experiencing high levels of stress from workload also reported higher levels of stress in every other attribute than nurse managers who experienced moderate or low levels of stress from workload. High levels of stress from workload were also associated with lower levels of overall job satisfaction (p < 0.001), personal satisfaction (p < 0.001) and professional satisfaction (p < 0.001, Table 3).
Association between stress from workload and the other constructs and factors of the NCI instrument.
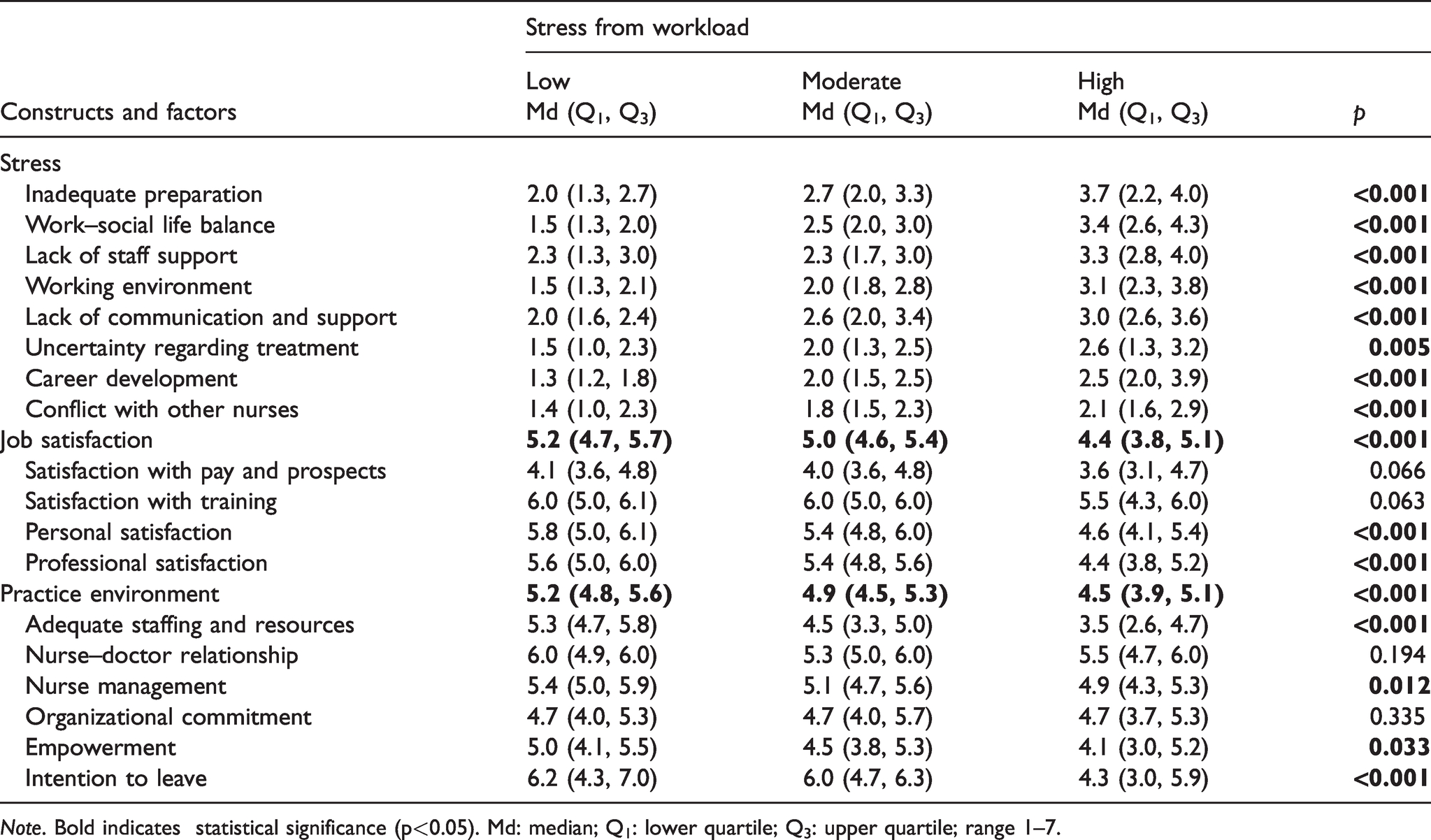
Note. Bold indicates statistical significance (p<0.05). Md: median; Q1: lower quartile; Q3: upper quartile; range 1–7.
High level of stress from workload was associated with a more negative perception of overall practice environment (p < 0.001), nurse management (p = 0.012), empowerment (p = 0.033) and staffing and resources being adequate (p < 0.001). Those nurse managers who experienced high levels of stress from workload reported significantly lower scores in the practice environment’s attribute of intention to leave (p < 0.001), which indicated a stronger intention to leave than nurse managers who reported moderate or low levels of stress from workload. No statistically significant associations were found between stress from workload and respondents’ demographic characteristics.
Discussion
In this study, nurse managers’ stress from workload was overall reported as moderate. In an earlier study, nurse managers’ stress from workload has been reported as being on a high level. 1 Studying nurse managers’ stress from workload can be problematic. Nurse managers who are under a lot of pressure and struggle to manage their work are very likely to not prioritize answering surveys. The response rate of this study was quite high (42.7%) but it is possible that the nurse managers with the most stress from workload did not actually participate in this study.
The highest scores within stress from workload were given to the job entailing too much pressure, and moderate scores to other factors such as always being in a hurry to complete one’s work and being asked to do too much. Earlier studies support this finding, since time pressure has been reported as one of the highest stressors in nurse managers’ jobs 1 and nurse managers often have so many projects going on that they couldn’t possibly achieve their goals before another project is already presented. 25 The descriptions of nurse managers’ daily work include a wide range of managerial work, administrative and financial duties as well as clinical work and other duties. 45 Since the stress level was moderate in this study, it is possible that nurse managers sometimes enjoy the variation in their work and do not experience it as an adverse side of the job. The challenge of being asked to do a lot may act as an incentive to achieve more. It is also possible that the difference in the stress experience between this study and previous studies could be explained by the difference in the average age, that could in turn indicate experience in nursing and as a nurse manager. The average age of respondents in this study was 53 years, which was a little higher in previous studies.1,23 Excessive workload may especially target novice nurse managers on the qualitative side of workload since they do not necessarily yet have the skill set to tackle all kinds of problems efficiently. The tasks end up taking so much time and emotional and physical energy that one does not even have the time or possibility to gain new resources or develop skills. 33 However, stress from workload did not yield a statistically significant difference with any of the demographic or occupational characteristics in this study.
In this study, it was discovered that a fifth of nurse managers experienced a high level of stress from workload. Interestingly, nurse managers who reported experiencing high levels of stress from workload also reported higher levels of stress in every single other job stress factor than nurse managers who experienced moderate or low levels of stress from workload. These findings do not explain the direction of the association. For instance, it could be that stress from workload causes stress from work–social life balance or that stress from the lack of communication and support causes stress from workload if one feels unsupported in handling all of the work. Previous studies have also discovered that trait negative affectivity has a positive relationship with job stressors such as workload. A nurse manager who has high stress from workload and every other stress factor, could also be high in negative affectivity and unintentionally create stressful work situations or perceive work environments as threatening even when they actually are not. 33 Nevertheless, nurse managers who experience high levels of stress from workload are more likely to leave their jobs than nurse managers who reported moderate or low levels of stress from workload. It is therefore vital that we find ways to decrease their stress levels.
High level of stress from workload was associated with lower levels of overall job satisfaction, personal satisfaction and professional satisfaction. This finding is consistent with a previous study that found a correlation between quantitative workload and job satisfaction. Like job stress, there was a connection between job satisfaction and negative affectivity, but also with general health, autonomy and variety. 46 This indicates that by offering freedom in decision-making, variety in managerial tasks as well as training in enhancing one’s self-management and wellbeing, it is possible to affect job satisfaction directly and stress from workload indirectly. Even though the nurse managers with high stress from workload were slightly less satisfied with training as well as pay and prospects, the difference was not statistically significant.
High level of stress from workload was associated with a more negative perception of overall practice environment and in the factors of nurse management, empowerment and adequate staffing and resources. A possible explanation for the more negative perception of nursing management among the nurse managers who experience high stress from workload could be the span of control. The number of full-time equivalents (FTEs) that nurse managers oversee varies a lot. In this study the average number of employees per manager was 28, but every fifth nurse manager had more than 50 employees. With this number of employees the administrative tasks tend to pile up. The manager role might have some work built in that is not even specifically a nursing function. In that case the nurse manager could benefit from an administrative assistant or at least an assistant nurse manager, especially when the span of control is large.25,47,48 In a previous study, ward managers reported that after administrative assistants took tasks from the manager’s hands, visible and active leadership was increased and both key performance measures and staff motivation were improved. 47 Instead, often nurse managers are offered more responsibilities with the same performance expectations and without additional resources or any tasks being taken away. 25
Health service administrators should assist nurse managers in transformational and participative leadership styles, since they could be beneficial to both nursing staff and the nurse manager. These leadership styles have a significant relationship with nurses’ turnover intention by engaging the nurses to take part in the decision-making and resolving problems in the workplace autonomously. 6 At the same time the need for nurse managers to take active part in solving problems decreases, saving some time in the process.
Empowering structures would require opportunities for peer and superior support to a nurse manager, since the sense of workload is negatively related to general social support and support by one’s supervisor as well as co-workers. 33 Excessive workload may prevent one from fostering interpersonal relationships in the workplace 33 and nurse managers’ jobs have been described as very lonely and lacking in support since there often is not enough – or any – time for it. 45 According to a previous study, insufficient empowerment is one of the most important factors for managers intending to leave. 34
The connection between stress from workload and a more negative perception of adequate staffing resources is supported by the fact that nurse managers spend an enormous amount of time managing staff shortages. 30 According to a previous study, staff shortages were also one of nurse managers’ biggest stressors. 1 Sufficient human or fiscal resources is one of the most important factors that makes it or breaks it for managers’ recruitment or turnover, as it highlights the manager’s ability to ensure high-quality patient care.34,48
Study limitations
The data for this study were collected in spring 2016. In a constantly changing world and healthcare field this forms a limitation to this study, as every set of data is a reflection of its own time. Although, from the point of view of an active nurse manager of today it seems as nothing has changed. The workload still is the one aspect of the job that causes the most stress – every day.
Previous studies indicate that nurse managers are at least moderately stressed or even on the verge of burning out,1,23,33 when this study reported that nurse managers stress levels were low. The questionnaire includes statements that can be considered not as applicable in describing the work context of nurse managers as that of nurses. Partial non-response was detected more often in statements in which the patient was mentioned than ones in which the patient was not mentioned. Also, the dimension of job stress did not include statements about financial control and following a budget, constant measuring of operations, role distress and overload and round-the-clock responsibility, which are important stressors for nurse managers according to previous studies.28,29,33 It appears that the instrument could be further developed and tested to better describe nurse managers’ work context. However, the construct of workload was, in the researchers’ opinion, applicable to describe the nurse managers’ stress as it did not focus on statements about direct patient care.
Concerning the data collection, some amount of variation existed among the selected hospitals and what they included in the central hospital activities, thus impacting how many nurse managers existed. However, the ultimate goal was to reach all nursing managers in the selected central hospitals. Central hospitals, in addition to university hospitals of the hospital districts, are responsible for the most demanding medical operations and specialized medical care services are provided at hospitals in Finland. Specialized medical care refers to examinations and treatments, such as surgeries, provided by medical specialists at hospitals. 39 This study included nursing units from a range of different specialties as seen in Table 1, and is therefore also generalizable to various nursing settings.
Conclusion
Nurse managers working nationwide in Finnish central hospitals reported moderate levels of stress from workload. However, every fifth nurse manager experienced a high level of stress from workload, which is associated with increased job stress in numerous aspects, decreased overall job satisfaction and negative perception of practice environment. This study reveals a critical need to identify those around 20% of nurse managers who experience high levels of stress from workload in order to support and retain them in their positions and to enhance their satisfaction.
Nurse managers’ perceptions of workload should be taken into consideration when designing leadership structures and dividing work in certain organizations. Nursing management needs adequate staffing and resources, clear division of work and better empowering structures as a foundation from which to face the future challenges of healthcare reform. Stress from workload could be addressed by enhancing nurse managers’ personal and professional satisfaction by enabling a better work–life balance and offering training in self-management and wellbeing.
Ethical considerations
Approval from a research ethics committee is not required for this kind of survey in Finland according to the Medical Research Act. 49 Appropriate study approvals were obtained from all participating hospitals before conducting the survey. The authors also obtained a permission to use the Nursing Context Index instrument. The survey was completed anonymously, and written consent forms could not therefore be collected. The respondents were provided with a comprehensive information letter about the study. After that, answering the survey was considered as informed consent to participate in the study. The anonymity of the respondents was also protected throughout the study, for example by grouping the respondents if there were few respondents in certain healthcare units or demographic characteristics. The data are stored on a password-protected hard drive by the head researcher as long as it is still needed in the research project. When there is no further use for the data, they will be appropriately destroyed.
Supplemental Material
sj-pdf-1-njn-10.1177_20571585211018607 - Supplemental material for Connection between nurse managers’ stress from workload and overall job stress, job satisfaction and practice environment in central hospitals: A cross-sectional study
Supplemental material, sj-pdf-1-njn-10.1177_20571585211018607 for Connection between nurse managers’ stress from workload and overall job stress, job satisfaction and practice environment in central hospitals: A cross-sectional study by Karita Jäppinen, Mervi Roos, Paul Slater and Tarja Suominen in Nordic Journal of Nursing Research
Footnotes
Acknowledgements
We thank Professor Brendan McCormack for his valuable comments regarding the Nursing Context Index (NCI).
Author contribution
KJ, MR, TS; Data collection: KJ; Data Analysis: KJ, MR, TS; Manuscript preparation: KJ, MR, PS, TS; Manuscript review: KJ, MR, PS, TS. All authors have approved of the final version of the manuscript being submitted.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.