
Abstract
During rehabilitation, professionals and patients experience difficulties addressing complex issues. In a hermeneutical approach we examine how the ICF model can capture the complexity of the rehabilitation process using secondary deductive content analysis of transcripts from a previous interview study in line with COREQ. When focusing on interactions, the ICF model captures the complexity of individuals’ issues in a convincing way. Three themes were identified: ‘The influence body function, activity, participation and environment have on an individual’s ability to handle daily tasks of personal importance’, ‘The influence the environment in combination with body function, activity, and personal factors have on an individual’s ability to maintain their social roles’, and ‘The influence personal factors and body functions have on an individual’s confidence in participating in activities they like’. The findings show that the ICF model could provide a useful tool to facilitate communication regarding individuals’ complex issues that are often neglected.
Keywords
Introduction
This article explores how the International Classification of Functioning, Disability and Health model (ICF) 1 can capture individuals’ complex issues during rehabilitation and we discuss how the ICF model can facilitate communication between professionals and individuals during rehabilitation.
Background
Rehabilitation following severe injury such as traumatic spinal cord injury (TSCI) requires that individuals find a way of living with their changed body functions, restricted activities, limited participation as well as the psychosocial consequences of the injury.2,3 Therefore, both early hospital and long-term community rehabilitation are offered to optimize their functioning, psychosocial well-being and reintegration into society.4,5 The complexity of an individual’s situation requires comprehensive communication about the individual’s specific issues.2,6 Despite efforts at optimizing this, individuals encounter various problems in their daily lives and face barriers in the environments in which they live; issues which are rarely addressed in communication with professionals.7–9 These problems and barriers potentially affect the individual’s psychological adjustment10,11 and sense of stress, 12 and they increase the risk of depressive psychological morbidity. 10 A qualitative study has shown that the process of getting on with life following TSCI proceeds through various phases where the individual learns to live with his or her limitations to achieve quality of life. 13 Facilitating this process includes raising issues such as relationships, goals, priorities and spirituality. 14 Also, perceived control, sense of coherence, self-worth, hope and purpose in life are associated with quality of life following TSCI. 15 Age, education, lifestyles and habits can also influence the rehabilitation process, both positively and negatively.12,14,16 The interaction between these factors makes rehabilitation a unique and often difficult and unpredictable process.2,6,17,18
Previously, we found that individuals with TSCI had difficulties in addressing sensitive issues related to their daily lives, and that, in turn, they were neither understood nor given adequate support.19–21 These findings demand that more attention be paid to approaches taken by professionals in regard to complex issues faced during rehabilitation.
The ICF model describes functioning, disability and health by means of the ICF components; ‘body function’, ‘activity’, ‘participation’, ‘environmental factors’ and ‘personal factors’. 1 The model is attentive to the interactions between these components, may have the potential to capture the complexity of issues that individuals face during rehabilitation, and may be a useful tool in communication. Our previous studies19–21 revealed that complex interactions seemed to add to the problems and barriers that the individuals experienced in their daily lives. Therefore, addressing ICF component interactions could be useful in communication in order to achieve person-centred rehabilitation that meet individuals’ needs. The aim of this study was therefore to examine how the ICF model can capture individuals’ complex issues during rehabilitation following severe injury.
Method
This article takes a hermeneutic approach, interpretating individual interviews in deductive content analysis. The ICF model is used with specific attention to the ICF component interactions. The interviews were conducted in a previous study19–21 and the study was conducted in accordance with the consolidated criteria for reporting qualitative studies (COREQ) 32-item checklist. 22
Participants and setting
In the previous study,19–21 eight interviewees (two women and six men; aged between 27 and 73 years; one complete paraplegia, seven incomplete tetraplegia), signed an informed consent. The interviewees, who had been admitted to The Spinal Cord Injury Centre of Western Denmark, were asked about their expectations, wishes and worries prior to discharge from the rehabilitation centre. At home they were asked about their experiences one month and one year after discharge (Table 1). The recruitment process involved the chief physician and the charge nurse at the rehabilitation centre who evaluated the hospital’s list of patients admitted in the study period. Together with the interviewer (BBN) they identified nine patients who were invited to participate, and eight accepted.
Interview guide used in the original interview study.
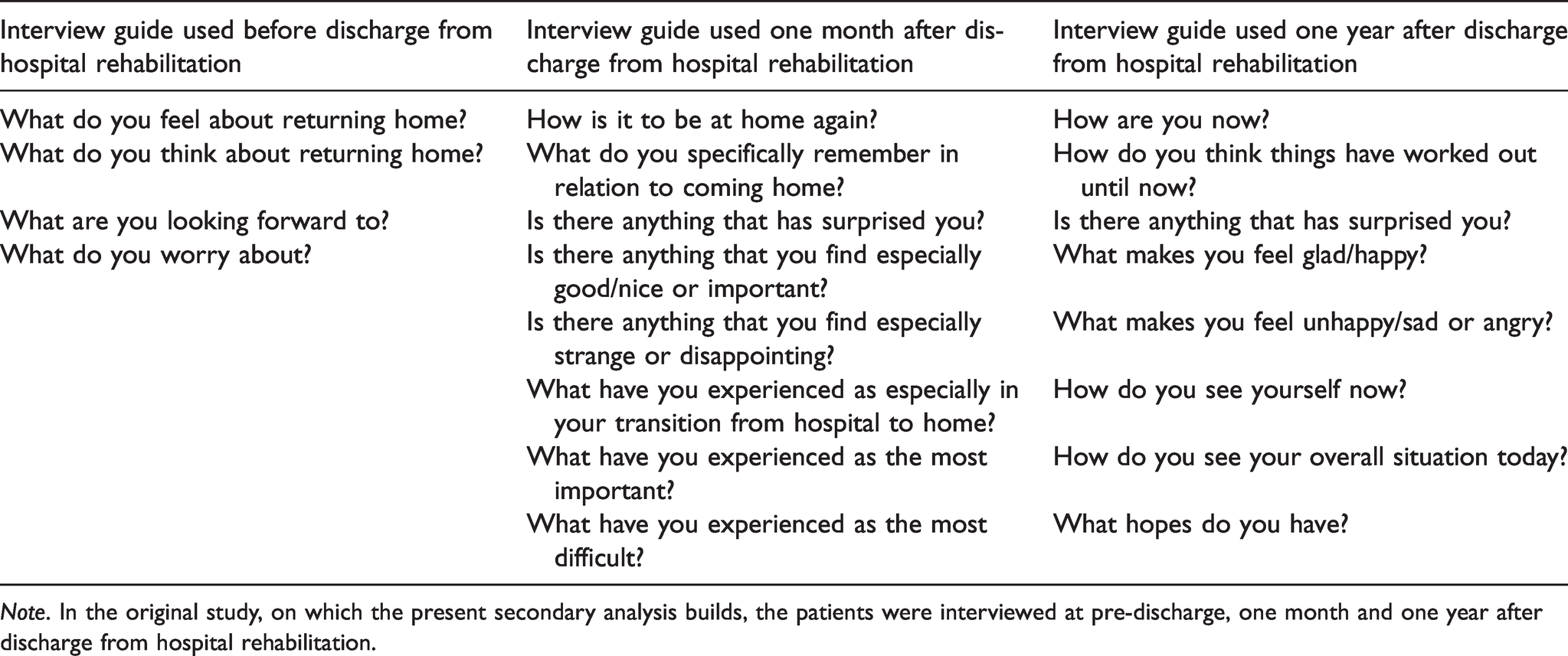
Note. In the original study, on which the present secondary analysis builds, the patients were interviewed at pre-discharge, one month and one year after discharge from hospital rehabilitation.
Ethics
The previous study was approved by the SCI Centre of Western Denmark and the Danish Data Protection Agency in 2012 (J.nr. 2012-41-1283). This secondary analysis was conducted on the anonymized interview transcripts.
Data analysis
This secondary deductive content analysis of the transcribed interviews was conducted in a constant dialogue among the authors in a three-step process.23–28 Firstly, a coding frame was developed using the ICF model 1 and the definitions of the ICF components, and the data were reviewed for content and coded into these ICF components (Figure 1 displays the ICF model with component interactions and Table 2 the ICF terminology). In this coding process the transcripts were linked to the ICF model using the ICF Core Sets for individuals with SCI, 29 which specify any possible aspect related to spinal cord. The component ‘body function’ is specified by 63 categories, the components ‘activity’ and ‘participation’ are specified by 64 categories and the component ‘environmental factors’ is specified by 41 categories. The fifth ICF component ‘personal factors’ is not included in the Core Sets, therefore this was specified by lifestyles habits, character styles, behaviour patterns, relationships, priorities, values, skills, spirituality, perceived control, self-worth, hope and purpose in life.15,30 Secondly, meaning units were systematically coded from the transcripts using the ICF coding frame. 1 As we focused on revealing the ICF component interactions from the transcripts, in this context a meaning unit was defined as the individual’s descriptions of situations or events in daily life, where ICF component interactions can be identified. Thirdly, the coded meaning units were condensed into three themes describing ICF component interactions and how they influence a person’s life.
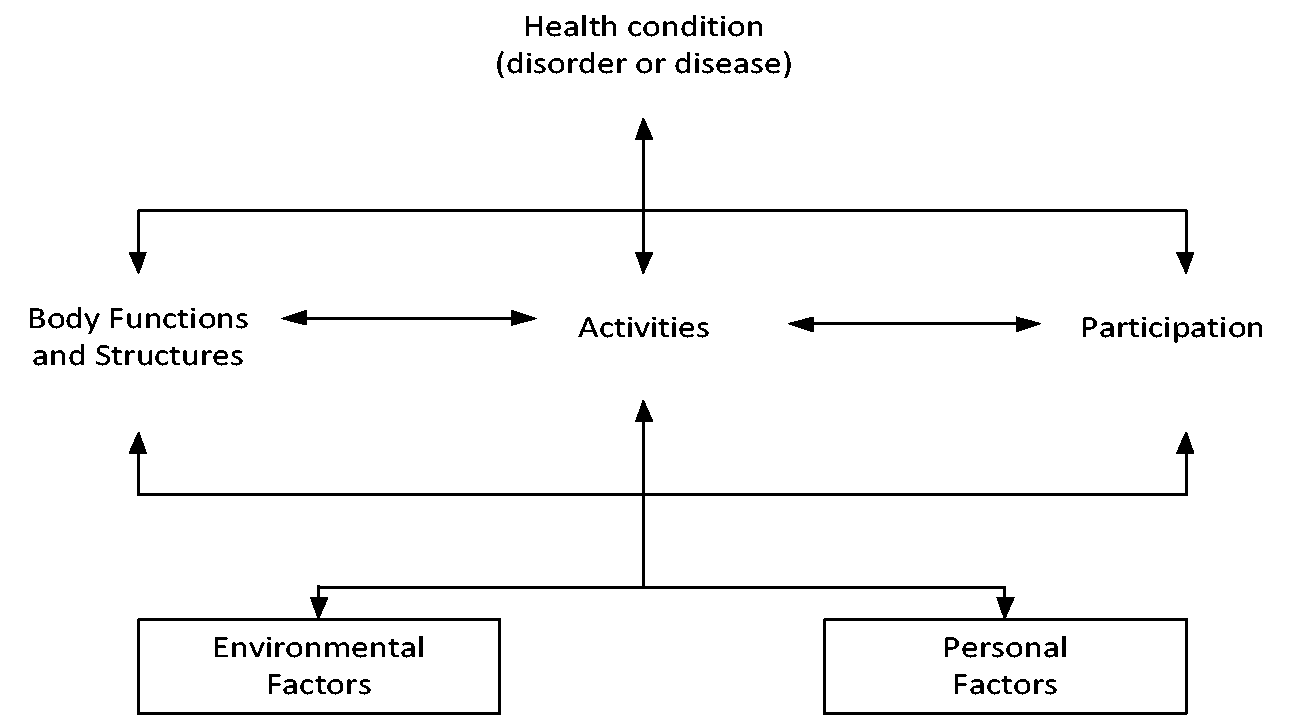
The ICF model.
The ICF model: terminology.
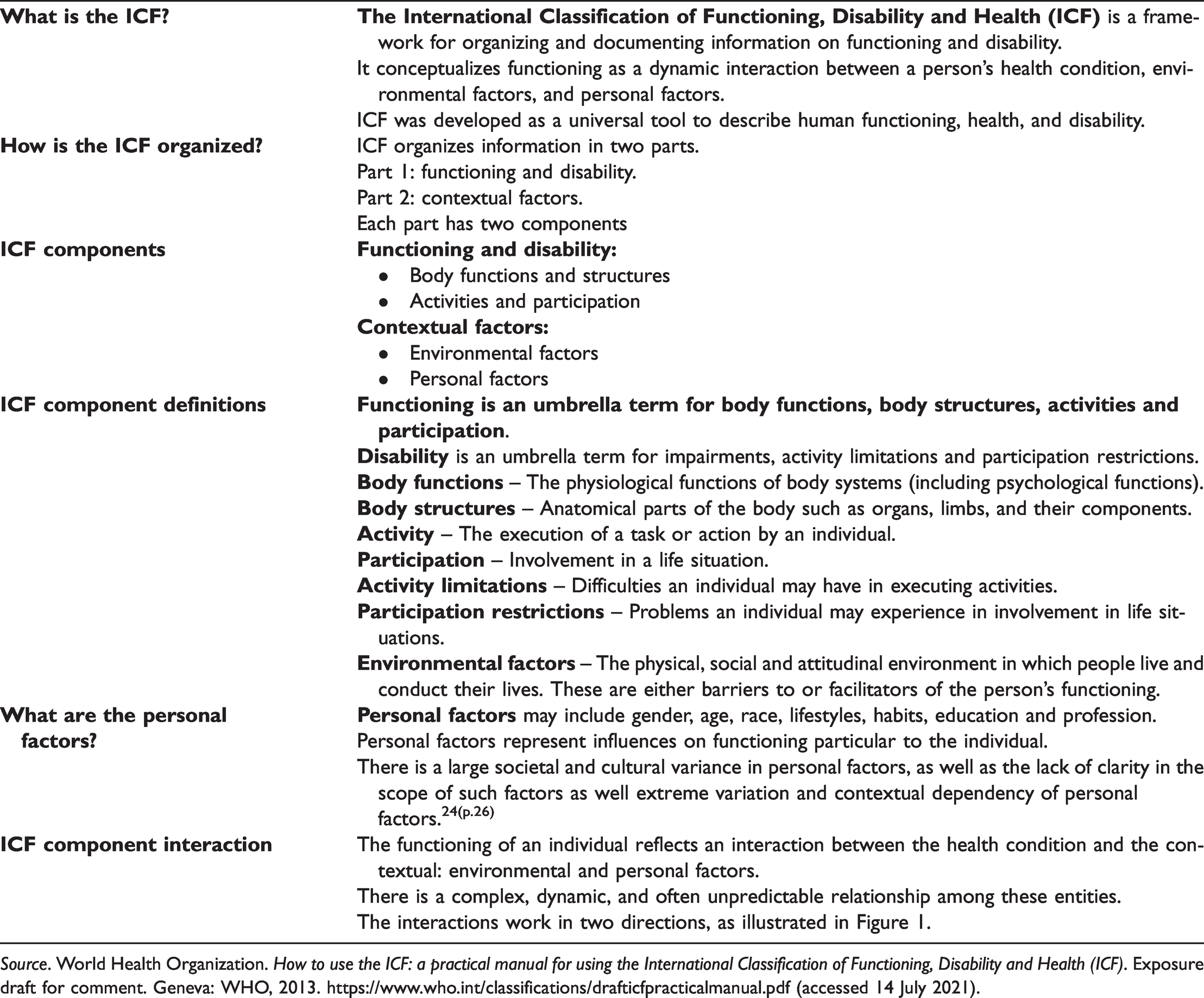
Source. World Health Organization. How to use the ICF: a practical manual for using the International Classification of Functioning, Disability and Health (ICF). Exposure draft for comment. Geneva: WHO, 2013. https://www.who.int/classifications/drafticfpracticalmanual.pdf (accessed 14 July 2021).
Findings
In the various types of ICF component interactions that appeared from the transcripts, specifically, dimensions of the component ‘personal factors’ played an important role. Three themes describing ICF component interactions that influence individuals’ lives were identified: ‘The influence body function, activity, participation and environment have on an individual’s ability to handle daily tasks of personal importance’, ‘The influence the environment in combination with body function, activity, and personal factors have on an individual’s ability to maintain their social roles’, and ‘The influence personal factors and body functions have on an individual’s confidence in participating in activities they like’.
‘The influence body function, activity, participation and environment have on individuals’ ability to handle daily tasks of personal importance’
Following the injury, the individuals experience a changed and challenged overall life situation. Although they are thankful due to their improvements, many daily tasks have become difficult to perform. The changed body functions in terms of impaired hand, arm and leg use, paralysis, pain, and spasm, affect activities, such as moving around, washing, dressing, eating and doing housework. These physical impairments can result in restricted activities and limited participation, which is experienced as problematic especially because individuals become incapable of taking care of daily tasks of personal importance in their lives. We found that the complex interactions between body function, activity, participation and environmental factors are influenced by personal factors and that these interactions all together influence individuals’ lives. Personal factors such as prior roles, values and character styles can explain which daily routines and tasks the individuals experience as specifically important, necessary, and valuable. I am self-sufficient … due to intensive training, there is a life for me, too … My neurogenic pain and spasms – they are what I struggle with … The worst thing for me is inserting the car key and turning the key. There are a lot of things I can’t do at home during the day … not turn on the heating … nor switch on the lawnmower … This is a problem … I have always been hardworking, doing what is necessary … It should not be that my partner has to take care of me when she is at home from work. It will lead to a breakdown. (One year after discharge. Male in late fifties, incomplete tetraplegia due to fall. This quotation illustrates the coding using the ICF model in Figure 2). The categorization into the ICF components, including interactions.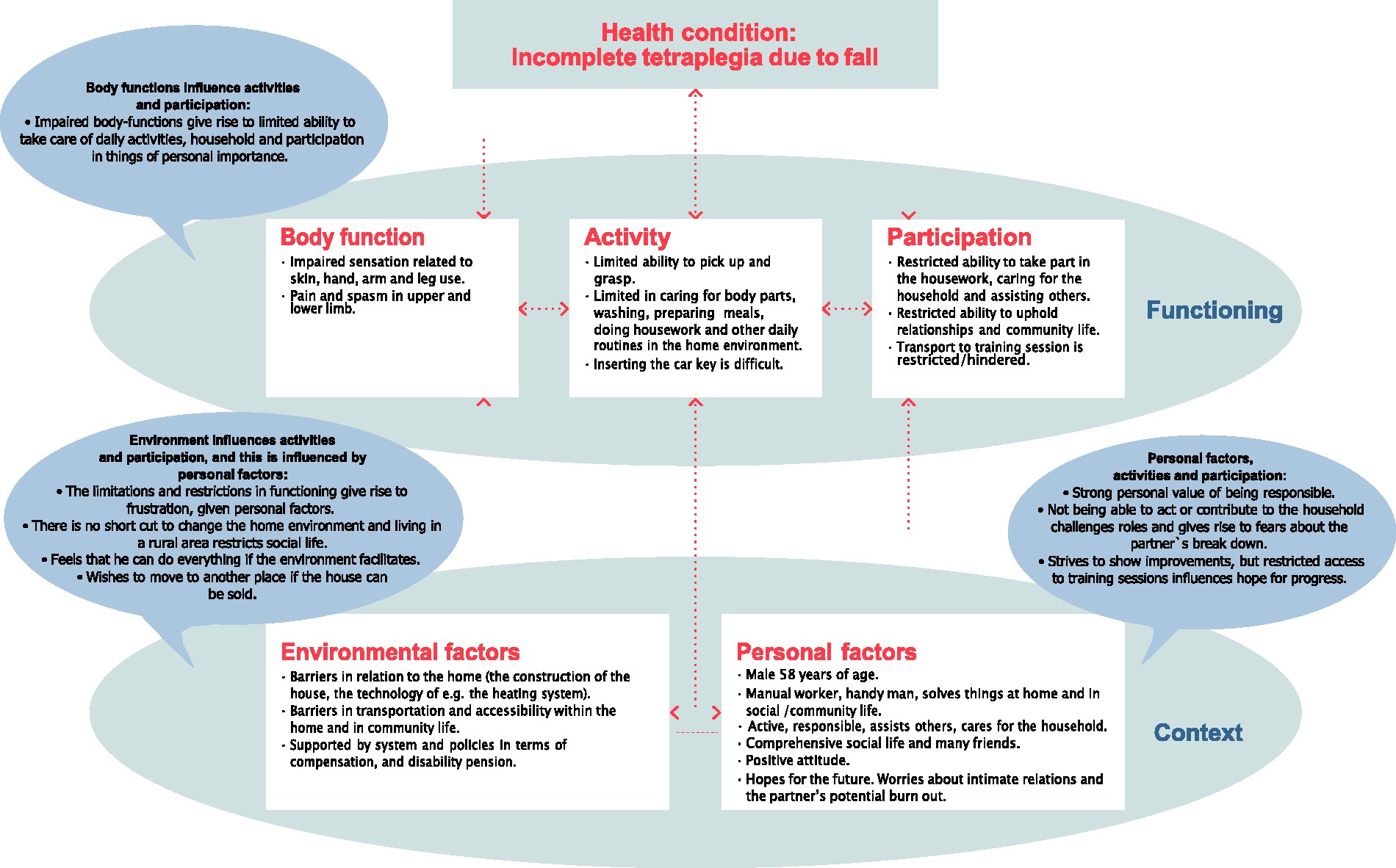
Not being able to take care of personal issues of importance adds to the sensation of dependence and being a burden. Also, it adds to the fear that the individual’s impairments can lead to relationship breakdown and family breakup, as illustrated in the quotation above. Therefore, despite the individual’s motivation and hope they also experience fear and sorrow. The complex ICF component interactions mean, for example, that living in a rural area and not being able to insert the car key and drive can impede participation, e.g. in training sessions. Participation in training gives hope for progress and is an issue of great personal importance and a necessary and valuable task during rehabilitation. By training, the individual demonstrates to relatives his/her eagerness to achieve improvement and independence, which is crucial in order to keep up with usual family structures. Therefore, participation in training becomes of utmost personal importance. The findings revealed that personal factors explain how the ICF component interactions influence individuals’ lives. Sensitive personal issues appear in the individuals’ descriptions of daily situations and events, e.g. how they experience their difficulties contributing to the household as they used to and what this means to them. Thereby, the personal factors such as personal values of being responsible and striving to show improvements and independence appears.
‘The influence the environment in combination with body function, activity, and personal factors have on an individual’s ability to maintain their social roles’
Following the injury, the individuals’ social role maintenance becomes challenged. Impaired ability to sit, stand, walk, bend, lift, and carry means that many daily routines, e.g. taking care of children, are difficult and the role as a parent can be threatened. Also, sadness and decreased energy level threaten usual roles. The individuals deeply wish that they will be able to do what is necessary and reasonable and thereby live up to the expectations of the professionals in the community and their relatives, as well as their own expectations. However, they worry about whether they will be able to maintain their social roles, e.g. as a responsible husband, wife, parent and citizen. Also, they worry whether the community professionals who assess their case will understand their complex situation. Therefore, the community professionals can become either a supporting or a non-supporting environmental factor depending on their ability to understand the complex ICF component interactions that influence the individual’s situation and social roles. Many things may seem straightforward from the outside, but the individual’s capability to do what may seem reasonable is not easy. This generates a fear of not being able to live up to social norms. How individuals experience this is influenced by personal factors such as self-worth, hope and purpose in life. The interactions between the environment, body function and activity can impact self-worth as a parent or partner. Also, individuals express worry that professionals may condemn them as demanding and irresponsible. This is problematic as the individuals value being responsible, loving and engaged parents, partners etc. Moreover, the individuals value being responsible citizens, who strive for independence and who are not too demanding in terms of asking for practical and economic support from the community. If impaired body function, restricted activities and personal factors are combined with an unsupportive environment, usual social roles are especially challenged. I am very thankful that I can walk again and manage the pain … I really try not to worry … I hope there will be a safety net at home. It is important that I have a relationship of trust to the community, so that I can reach out if I need it … I can manage the injury, but the mental issues are much more difficult for me. I hope that I don’t get the feeling that the professionals think that I haven’t space in my heart for my children and my family. (Before discharge from hospital rehabilitation to home. Woman in mid-twenties with incomplete tetraplegia due to fall)
The individuals deeply hope that their situation post injury, and the sensitive issues it involves, will be understood by others. Thus, individuals’ close relations to others, both loved ones and professionals, become very important. To feel safe, the individuals must be sure that they can reach out for help, and that this will be accepted and understood. However, it seemed to be complicated for the individuals to express how all these sensitive issues were interconnected.
‘The influence personal factors and body functions have on individuals’ confidence in participating in activities they like’
The new life situation following injury involves fear of losing control due to unpredictable and untrustworthy body functions, e.g. the person’s limitation of physical endurance. This gives rise to uncertainty about which activities are manageable during the day. Often it means that the individual withdraws from activities and participation in social life. Avoiding tasks, activities and situations that are deemed to create uncertainty and discomfort or entail a risk is a mean of asserting control. Individuals protect themselves by staying home, although this has implications for their participation. I am not as sparkling as I used to be. I am not as social as I used to be. Well, previously, I was part of the biking club. Every week during the summer, we biked, and afterwards we had a picnic. During winter, we went to the gym and had dinner afterwards. I was there recently to find out if I could still be a part of it. But I don’t think so, although I would like to. I’m afraid … the price is too high. I can’t manage being spontaneous … If I do anything, I must remember what my form is on the day. It is not fun finding out that one is totally exhausted. (One year post discharge. Male in mid-sixties, incomplete tetraplegia related to sports accident)
Staying home and not participating in social activities is well suited for some and straightforward due to their strong self-worth, life priorities and ability to cope with the demands following the injury. On the other hand, some encounter comprehensive struggles coping and keeping control. Complex interactions between body functions in terms of paralysis, spasm and neurogenic pain hinder daily activities such as preparing meals, washing oneself, dressing, and moving around. These comprehensive disabilities and restrictions are under the influence of personal factors such as sense of control, lifestyles habits, behaviour patterns, thoughts, beliefs, relationships and self-worth. In some cases, such personal factors hinder participation in terms of being together with friends and peers. Low self-worth can negatively influence self-confidence, affecting the sense of being accepted and included by friends or peers. Pain, spasms and paralysis keep some individuals at home in bed, where they can feel safe and keep control, although this might add to sadness and loneliness. Outside their home they feel unsafe and have a fear of falling, which is humiliating. For some, the need to keep control can have extreme consequences. Sometimes, I try to get up early, but I can’t. I just can’t … my nerves and those things, they don’t bother, they can’t … It is not that many who come to see me anymore. It must be boring for them … Very often, when my friends go out, I stay at home, because it is too annoying for them … with me. If we do something physical … I used to be with them all the time; we did a lot of things together. I can’t cope with it … then I just do nothing … I do not know what is going to happen … I sometimes stay in bed for 16–17 hours. I don’t want to topple over in the street and things like that. Although it can differ, some days I can walk and some days I can’t … and the wheelchair, oh no, then I will not go anywhere. (One year after discharge. Male late twenties, incomplete tetraplegia due to transport accident)
Thus, personal factors can interact both positively and negatively on the individuals’ rehabilitation processes. A personal mindset bent on keeping control involves a risk that the rehabilitation process can move in the wrong direction and the need for control can be so strong that willingness and courage to participate in social life are hindered.
Discussion
Based on our findings of three examples of ICF component interactions that influence individuals’ lives following severe injury, we discuss how the ICF model can facilitate the communication between professionals and individuals during rehabilitation. Using the ICF model reveals various ICF component interactions between the individuals’ functioning described by the components ‘body function’, ‘activity’ and ‘participation’, and the context described by the components ‘environmental factors’ and ‘personal factors’.1,29 Our findings suggest that the importance of the interaction between the ICF components surface in the individuals’ descriptions of dilemmas, situations and events in daily life.
Our findings show that especially the component personal factors influences how the interactions are experienced and influence individuals’ lives. Post and van Leeuwen and Geyh et al. specify the personal factors used in this context.15,30 Geyh et al. explored the psychologic-personal factors according to the ICF 30 and found 40 personal factors, e.g. quality of life, subjective well-being, life events, perceived stress, locus on control, self-efficacy, coping, lifestyle and personality. Post and van Leeuwen 15 reviewed the literature on subjective well-being in people with spinal cord injury and found that psychological factors such as control, sense of coherence, self-worth, hope and purpose in life play a substantial role. The three themes identified explain the influence of different aspects of personal factors. Personal factors such as lifestyles habits, character styles, behaviour patterns, relationships, priorities, values, perceived control, self-worth, hope and purpose in life interact with body functions, activity, participation and environmental factors in various combinations and have a decisive impact on the rehabilitation process. Our previous study revealed that these personal factors often seem to be neglected in professionals’ communication during rehabilitation.20,21
The findings show that it is essential to communicate personal things of importance and be vocal about how the individual’s environment can support them in doing these things. Ong et al. 31 argue that the professionals may hold misconceptions about what it means to live with the long-term consequences of injury once in the community. Communicating about complex personal issues may seem straightforward; however, it is not that simple, because relatives and professionals often have no idea how complicated simple activities at home and in the community environment can be following severe injury.7–9 However, it is important to communicate about complex interactions involving personal issues as the majority of the people in the long-term context following TSCI experience limitations 32 as well as psychological issues. 10 Therefore, frameworks that can support the professionals are valuable. 31 Using the ICF model in communication can increase the awareness of complex interactions that can uncover the underlying issues of importance.
The idea that various environmental factors can act both as facilitator and barrier is supported by a meta-synthesis of qualitative findings. 32 This meta-synthesis reported that dimensions of environment, e.g. the physical, economic, legal, social and cultural environment, either enable or constrain the quality of life for individuals with spinal cord injury. 32 Further, that personal factors, e.g. self-worth, values and perspective in life are essential for quality of life. Specifically, the importance of communicating how to improve a positive sense of self-worth, and of being capable, valuable and useful. Also, the development of new values and perspectives are important topics in communication in order to achieve well-being. 32 This supports the idea that the ICF model can be useful to initiate communication about an individual’s personal factors, which we find have the potential to impact the rehabilitation process.
The maintenance of social and family roles is a sensitive issue, and the ability to raise such an issue rests on a trustful relationship with professionals. Our findings show that relationships both with loved ones and with professionals are especially sensitive issues. The importance of relationships is in line with findings that, among individuals with TCSI, relationships are of high life priority 33 and an important determinant of life satisfaction. 34 However, social roles are threatened by impairments. When individuals with TCSI are asked about their health priorities, especially hand and arm use and mobility are of high priority as these can compound difficulties in other areas and are associated with independence in many activities. 33 Therefore, the professionals’ communication about interactions is important. In order to communicate effectively, relationships with professionals are important. Using the ICF model can facilitate the professionals’ incentive to address relationships.
Sensitive issues such as personality, behaviour, habits and sense of control are valuable topics to communicate in order to prevent the negative rehabilitation outcomes of, for example, social isolation, depression and abuse. Our findings show that such personal factors can have the potential to steer the rehabilitation process both in a positive and a negative direction. The influence of psychological issues is supported by several studies in the field of spinal cord injury.6,14–16,35 Therefore, approaching personal factors is of importance, even if it seems that being open about thoughts and feelings is difficult. Doing so may improve an individual’s acceptance of their new life situation.
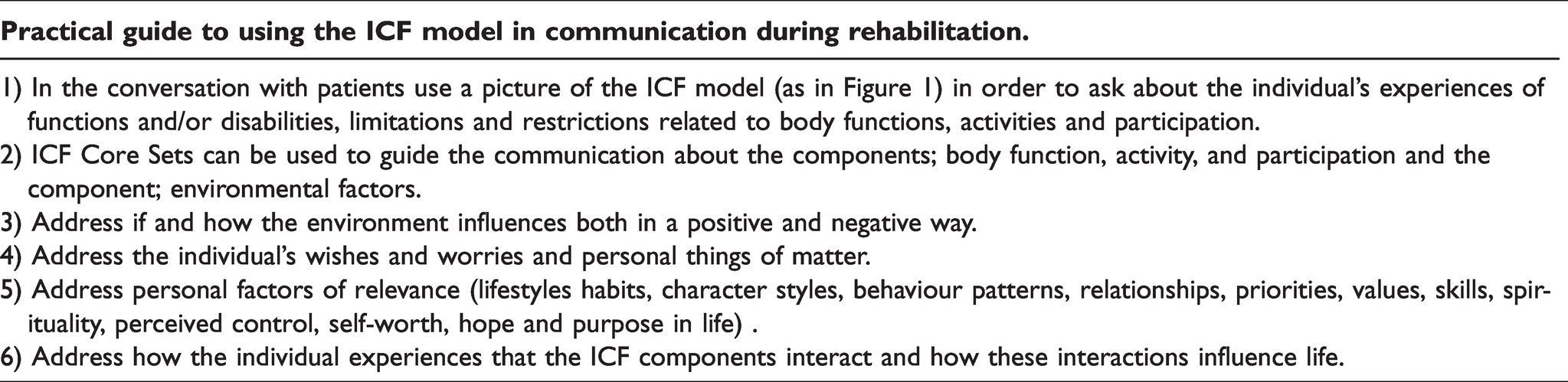
The ICF model is attentive to component interactions, is accepted worldwide and used for several purposes 1 also in relation to spinal cord injury.29,36–39 To capture what matters to individuals with TSCI, the ICF model can guide the communication by addressing each component and specifically approaching the ICF component interactions by means of the arrows in the ICF model. 1 Using the model can facilitate awareness of the ICF component interactions that seem to produce individuals’ complex issues during rehabilitation. We suggest that professionals involved in rehabilitation in practice use the ICF model when communicating about the individuals’ complex issues. When professionals address the individuals’ body functions, activities and participation, as well as their wishes and worries, their complex issues appear in their descriptions of concrete situations, events and dilemmas in daily life. When exploring the environmental factors and personal factors, their influence on body functions, activities, and participation can be revealed (Table 3).
Practical guide.
Limitations and strengths
A limitation is that personal factors are not defined in the ICF model. 1 Therefore, we use the work of Geyh et al. 30 and Post and van Leeuwen, 15 which can be a strength as they detail the descriptions of personal factors. This present study extends the use of the ICF model by specifying ICF component interactions and their influence on individuals’ lives. This may enhance person-centred rehabilitation and increase well-being and empowerment. The ICF model can be used for any health conditions aside from spinal cord injury. 1 We use the ICF Core Sets for individuals with spinal cord injury, which specify the ICF components comprehensively. 29 However, Core Sets are developed in various fields40–42 and can be used to guide practice.
Using the ICF model in communication requires education and training of the professionals in order for them to achieve knowledge about the ICF model and to understand the meaning of ICF component interaction. This can be a limitation of the study.
In our previous study,19–21 the interviews were completed at three time points during the first year post discharge from hospital rehabilitation. During that time, the individuals experienced a development in their life situation. However, this does not impact the ICF model as a tool to capture the complexity of rehabilitation. We focus on the meaning of ICF component interaction, and in that sense the changes over time were not of specific interest. However, we cannot eliminate the possibility that the ICF model can be useful to address changes over time.
Conclusion
The ICF model can capture the individuals’ complex issues. The ICF model could provide a useful tool to facilitate communication; however, only when the focus is on the interactions between the ICF components and thereby the sphere of the real lives of TSCI individuals. This approach can support person-centred rehabilitation. The study is a first step to developing such a tool, and we invite other scholars to contribute to this effort.
Footnotes
Acknowledgements
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.