
Abstract
An increasing number of children attend schools with chronic illnesses/disorders that require managing and comprehensive healthcare from school nurses during the day. Collaboration between school nurses, the school-aged child with attention-deficit hyperactivity disorder (ADHD) or asthma, and their families is needed when coordinating/managing chronic health problems in the school setting. However, involving families in the assessment and care planning processes can be challenging. The aim of this study was to survey the illness beliefs of school nurses and their perceptions of their family nursing practice skills when offering healthcare services to children with ADHD or asthma in schools. A cross-sectional study was used for a sample of 82 school nurses. The manuscript was prepared following STROBE guidelines. Results indicated that the school nurses perceived themselves to be more confident and to have better knowledge and skill in family nursing practice when offering healthcare services to families of children with ADHD in comparison to asthma.
Keywords
Background
School nurses have similar responsibilities throughout the world when providing care to children in schools with chronic illnesses and their family units. School nurses supervise, manage (e.g. medical management), intervene, treat, and coordinate the care of the children when in school; they also work to empower health promotion and decrease risk-taking behaviors.1,2 These nurses also work collaboratively with families, clinicians, and school employees to offer information regarding the health and well-being of the children in their care. 3 About one-fourth of school-aged children have physical or mental chronic illnesses or disorders; 3 many children may have multiple diagnoses.4,5 For the school nurse, this means careful screening and complex care planning, 6 to promote successful and safe caregiving at schools. When engaging families of school-aged children with chronic illnesses in care coordination, therapeutic conversations might be beneficial for the families. In such conversations, it is important for health care professionals to address illness beliefs. Families usually draw on their own strengths to solve problems they encounter. According to Wright and Bell 7 challenging constraining or hindering beliefs and strengthening helpful beliefs is important within therapeutic conversations, since these beliefs have an impact on health. Further, it is vital for healthcare practitioners to be mindful of their beliefs regarding chronic illnesses and to be aware of how their beliefs might influence their therapeutic conversations with families. Nevertheless, little is known about school nurses’ attitudes or beliefs or their perceptions regarding their practice skills with families, especially when offering healthcare services to children with attention-deficit hyperactivity disorder (ADHD) or asthma. This study was undertaken to learn more about these attitudes, beliefs, and perceptions.
Worldwide, the two most common chronic health conditions in school-aged children are ADHD and asthma.8,9 Therefore, a high number of elementary students who are diagnosed with ADHD or asthma need attention and support on a daily basis, from school nurses. Between 5% to 9% of children aged 9 to 17 have difficulty with being able to function in school or in society. 10 The incidence and prevalence of physical chronic illness, such as asthma, has been increasing. 9 The prevalence of children and adolescents with ADHD is 6.4% to 7.2%. 11 Children with serious ADHD symptoms including aggression, emotional deregulation, and learning difficulties may have more problems in school than those without. 12 About 40% to 60% of children with ADHD have been found to have comorbidities such as learning disabilities, anxiety and depression. 13 Asthma impacts quality of life for families.14,15 Consequently, children and adolescents with asthma may require complex daily management of symptoms or exacerbations resulting in emergency hospital visits and admissons. 16 There is a concern that problems regarding psychological health, such as anxiety and depression, are associated with difficult asthma control. 17 The relationship between psychological health, asthma, emotional well-being, and worse asthma outcomes in school children is not well understood. Therefore, school nurses should be the key coordinators and care providers in schools, taking an active role in collaborating with teachers and families of children and adolescents with asthma.3,14
School nurses can enhance their students’ health in their role; 3 with general school personnel, they can have an impact on student well-being. School nurse healthcare services include offering medical and emotional support. The school nurse role in a team of clinicians includes providing healthcare services to children with chronic illnesses in schools and their families, with a specific focus on prevention, early identification, interventions (e.g. therapeutic conversations), and referrals. 6 According to an Icelandic study, nurses in schools are in a good position to offer prevention and health-promoting programs for children. However, lack of time and limited access to specialists in mental healthcare were the main barriers for offering children an appropriate healthcare service when they were seeking assistance. 18
Managing chronic illnesses in schools requires collaboration between the school nurse and the children’s families. Having these individuals work closely together can lead to a better family functioning, improved management of the illness or disorder, and to greater well-being for the school-aged child and their family. However, an understanding of mental disorders and psychiatric education among professionals is often lacking.19,20 Nurses have been found to have more negative attitudes or beliefs towards mental illnesses compared to physicians. 21 School nurses have described little acceptance for children with ADHD and that they have narrow understanding of ADHD and management with stimulants. 22 In a recent study of 97 school nurses in Minnesota, Brown, Looman and Garwick 23 found that school nurses described less assurance and competence in working with families of children with ADHD when measured against families of children with asthma. School nurses need education on ADHD so they can be effective in their assessment and support for children with ADHD. 22 In a study by Poreddi, Thimmaiah and Math, 24 it was suggested that psychiatric education may be effective in changing attitudes of medical students toward people with mental illnesses. Among teachers, their knowledge of ADHD has been found to be very low; 25 some teachers were found to have a low tolerance for children with ADHD. Nurses could play a role in increasing teachers’ knowledge, 26 and thus schools would become an integral part of a process of advancing the healthcare service for children and their families. 10
Illness beliefs have been conceptualized by Wright and Bell 7 as the glasses that we view our world through and that direct our selections in life, our behaviors, and emotional reactions. Further, beliefs are defined by these authors as the values, attitudes, preferences or meanings towards an illness situation. The progress of a chronic illness in a child can result in a difficult emotional reactions within families. Additionally, there are various beliefs held among school-aged children, their families and clinicians about the prognosis or the etiology of an illness that can impact the school nurse. Through therapeutic conversations, the nurse can generate an environment for soothing, by looking at illness beliefs, facing hindering beliefs and by reinforcing helpful beliefs.7,27–29 Therefore, the greatest challenge for school nurses, other healthcare providers, and teachers, may be to recognize and to challenge their own beliefs, to see if they are useful or not, regarding the caregiving of the child or adolescent.
Nurses’ beliefs and attitudes towards an illness have also been found to correspond to their family nursing practice.8,28,30,31 To encourage a more active role in school nurses’ care coordination, when offering healthcare services to children with asthma and their families, it is important to know their attitudes and beliefs and their awareness of their practice skills with families. By offering therapeutic conversations to families dealing with different health conditions in school settings, school nurses can invite the families to reflect on their illness experiences and on their illness beliefs, to facilitate a new view and understanding of themselves; to identify their strengths and resources to handle the illness or to apply new methods to cope with the illness situation.
The Calgary Family models (CFAM/CFIM) 28 and the Illness Beliefs Model 7 were the conceptual frameworks for this research. In these clinical models, school nurses’ views regarding including family members in their care at schools are perceived to be impacted by their beliefs regarding illness, healthcare professionals and families. These clinical models can guide nurses when they are assessing, interacting, and intervening with families of children with health problems. According to Wright and Bell, 7 how children in elementary school and their family members experience an illness is more dependent on their beliefs than on the diagnosis. Beliefs of school nurses can have an impact on their decisions in offering treatment and on how they interact with family members of children diagnosed with chronic disorders or illnesses.
Research questions
Based on the literature review and on the CFAM/CFIM 28 and the Illness Beliefs Model 7 we asked to following research questions: (a) What are the differences in illness beliefs amongst school nurses caring for children with ADHD and asthma? (b) What are the differences in nursing family practice skills amongst school nurses caring for children with ADHD and asthma? (c) What predicts family nursing practice skills, among school nurses caring for children with ADHD and asthma?
Methods
Procedure and participants
Potential participants needed to be school nurses working with elementary school-aged children in a school setting in either the rural or the urban area in Iceland. A Community Health Care nurse with an MSc degree, who was responsible for organizing the data collection, introduced the study to all school nurses in Iceland (N = 130). After the school nurses had signed the consent form, they received, via email, a separate electronic code which they could use to enter the research electronic data capture (REDCap) study. There were 106 (81.5%) participants who were enrolled in the study and accessed the REDCap electronic survey. 32 Out of those, there were 82 nurses who completed the questionnaires (76.4%). The data were collected in September–December 2015. The manuscript was prepared following STROBE guidelines. 33
Data collection
Background information included participant age, education, practice location, employment status, type of schools, number of children with asthma and ADHD cared for and frequency of contacts with children with asthma and ADHD (see Table 1).
Background information of the school nurses (N = 82).
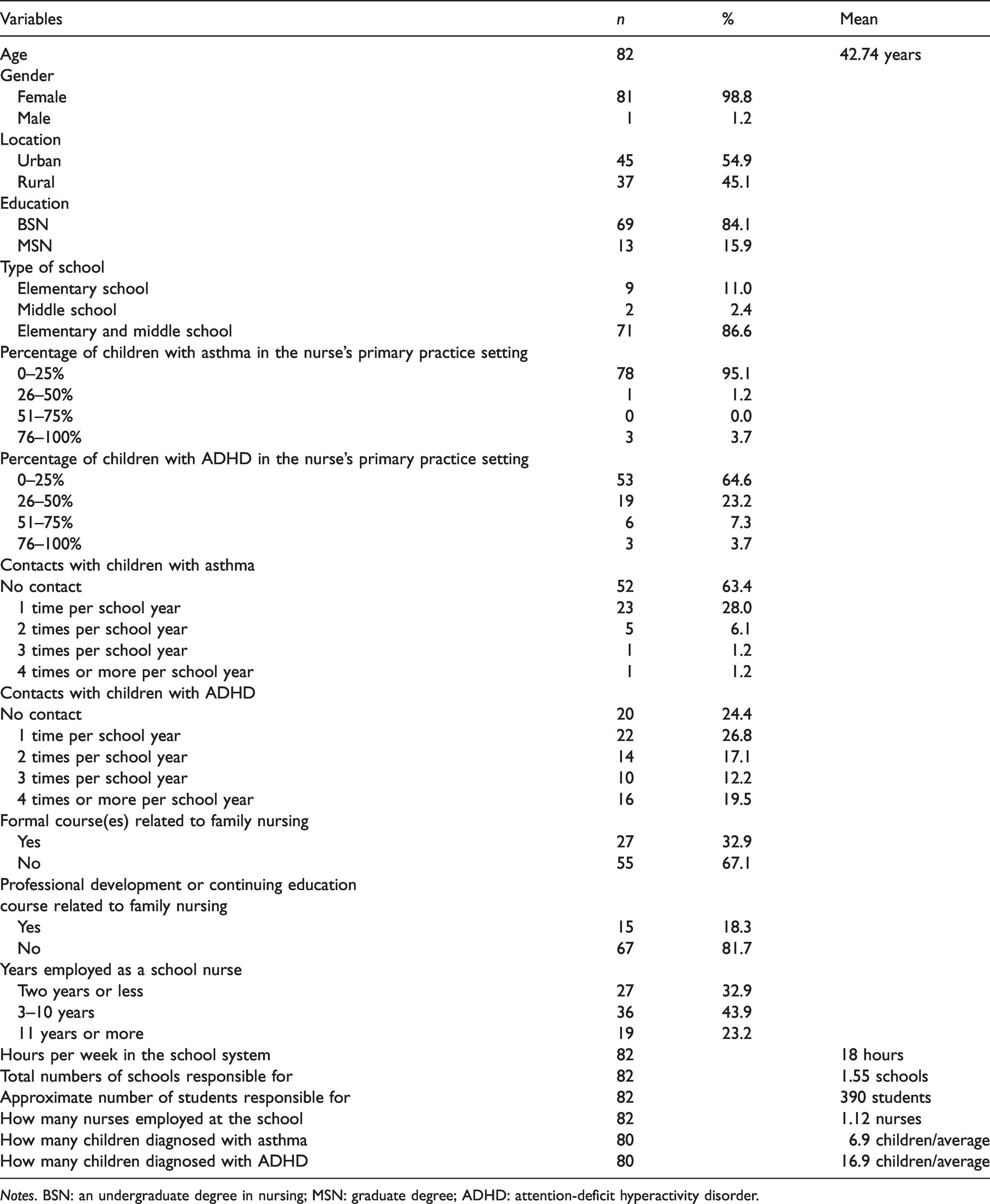
Notes. BSN: an undergraduate degree in nursing; MSN: graduate degree; ADHD: attention-deficit hyperactivity disorder.
Paired t-tests of school nurses’ perceptions regarding their illness beliefs and their practice skills in family nursing for families of children with asthma and for families of children with ADHD (N = 82).
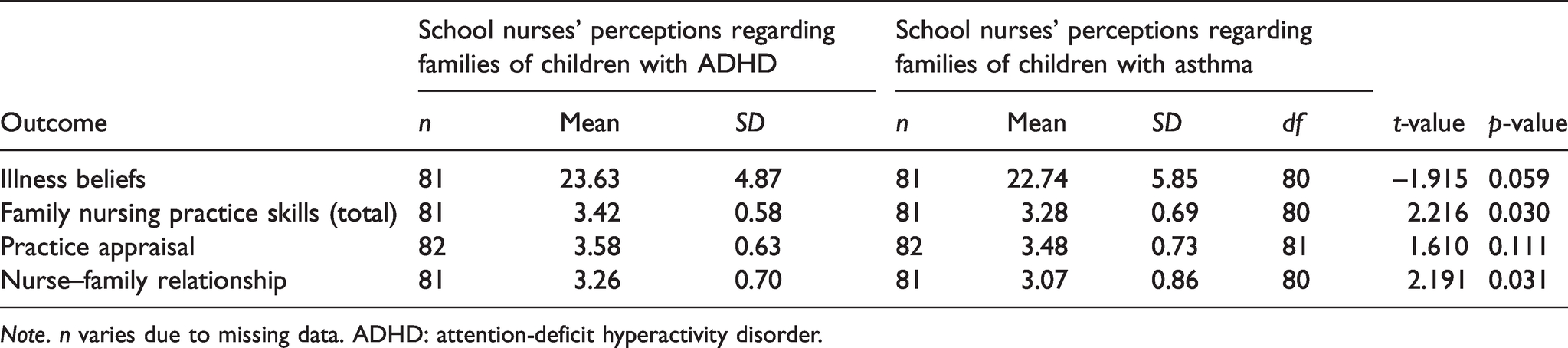
Note. n varies due to missing data. ADHD: attention-deficit hyperactivity disorder.
Yates Chi-square tests based on level of education (BSN vs. MSN) of school nurses’ perceptions regarding their practice skills in family nursing for families of children with ADHD and for families of children with asthma (N = 82).
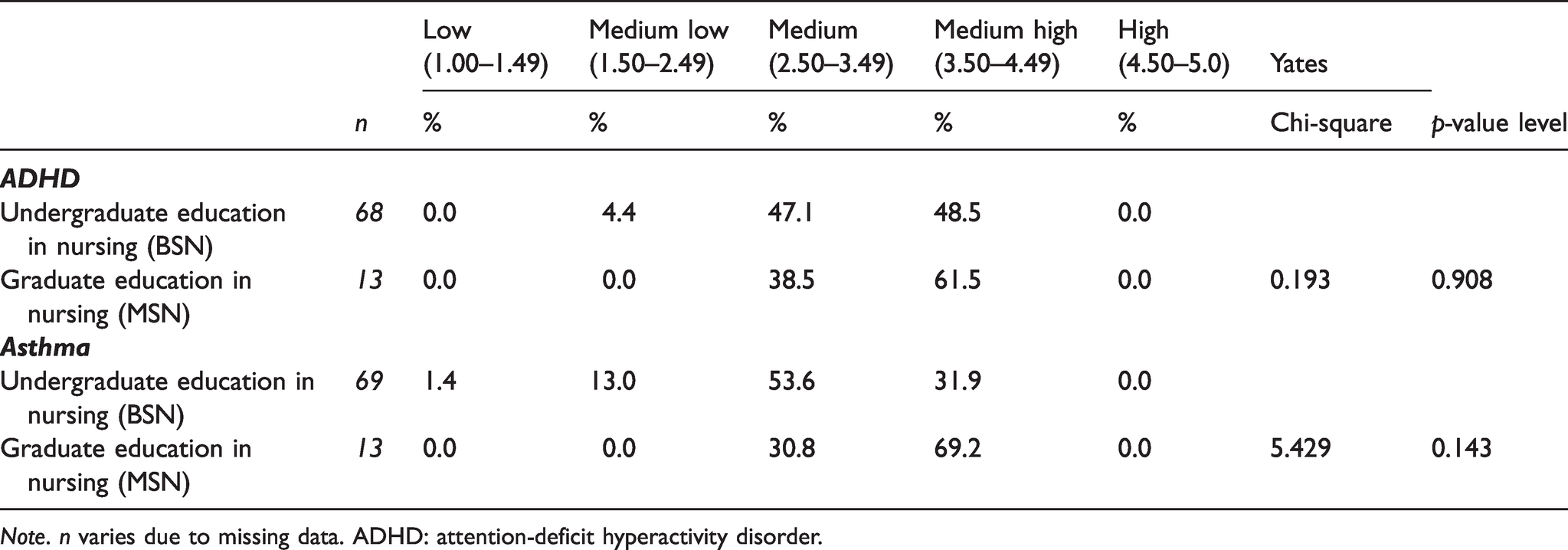
Note. n varies due to missing data. ADHD: attention-deficit hyperactivity disorder.
Linear regression analysis among school nurses for predicting family nursing practice skills for families of school children with ADHD (n = 81).
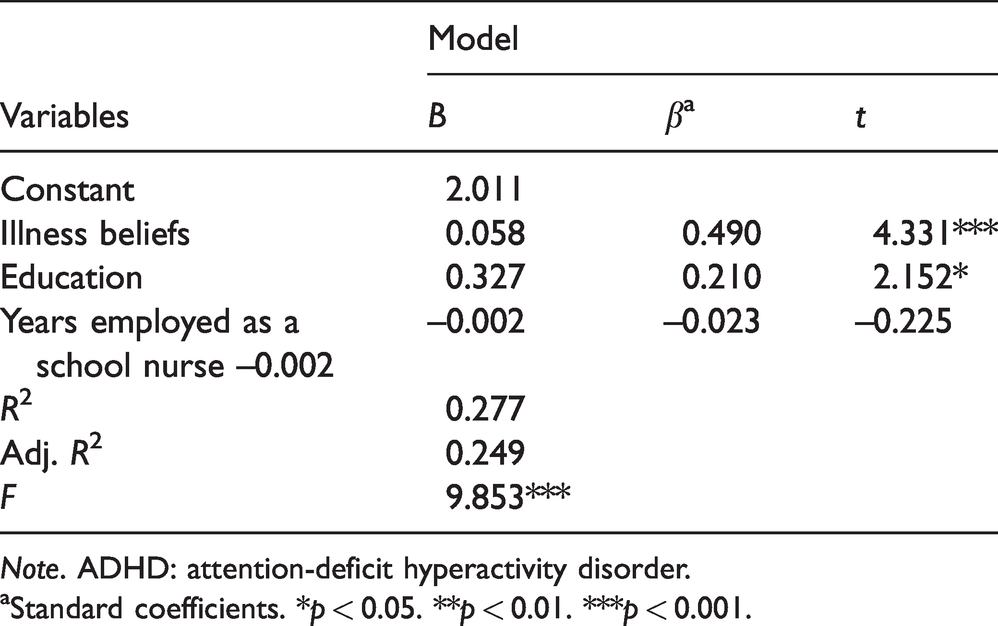
Note. ADHD: attention-deficit hyperactivity disorder.
aStandard coefficients. *p < 0.05. **p < 0.01. ***p < 0.001.
Linear regression analysis among school nurses for predicting family nursing practice skills for families of school children with asthma (n = 81).
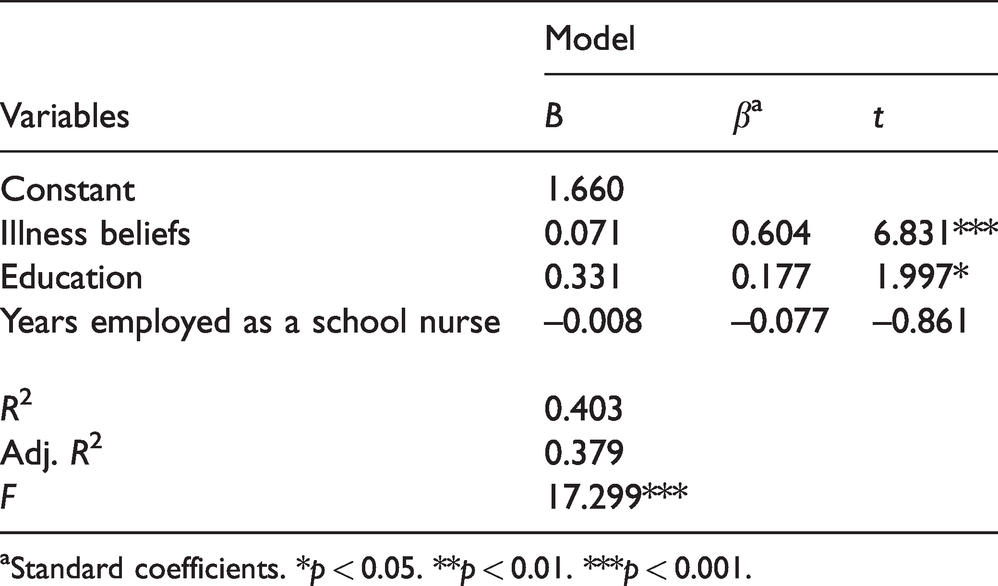
aStandard coefficients. *p < 0.05. **p < 0.01. ***p < 0.001.
The Iceland Health Care Practitioner Illness Beliefs Questionnaire 8 has seven items and an additional four open-ended questions. It is designed for healthcare practitioners who are caring for children in schools with asthma and ADHD. Statements about the healthcare practitioners’ beliefs are ranked never (1), rarely (2), sometimes (3), usually (4), and always (5). Scores are summed; higher scores indicate more self-confidence in illness beliefs about asthma and ADHD. Open-ended responses were not used in the analyzes in this study. The questionnaire is both reliable and valid and has been psychometrically tested. Cronbach’s alpha is reported to be 0.83–0.92. In this study, Cronbach’s alpha = 0.92 for ADHD and = 0.91 for asthma. Only the Likert-type responses are analyzed and reported on in this study.
The Family Nursing Practice Scale 34 is a 10-item Likert-type measure with open-ended responses, that evaluates perception of practicing with families. The instrument has two subscales (a) critical appraisal of the nurse’s family practice (Practice Appraisal-PA) and the nurse’s assessment of their Nurse Family Relations (NFR). The scale ranges from 1 to 5; higher scores indicated better outcomes. According to the literature, scores within two units of the maximum are considered to be high and scores within two units of the minimum are considered to be low.21,28,29 This measure is valid and reliable and has been psychometrically tested. Cronbach’s alpha reliability coefficients have been reported to be 0.86 for the total scale and 0.88 and 0.73 for the two subscales. 34 Cronbach’s alpha in this Icelandic study was = .89 for ADHD and =.84 for asthma. Only the quantitative items are used in this analysis.
Data analysis
Data were analyzed to answer the research questions through descriptive statistics, paired t-tests, Chi-square statistics, Pearson’s correlations between main study variables, and linear regression.35,36 The linear regression analysis was conducted by entering the illness beliefs variable, the family nursing practice scale variable and the numbers of years practicing as a school nurse into the regression model. These variables were chosen based on the models that guided the research and theoretical constructs about illness beliefs. Further, both the outcome variable (the family nursing practice skills) and the independent variable (illness beliefs) that were entered into the regression analyzes were continues variables. The categorical variable that was entered into the equation was the level of education (BSc vs. MSc). IBM SPSS Statistics was used for analysis of the data.
Ethical considerations
This study is a part of the International School Nurse Asthma and ADHD research Project (I-SNAAP). The study was conducted simultaneously in Iceland and Minnesota, USA. The study was approved as being of minimal risk by the Institutional Review Boards in each country. Results from the Minnesota study have been previously published.23
Results
The majority of participants were female (99%), with a mean age of 43 years, were registered nurses (RNs) and had bachelor’s degrees in nursing (84%). Only 16% of the school nurses had MScs in nursing. Over half were working in an urban school setting (55%) and most were working concurrently at the elementary and middle-school level (87%). Each nurse was most often responsible for 1–2 schools and worked a mean of 18 hours per week in the school system. Participants were responsible for about 390 students on average; they had contact 1–2 times over the school year with each child with asthma (n = 287, 34%), and contact 1–4 times/year with each child with ADHD (n = 62, 76%). They identified that 1.9% on average (n = 6.9), of children in their schools had asthma and 5.1% on average (n = 16.9), of children in their schools had ADHD. The majority of participants had not taken a continuing education course related to family nursing (82%) or formal course(s) related to family nursing (67%) (See Table 1).
There were no significant differences on the Illness Beliefs subscale between families of children with ADHD or asthma. That is, the school nurses perceived that they knew the cause of both ADHD and asthma, that they knew how to control both ADHD and asthma, and that they knew the effect, who was suffering the most and what was most and least helpful to cope with ADHD and asthma (t = –1.015, p = 0.059) (See Table 2). However, a significant difference was found on perception regarding practice skills for families of children with asthma versus ADHD (MADHD = 3.42, Masthma = 3.28, t = 2.216, p = 0.030) (See Table 2). Thus, participants perceived themselves to be more confident with better knowledge and skills for children and families with ADHD when compared to families of children with asthma. Similarly, they perceived that they had better nurse–family relationships with families of children with ADHD compared to families of children with asthma (MADHD = 3.26, Masthma = 3.07, t = 2.191, p = 0.031) (See Table 2). There was no significant difference on the subscale of Practice Appraisal between their perspective when offering healthcare services to children with ADHD and their families, compared to asthma (t = 1.610, p = 0.111) (See Table 2).
Participants with an undergraduate degree in nursing (BSN) perceived their family nursing practice skills to range from low to medium-high. However, participants with a graduate degree (MSN) reported their family nursing practice skills to range from medium to medium-high. This difference between the level of education of the nurses was, however, not statistically significant (See Table 3).
Results from the linear regression analyses indicated participants’ perceptions of illness beliefs towards ADHD and their level of education explained 25% of the variance in the outcome of their perception regarding their family nursing practice skills (adjusted R2 = 0.249, p < 0.001) (See Table 4). Similarly, perceptions of their illness beliefs towards asthma and level of education explained 38% of the variance in the outcome of their perception regarding their family nursing practice skills (adjusted R2 = 0.379, p < 0.001) (See Table 5). School nurses’ illness beliefs when offering healthcare services to children with asthma and ADHD and their families, and their level of education (MSN vs. BSN) predicted between 25% to 38% of the variance in their perceptions regarding their nursing practice skills with families.
Discussion
The main finding suggests that the school nurses’ perceptions regarding their confidence, competence, knowledge, and skill in family nursing practice, when caring for children in schools with ADHD was perceived to be significantly higher when compared to children with asthma. Further, their perceptions towards the nurse–family relationship when the focus was on planning interventions were also significantly higher when caring for children with ADHD in comparison to asthma. To our best knowledge, this result is new and has not been reported before in the literature and therefore adds to it. One explanation could be that these Icelandic school nurses had, as indicated in the study, more frequent contact over the school year with children with ADHD in comparison to children with asthma. Another explanation might be that the nurses had been working in the school system for a fairly long time: 3 to 11 or more years. Thus they might be more experienced in caring for children with ADHD as they had more frequent contact. In the Icelandic school system, children with ADHD have special accommodations, for example, a quiet room for test-taking; as a result, the school nurses might been more aware of children with ADHD as compared to asthma. It is worth noting that most participants had not taken a formal course or continuing education course in family nursing. The school nurse role is to be supportive to students and their families with chronic health conditions in order to enhance their learning. Family nursing practice in schools might be enhanced by offering school nurses a formal course with an emphasis on therapeutic conversations for these children and their families.
It is notable that the participants perceived their illness beliefs regarding ADHD and asthma to be more similar rather than different. The participants were confident in their perceptions regarding the causes of ADHD and asthma, symptom management, effect of the health conditions on families, and on receiving support from healthcare providers. Understanding the participants’ illness beliefs is important, because nurses’ beliefs and attitudes have been found to correspond to their utilization of system knowledge and skillfulness in clinical practice.7,28,31
Even though the participants perceived themselves to have more family nursing knowledge and skill and to be more confident in caring for school-aged children with ADHD than with asthma, the mean score on the family nursing practice skill scale ranged from low to high. However, in contrast to the findings from this Icelandic study, Brown, Looman, and Garwick, 23 found school nurses in Minnesota to report significantly higher item means on three practice appraisals for asthma compared to ADHD. In other words, the school nurses in Minnesota reported less self-confidence and skills, caring for family members of children with ADHD when compared to asthma. One explanation for this contradiction could be that the Icelandic nurses reported more than twice as many children with ADHD in the school setting compared to those with asthma. On the other hand, the school nurses in Minnesota reported more students in their schools with asthma than ADHD.
Interestingly, for both ADHD and asthma, participants’ illness beliefs and their level of education (MSN vs. BSN) predicted their family nursing practice skills. This finding is important as, even though the majority of the participants had a BSN, those with an MSN contributed to the explanation of the variance in their nursing practice skills with families. This finding regarding the level of education is consistent with findings from Brown and colleagues 23 who found that school nurses with a graduate school education described better skills working with families. Similarly, Svavarsdottir and colleagues 37 reported that nurses with a master’s education who took a continuing education family nursing course scored significantly higher on the family nursing practice questionnaire, when compared to BSc-prepared nurses. Graduate school education can increase skills in working with families of children with chronic disorders; this might increase a nurse’s confidence and knowledge and in turn contribute to the nurse–family relationship. School nurses need to expand their family nursing knowledge where the attention is on the child and the family unit, but not just on the health condition. Through evidence-based family nursing practice, school nurses can learn how the family has an impact on the child, how members of the family help, sustain, or expand the child’s health, and grasp more entirely the child’s perspective regarding their health and life.
Methodological considerations
The cross-sectional research design in the study is a limitation within itself since the design only presents a snapshot of reality but the study was conducted about five years ago. However, we believe that the content is very much relevant and up to date, especially since beliefs and perceptions on family nursing practice skills take time to change, which can be achieved if needed through education. The sample is, however, well representative of the population, but the population of school nurses in Iceland was 130 nurses at the time of the study. The instruments used are both reliable and valid and the community healthcare nurse who collected the data had an MSc in nursing and had been trained in the data collection procedure. Because a high percentage of the population of school nurses participated, the findings from this sample can be generalized to the population. One limitation, however, to keep in mind is that the school nurses’ illness beliefs might not predict their actual behavior with families. Further, self-report was used in the research, but future studies may consider an experimental research design (testing the impact of a family nursing education on nursing practice) or other methods such as interviews or observations.
Conclusion
Evidence-based practice is now considered to be the standard goal in healthcare. Therefore, school nurses need to be aware of how to utilize research evidence regarding family-centered care in their clinical practice, when caring for children with ADHD and asthma. Therapeutic conversations have benefitted families of children with chronic disorders and illnesses. Therefore, to enhance family nursing practice in schools, school nurses might consider taking formal courses in family nursing or pursue graduate education so they will be able to offer therapeutic conversation with family members of children with chronic health conditions.
There is a call from institutions to offer family-centered care because of increased data on the benefits of involving family members in the healthcare services. In this study, school nurses perceived themselves to be confident and to have better knowledge and skills when offering healthcare services to families of children with asthma compared to children with ADHD. This underlines the need for further family nursing education among school nurses. Additionally, their beliefs and having an MSc education explained over 25% of the variability in their perceptions of their family nursing practice skills, which highlights the importance of graduate school education among school nurses.
Supplemental Material
sj-pdf-1-njn-10.1177_20571585211009690 - Supplemental material for Enhancing family nursing practice in schools: School nurses’ perspectives on illness beliefs and family nursing practice skills when caring for children with attention-deficit hyperactivity disorder or asthma – A cross-sectional study
Supplemental material, sj-pdf-1-njn-10.1177_20571585211009690 for Enhancing family nursing practice in schools: School nurses’ perspectives on illness beliefs and family nursing practice skills when caring for children with attention-deficit hyperactivity disorder or asthma – A cross-sectional study by Erla Kolbrun Svavarsdottir, Gudny Bergthora Tryggvadottir, Margret Gisladottir and Ragnheidur Osk Erlendsdottir in Nordic Journal of Nursing Research
Footnotes
Human subjects approval statement
This study is a part of the International School Nurse Asthma and ADHD research Project that was conducted simultaneously in Iceland and Minnesota, USA. The study was approved as being of minimal risk by the Institutional Review Boards both in Iceland and in Minnesota. Participants provided informed consent at the beginning of the online survey.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author contribution
The study was designed by EKS. ROE worked on the data collection in collaboration with EKS. GBT in collaboration with EKS analyzed the data. EKS wrote the manuscript with critical input from MG. The manuscript was prepared following STROBE guidelines.
Acknowledgments
The authors would like to thank all the school nurses who participated in the study for their participation..
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by a grant from the Icelandic Nurse Association in Reykjavik, Iceland.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.