
Abstract
Emergency care nurses (ECNs) face several challenges when they assess patients with different symptoms, signs, and conditions to determine patients’ care needs. Patients’ care needs do not always originate from physical or biomedical dysfunctions. To provide effective patient-centred care, ECNs must be sensitive to patients’ unique medical, physical, psychological, social, and existential needs. Clinical practice guidelines (CPGs) provide guidance for ECNs in such assessments. The aim of this study was to evaluate the quality of CPGs for comprehensive patient assessments in emergency care. A quality evaluation study was conducted in Sweden in 2017. Managers from 97 organizations (25 emergency medical services and 72 emergency departments) were contacted, covering all 20 Swedish county councils. Fifteen guidelines were appraised using the validated Appraisal of Guidelines for Research & Evaluation II (AGREE II) tool. The results revealed that various CPGs are used in emergency care, but none of the CPGs support ECNs in performing a comprehensive patient assessment; rather, the CPGs address parts of the assessment primarily related to biomedical needs. The results also demonstrate that the foundation for evidence-based CPGs is weak and cannot confirm that an ECN has the prerequisites to assess patients and refer them to treatment, such as home-based self-care. This may indicate that Swedish emergency care services utilize non-evidence-based guidelines. This implies that ECN managers and educators should actively seek more effective ways of highlighting and safeguarding patients’ various care needs using more comprehensive guidelines.
Introduction
The professional foundation of nursing care values and responsibilities includes the registered nurse’s (RN) stance, approach, and actions. Based on a humanistic and caring perspective in which the human being is viewed as an entity consisting of body, soul, and spirit with varying nursing needs, the RN’s task is to alleviate patients’ suffering and promote well-being. 1 In emergency medical services (EMS) and emergency departments (ED) (henceforth ‘emergency care’), which involve life-threatening, urgent, and non-urgent care situations, patients are more exposed, dependent, and vulnerable than in other care situations.2–6 This constitutes a challenge for RNs to address issues related to patient assessment, participation, and influence over care.7–9 In emergency care, RNs and specialist nurses (henceforth ‘emergency care nurses’, ECNs) face challenges when they assess patients with different symptoms, signs, and conditions to determine patients’ care needs.10–12
Assessing patients, determining whether their conditions are stable or unstable, and defining care needs are important tasks for ECNs. 10 Failure to assess patients according to their individual care needs may lead to undesired consequences, such as incomplete nursing care and adverse health events. 13 In Sweden, patient assessment generally focuses on patients’ physical and biomedical status by using the A-E principle (airway, breathing, circulation, disability, and exposure), observing vital signs, and listening to the patient’s perceived symptoms of illness or injury. 14 Most ECNs use the Rapid Emergency Triage and Treatment System (RETTS) to assess the patient’s medical care needs. 15 In addition to conducting a structured and often time-constrained medical assessment, ECNs must develop an understanding of each patient’s care needs and complex health conditions.16–18 In a comprehensive assessment, patients’ urgent care needs may prove to be based on non-medical or non-physical problems. In addition, a significant number of patients in emergency care are older persons with increased care needs. 19
To provide effective patient-centred care, ECNs must be sensitive to patients’ unique psychological, social, and existential care needs. 14 This promotes a comprehensive patient assessment defined as a five-dimensional evaluation of medical, physical, psychological, social, and existential needs. 20 Physical examinations involve determining patients’ abilities, the degree of physical activity in their daily lives, their balance, and their risks of falling.14,21 Patients’ psychological needs are assessed in terms of sleeping problems, depression, stress, melancholy, and risk of suicide. Finally, patients’ social and existential needs are assessed in terms of their autonomy and ability to make decisions and experience meaning in their lives. 22
In this article, a comprehensive patient assessment is viewed as an ongoing process that begins when a patient is first encountered by an ECN and ends when the patient is discharged from the ED, gets referred to a more suitable level of care, or is left at home or on site with self-care advice. This means that comprehensive patient assessments are not a one-time occurrence. Research indicates that comprehensive assessment of patients has a positive impact, leading to increased patient satisfaction and fewer patients leaving the ED without being assessed. 23 However, the environment in which ECNs carry out their assessments is frequently chaotic, unpredictable, and stressful.3,8,17,24 One way to promote the initiation of a comprehensive patient assessment in acute or urgent situations is to offer nurses support and standards in terms of clinical practice guidelines (CPGs).
Clinical practice guidelines are tools that support the use of the best available evidence.25,26 They are recommendations aimed at promoting quality healthcare, reducing practice variability, and helping ECNs make decisions about patient care. 25 However, CPGs are not always available or used as intended. Research has indicated that CPGs focus on patients with acute medical needs, and there is a lack of CPGs for non-urgent patients and acute abdominal conditions.27,28 Adherence to and trust in CPGs might also be lacking. A study of RETTS revealed that a correctly documented level of urgency varied from 43% in EMS to 64% in EDs, which indicated poor adherence to CPGs for medical assessment. 29 Another RETTS study indicated that only 15% of medical assessment scenarios were conducted in concordance with the CPGs. 15
Transferring guidelines into clinical practice might also be problematic. Previous research has found that inadequate administrative and organizational support made it difficult to use the guidelines in practice, 30 resulting in time-consuming screening, flow stops, and insufficient time to implement the CPGs. 31 Although CPGs were available, their implementation and dissemination also depended on their quality. 32 Low methodological precision and non-specific recommendations can influence CPG quality. 33 Various CPGs are used in Swedish emergency care. However, it is unclear whether these constitute support for ECNs when performing a comprehensive patient assessment.
In summary, in keeping with ECNs’ professional foundation of ethical core values and responsibilities, comprehensive patient assessments should be initiated as soon as possible to meet patients’ varying nursing needs. Given the difficult context in which ECNs operate, it is reasonable for them to be given optimal guideline support in their assessments. Therefore, the aim of this study was to evaluate the quality of CPGs for comprehensive patient assessments in emergency care.
Method
To increase our knowledge and develop a better understanding of ECNs’ assessment of patient care needs, a study was conducted to explore the quality of CPGs for comprehensive patient assessment. 34
Sample and setting
A quality evaluation study was conducted between January and June 2017. A total of 97 emergency care organizations (25 EMS and 72 EDs), covering all 20 Swedish county councils, were invited to participate.
Data collection
A request to provide CPGs for comprehensive patient assessments was sent by email to EMS managers and by letter to ED managers. An informational letter was sent alongside this request. The letter clarified the definition of a comprehensive patient assessment as including medical, physical, psychological, social, and existential needs. Some managers replied by asking for more specific information about which CPGs to provide. They were informed that all CPGs used for comprehensive patient assessment within their organization were eligible.
After two reminders, 103 CPGs (EMS, n = 59; ED, n = 44) were received, representing a large geographical spread across Sweden. Several CPGs were submitted by each organization (ED, range = 1–20, mean = 5, median =4.5; EMS range = 1–37, mean = 6.7, median = 3). During the screening of the CPGs (see Figure 1), 24 duplicates were identified. The duplicates included different versions of RETTS journals, which targeted different patient groups, such as children, adults, and trauma patients. Furthermore, 51 management documents describing ECN assignments, transportation between hospital departments and care facilities, and 13 care programmes (EMS, n = 10; ED, n = 3) were excluded. After screening, a total of 15 CPGs were retained for further analysis.
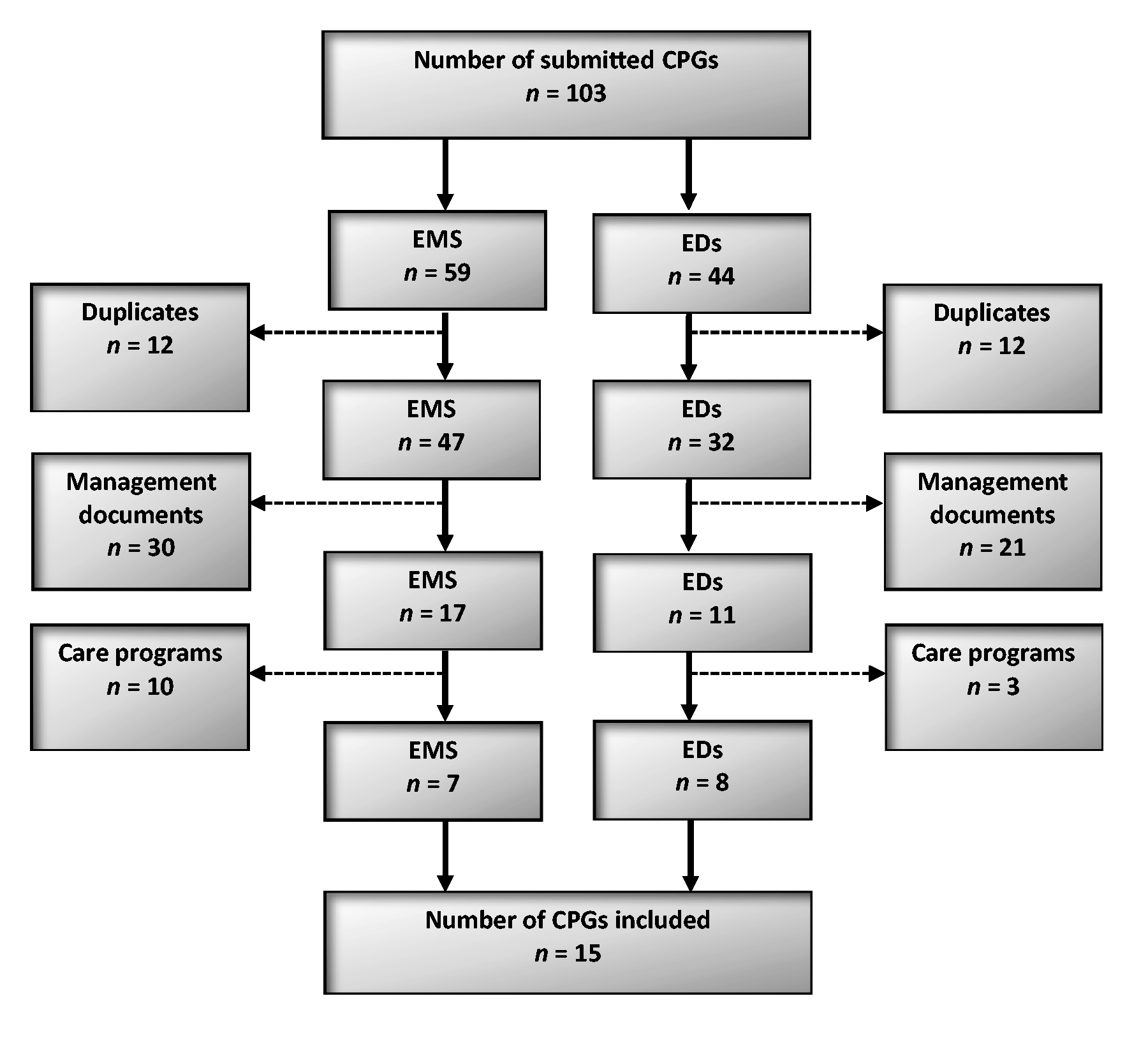
Flow chart of the inclusion process of clinical practice guidelines (CPGs) from emergency medical services (EMS) and emergency departments (EDs).
Quality appraisal of the guidelines (analysis)
The first and second authors conducted a quality appraisal of the CPGs using the Appraisal of Guidelines for Research and Evaluation (AGREE II) instrument. 34 AGREE II is an instrument that evaluates CPGs according to six domains: 1) scope and purpose, 2) stakeholder involvement, 3) rigour of development, 4) clarity of presentation, 5) applicability, and 6) editorial independence. 29 Each domain was rated for how well the CPG fulfilled the domain-specific items using a seven-point scale from 1 (strongly disagree) to 7 (strongly agree). The individual items for each domain are presented in the instructions manual for the AGREE II instrument. 34
A quality score was calculated for each domain. No CPGs were excluded due to low scores. Quality appraisal was initially a combined effort involving the first three CPGs to gain a sense of coherence in the appraisal process. The remaining 12 CPGs were divided between the two authors and appraised separately. After the review and scoring were completed, the results were discussed between the authors, and any doubts that had arisen during the appraisal process were resolved. Possible doubts included whether a CPG fell within the scope of the study (n = 1) or uncertainties regarding the scoring of a specific item during the appraisal of a CPG (n = 3). The data were analysed using descriptive statistics, such as range and median values.
Ethical considerations
This research was regulated by Swedish law, 35 which meant that no ethical approval from the Regional Ethics Review Board was needed and consequently this was not applied for. However, the study was conducted in line with the Declaration of Helsinki, 33 and the participants received written information about the study’s aim and procedures in advance. Informed consent was considered fulfilled when the participants responded to the participation request and submitted their CPGs. Special emphasis was placed on treating all replies confidentially to protect the identities of the emergency care organizations.
Results
Fifteen (N = 15) CPGs were included for evaluation: seven from EMS and eight from EDs. The results show that no CPG outlined a comprehensive patient assessment covering all five activity areas of interest. For further information, see Table 1.
Distribution of clinical practice guidelines (CPGs) and their coverage/inclusion of the five-dimensional areas of patient needs.
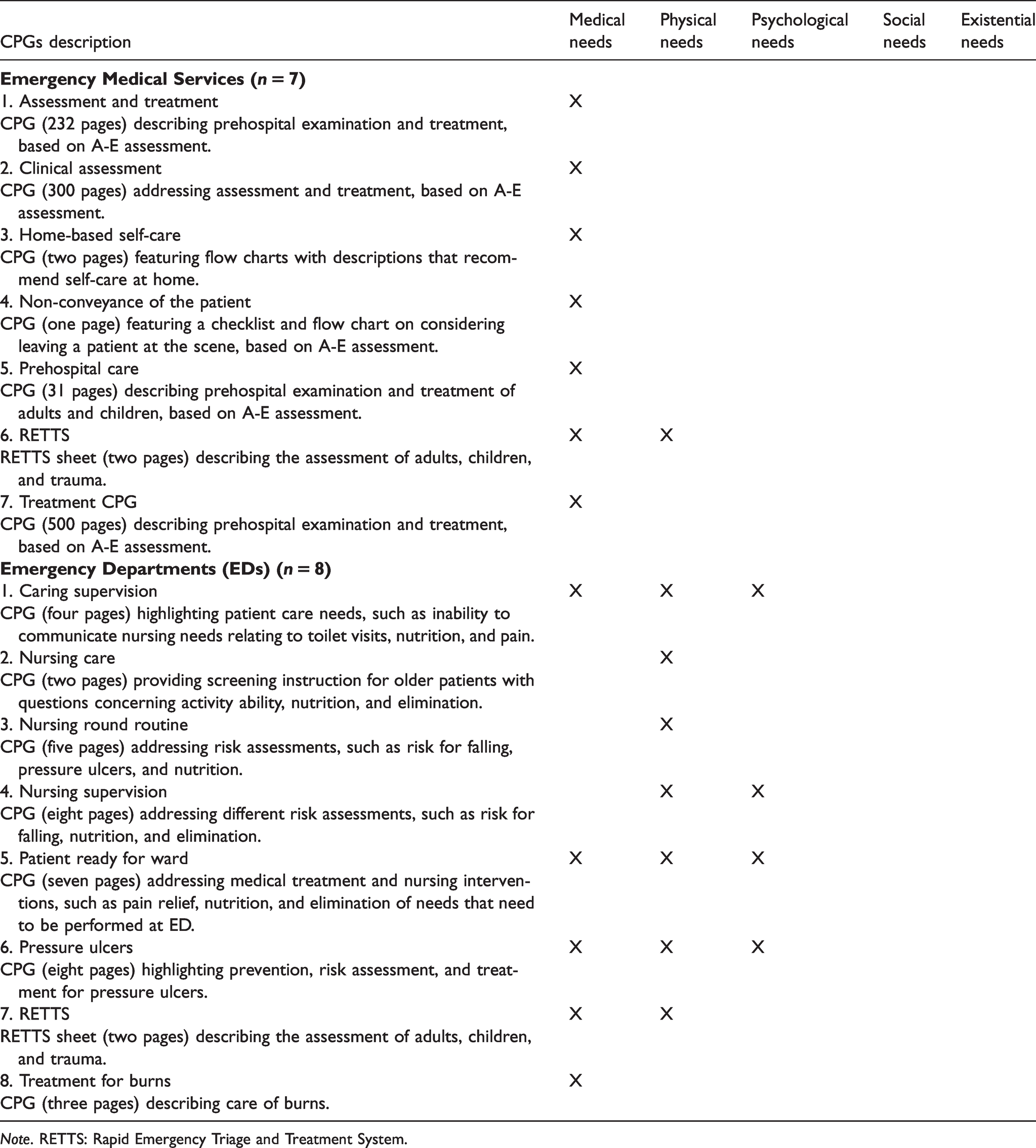
Note. RETTS: Rapid Emergency Triage and Treatment System.
There were no clear connections to scientific evidence in any of the guidelines. Five CPGs (two from EMS and three from EDs) had a reference list, and one ED CPG contained comments from patients obtained through interviews. The main characteristic of the CPGs was their focus on the medical assessment of patients with life-threatening conditions, mostly based on initial assessment and the A-E principle.
Emergency medical services
The EMS CPGs (n = 7) stated that the guidelines were based on decision support systems for patient assessment. Five of the EMS CPGs referred to the RETTS guidelines. One EMS CPG stated that it was the only CPG used to assess patient care needs. Six of the EMS CPGs were comprehensive and covered the entire care process, including assessment, treatment, monitoring, and handover. These differed from other CPGs in that they had a table of contents. The various section headings were written in bold, and two CPGs had colour-coded content sections, which further facilitated section navigation in addition to page reference. This provided a higher score in domain 4 (clarity of presentation) of the AGREE II appraisal.
Emergency departments
Of the eight ED CPGs included, one was the RETTS guidelines. Seven ED CPGs referred to preventing and treating pressure ulcers, treating burns, and accommodating nursing and patient supervision in the ED. All the EDs used the RETTS as a basis for patient assessment.
Quality appraisal of the guidelines
The AGREE II analysis revealed significant variation in the quality of CPGs. The EMS CPGs were all comprehensive and homogeneous. The ED CPGs were less extensive, but all had a homogeneous structure with bolded headlines and bulleted lists. Only one ED CPG referenced the material used to develop it, including references to databases, keywords, and the date of the literature search. Five CPGs (two from EMS and three from EDs) presented reference lists. However, no descriptions of the criteria drawn from these references were provided; it was unclear how the references were related to the CPG content. See Table 2 for more information.
AGREE II domains and clinical practice guidelines (CPGs) (N = 15) quality scores from emergency medical services (EMS) and emergency departments (EDs).
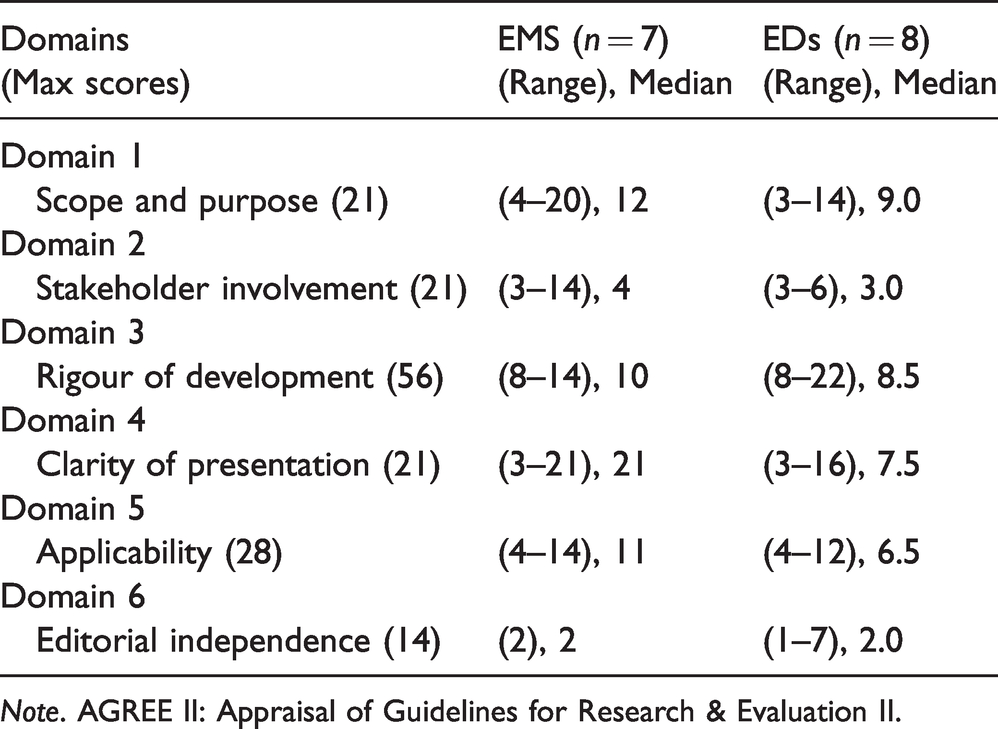
Note. AGREE II: Appraisal of Guidelines for Research & Evaluation II.
Domain 1: Scope and purpose
This domain concerned the overall aims of the CPGs, their specific health questions, and their target populations. Three CPGs (two from EMS and one from an ED) indicated the target group for the guidelines, using expressions like ‘healthcare staff’, ‘ambulance staff’, and ‘nurses and assistant nurses’. Five CPGs (three from EMS and two from EDs) received the highest scores because they clearly stated which staff categories or patient groups they were intended for. This information was presented in boldfaced font, bulleted lists, tables, and using colour markings.
Domain 2: Stakeholder involvement
The second domain focused on the extent to which the CPGs were developed by appropriate stakeholders and represented the views of their intended users. In two CPGs (one from EMS and one from an ED), the names and professional statuses of those involved in CPG development were presented. In 14 CPGs (seven from EMS and seven from EDs), the specific names of the persons who created or were responsible for the content were presented. One ED CPG presented the roles of persons involved in the development process: four senior executives, seven management physicians, and one specialist nurse. One ED CPG presented comments obtained from patients through interviews.
Domain 3: Rigour of development
The third domain concerned the process used to gather and synthesize the evidence for the CPG, the methods of formulating the recommendations, and the procedures for updating the CPG. One ED CPG presented the evidence upon which it was based, described how that evidence was collected, and listed the criteria used to develop the CPG. It also described its strengths, weaknesses, and health benefits. Five CPGs (two from EMS and three from EDs) included reference lists. The remaining 10 CPGs did not have reference lists. One ED CPG only presented how its evidence had been selected. One ED CPG was subjected to an external review process carried out by physicians, nurses, senior executives, and healthcare developers from other departments in the same hospital. One ED CPG described how its processes would be updated.
Domain 4: Clarity of presentation
The fourth domain involved the language, structure, and format of the CPG. In 12 CPGs (seven from EMS and five from EDs), the recommendations were clearly written. The EMS CPGs were similar in structure; that is, they all used bold headings and categorized phenomena alphabetically. The assessment process steps were easy to identify because they were presented in bulleted lists and followed the A-E principle.
In six ED CPGs, there were larger bodies of text in which the main recommendation was missing or unclear. This ambiguity arose from the recommendation being inserted into larger bodies of text instead of being placed under a heading as an independent subsection. Two ED CPGs presented brief and clear descriptions for each item in the patient assessment, using headings, bolded text, and bulleted lists.
Domain 5: Applicability
The fifth domain described strategies for implementing CPGs, whether potential resources for applying the recommendations had been considered, and whether the CPG presented monitoring criteria. All the CPGs clearly communicated which illness, type of injury, or patient group they were developed for. For example, they specified whether their purpose was to be used as treatment instructions, in the prevention of pressure ulcers, or in patient supervision.
Six EMS CPGs described how various recommendations could be applied in practice and when it was inadvisable to use them. One ED CPG described staff shortages, peaks in patient flow, and patient disease severity as examples of when the guideline had limited use. One ED CPG stated that no increase in costs was expected as a result of using the guideline. In the remaining CPGs, no organizational or economic factors that might influence CPG use were presented.
Domain 6: Editorial independence
The final domain concerned funding and how it influenced CPG content. None of the CPGs indicated whether external financing, funding, or competing interest had affected its development. In one ED CPG, information about external funding was presented and explained as being used to cover personnel costs for CPG development.
Discussion
The results demonstrate that there are currently no Swedish CPGs in use that support ECNs in performing comprehensive patient assessments in emergency care settings. No clear connections to scientific evidence were identified in the guidelines or methods used in evidence collection. The criteria for CPG development were not consistently documented. This study indicates that various CPGs are used in Swedish emergency care settings, but no CPGs for comprehensive patient assessment are available. Most of the CPGs in use focus on assessing patients’ biomedical care needs. This is in line with previous research showing that biomedical issues are given priority in emergency care and that caring for other aspects of patients’ well-being is not perceived as equally important.8,9,36 This may indicate that patient-centred care is lacking in emergency care. To provide patient-centred care, ECNs must consider all aspects of the patient’s life their assessment. 37
A lack of patient-centred care is not a new phenomenon in emergency care.2,38 Research has identified difficulties involved in ECNs taking a caring approach. 39 This tendency might be reinforced by the fact that ECNs do not always consider patients’ life situations as essential components of their assessment. 24 Patients who need emergency care are dependent on ECNs. Therefore, it is necessary to apply a caring attitude in encounters with patients to understand their unique needs 9 and be compliant with the professional foundation of nursing care values and responsibilities. 1
Comprehensive assessment is vital since it influences patients’ quality of life. 40 For example, comprehensive patient assessment could reduce readmissions among elderly patients with multiple comorbidities. 41 This kind of assessment could also help to identify psychological needs relating to sleep problems, depression, stress, melancholy, or suicide risk. 42 Finally, assessing existential care needs is important because illnesses may cause patients to lose hope and diminish their will to live. 43 However, comprehensive patient assessment is also a challenge. It is more complicated to evaluate the patient. 41 It is more expensive 40 and time-consuming 41 than simply assessing patients’ biomedical care needs. Nonetheless, comprehensive patient assessment has the potential to increase patient safety and reduce risk.41,44
In the present study, some CPGs were found to address adverse events, such as pressure ulcers, fall injuries, and malnutrition. Such events are preventable, but patients may be unaware of the potential risks. Therefore, it is the responsibility of the ECN to prevent such risks. However, underlying beliefs, attitudes, and contexts may support or obstruct patients’ participation and make it more difficult to prevent adverse events. 45 To counteract this, increased awareness is needed throughout the organization. Increased awareness of the most common factors associated with adverse events will enable targeted actions, reducing the risk of care and treatment complications and the frequency of readmissions. 23
The results also revealed ambiguity concerning the intended target population of CPGs. One consequence of this is that CPGs may be used for unintended or incorrect patient groups. This could harm patients, causing them to miss treatments or receive incorrect treatments. 46 Patients seeking emergency care must be able to rely on the ECNs’ competence and provision of safe care. However, patient assessment in emergency care settings combined with decision-making in chaotic environments present challenges from a patient-safety perspective, 44 and adverse events related to medical issues are common in emergency care. 47 Therefore, constructing systems that prevent adverse events constitutes a crucial component of patient safety.
The current study found that only one CPG included patient perspectives. This low number may be due to CPG developers not perceiving patient contributions as relevant to CPG issues or failing to see value in having representatives from patient associations contribute their experiences. 48 However, not including patient perspectives when developing CPGs is counterproductive since patients are the focus and objects of the care proposed.
To provide good quality and safe emergency care, ECNs must consider both nursing and medical care needs, and their assessment must be evidence-based. However, the results of the present study indicate that emergency care is deficient in developing evidence-based CPGs. Previous research has highlighted similar deficiencies, such as the flawed development of CPG content and its lack of connection to scientific literature. 28 A possible reason for this is limited knowledge among managers and employees in emergency care regarding how to construct evidence-based CPGs. Whatever the reason, there is a risk that assessments may be performed without any evidentiary foundation. 37
The findings of this study also illustrate how CPG development has mainly been executed by senior executives and management physicians. This means that ECNs, who are responsible for patient assessments in everyday care, are generally not included in CPG development. Thus, it is likely that other aspects of patient care needs are not given the same importance as medical care needs.8,36 This highlights the necessity for ECNs to be included in the development process as they can provide insight into patients’ unique care needs. Safety in emergency care can only be ensured through responsiveness to individual patients’ situations by confirming and understanding the patient’s needs. 7
In summary, ECNs currently do not focus on comprehensive patient assessment, including patients’ psychological, social, or existential care needs. We can speculate that one reason for this is that CPG developers are not involved in everyday emergency work. Consequently, Swedish emergency care has a shortage of evidence-based CPGs, and patients are not being provided with the best care and treatment.
Limitations and strengths
This study has some limitations. For instance, only 17 (17.5%) of the 97 emergency care organizations replied to our invitation to participate. This is not optimal, as it influences the generalizability of the results and the conclusions that may be drawn. Thus, comprehensive patient assessment and scientific support for CPGs may exist to a greater extent than demonstrated in the current research. Another limitation is that the authors were clearly not specific enough in their request for CPGs since many of the CPGs provided had to be excluded in the screening process. The initial request and informational letter could have been more specific.
All EMS and EDs in Sweden were invited to participate in the present study. However, the deficiency in the register of existing EMS and EDs presents a limitation, as it made it difficult to identify the managers of the organizations. Therefore, some EMS and EDs risk being excluded. However, a strength of this study is that, to the best of the authors’ knowledge, it is the first national cross-sectional survey on this topic. It should be noted that this study was conducted in 2017; however, no other studies on this topic have been published in the last four years. In addition, the organizations that participated in the present study cover the entire Swedish geography and include both large and small organizations. Another strength of the study is the use of the AGREE II instrument, which is a validated instrument made for specific purposes for the quality appraisal of CPGs. The results are likely transferable to other countries and healthcare contexts with similar organizations, education, and staffing.
Conclusions
The findings of this study demonstrate that there are currently no Swedish CPGs in use that support ECNs in performing comprehensive patient assessments in emergency care. This indicates that patients’ physical, psychological, social, and existential needs are not addressed in the same way as patients’ medical needs. The results also demonstrate that the foundations for evidence-based CPGs are weak and cannot confirm whether the ECN has the prerequisites to assess patients and refer to treatment, such as home-based self-care (i.e. ECNs are less able to conduct evidence-based practice). Such recommendations require the ECN to conduct a comprehensive patient assessment and identify the presence of various care needs. Additional research is required to better understand the importance of comprehensive patient assessments and the prerequisites for such assessments.
The findings of this study have implications for ECNs, managers, and educators who are involved in emergency care. ECNs should actively seek more effective ways of highlighting and safeguarding patients’ various care needs using more comprehensive guidelines. This means that ECNs need the resources to create, update, and implement CPGs in everyday emergency care. Managers should take responsibility for developing high-quality, evidence-based CPGs for comprehensive patient assessment. Educational efforts are essential to extend ECNs’ knowledge of CPG development and the critical evaluations supporting comprehensive patient assessments.