
Abstract
The application of master’s degree competence in nursing practice has been a hot topic of debate in various forums in recent years. International findings suggest that nurses with master’s degrees can make a positive contribution to the quality of services and patient safety, and an association has been suggested between higher education in nursing and a reduced mortality rate in hospitals. Therefore, this study aimed to investigate registered nurses’ (RNs’) experiences with how a master’s level education affected their work in the specialist health service. An inductive qualitative study design was used. Data were collected through focus group interviews with 18 participants in five groups and analysed using content analysis. This study is reported in accordance with COREQ. The results showed an ‘expectation gap’ between the RNs with master’s degrees and their managers. Our findings also reflected the RNs’ ambivalent experiences of being both a threat and a resource. The application of the competence describes the desire to utilise and recognise the master’s qualification. Furthermore, expectations for the future in the specialist health service were focussed on more evidence-based practice. The results of this study highlight that enhanced competence is a priority area aimed at meeting current and future needs for evidence-based practice and effective services. Clinical master’s degrees place emphasis on both the RNs’ clinical skills and their ability to obtain and apply new knowledge.
Background
The application of master’s degree competence in nursing practice has been a hot topic of debate in various forums in recent years in the Scandinavian countries 1 as well as internationally. 2 Master’s degree competence enhancement is in line with the international Bologna Process that is applicable to bachelor’s, master’s and doctoral degrees. International findings suggest that registered nurses (RNs) with master’s degrees are making a positive contribution to the quality of services and patient safety, and an association has been suggested between higher education in nursing and a reduced mortality rate in hospitals. 3 , 4 Conversely, the nursing profession has expressed concern that master’s degrees do not meet the needs of the health services, and the added value of such a qualification is being questioned. 1 Critical questions are also being asked about whether a master’s degree is needed to perform effective and responsible nursing, and whether all specialist RNs should have a master’s degree. A number of official Norwegian documents describe a need to increase competence within health-related subjects. 1 According to The Norwegian Association of Higher Education Institutions, the added value of a clinical master’s qualification is that the RN obtains advanced knowledge in clinical assessment, interaction and leadership, as well as academic competence. 1
Specialisation in nursing differs from one country to another, both with respect to the type of specialisation and length of the postgraduate programme. 5 In Norway, RN education is on a bachelor’s degree level. Some universities offer anaesthesia/surgery/intensive care at a master’s degree level, whereas other academic institutions have post-graduate education between bachelor’s and master’s level. The Norwegian Association of Higher Education Institutions, Wangensteen et al. and Cotterill-Walker assert that a nurse who is educated to master’s degree level is better equipped for analytical thinking and interdisciplinary collaboration. 1 , 6 , 7 In addition, Cotterill-Walker argues that the benefits of a master’s qualification can include enhanced skills in communicating nursing issues and more opportunities for professional and personal growth. 7 The master’s qualification improves RNs’ ability to function at a higher clinical level, exercise leadership, and influence decisions. Cotterill-Walker further emphasises the importance of these for RNs’ capacity to understand and use medical terminology and to practice critical thinking, which facilitates communication with doctors and other professionals. 7 Generally, critical thinking encompasses the concepts of problem-solving, decision-making, inference, divergent thinking, evaluative thinking and reasoning. 8 This is considered crucial for the professional development of nurses, and, according to Gerrish, McManus and Ashworth, it is important for RNs to demonstrate their own personal competence and to make this evident to others for the purpose of reinforcing nursing as an academic discipline. 9 A particular component of critical thinking is described as the ability to apply research findings to practice, provide evidence-based care and increase responses to change in the patient condition. 7 Report number 16 to the Norwegian Ministry of Education and Research describes how, more than ever before, there is a need for a competent population that is trained to think critically in relation to their own and others’ professional practices, whilst also employing scientific methods and ways of thinking to solve problems and critically evaluate sources. 10 RNs are required to adopt a knowledge-based approach and to work in line with recognised evidence-based knowledge. 7 , 10 Evidence-based practice can facilitate the development of new improved solutions and increase the health service’s credibility. 9,11 Casey et al. conclude that the competence attained from a master’s level education is under-utilised despite positive findings about its usefulness. 12 Drennan concludes that taking a master’s degree significantly improves nurses’ knowledge, making them better equipped to change practice, communicate, contribute to teamwork and resolve problems/address challenges. 13 The Coordination Reform in Norway, is communicating the responsibility for the community health services and the specialist health services, with hospitals. This reform will place a significantly greater responsibility on the specialist health services to provide guidance to the community health services. 14 Consequently, more expertise is needed at all levels. An RN with a master’s degree in advanced clinical nursing can ensure a higher level of patient satisfaction and better continuity of care since they are more accessible than doctors. This in turn can improve cost-effectiveness. 12
In summary, the research describes how enhancing competence impacts patient safety, patient satisfaction and the professional and personal development of RNs. There are a number of benefits to RNs taking master’s degrees, but the question of whether the RNs feel that their competence will be utilised in the specialist health service (secondary care), may also be a key issue. A literature review shows that there is a lack of international research examining RNs’ own experiences of how their master’s degree qualifications are utilised in the workplace. The aim of this study was therefore to investigate RNs’ experiences of how a master’s degree education affected their work in the specialist health service.
Method
The study used a descriptive qualitative design. 15 Data were collected through focus groups 16 and the transcribed text analysed using the content analysis method. 17 The qualitative descriptive design was found to be appropriate for gaining a deeper understanding and investigating the registered nurses’ experiences. 18 This study is reported in accordance with the consolidated criteria for reporting qualitative studies (COREQ). 19
Sample and recruitment
The inclusion criteria for participation in the study were RNs with master’s degrees in the field of nursing or health sciences, who were working or had worked in hospitals in clinical practice with patient contact within the past five years. Participants were recruited through managers at the hospitals. The RNs were contacted after a strategic sample 18 was selected by management at the relevant hospitals. The RNs were sent information letters and gave their consent to participate. When recruitment at the hospitals became difficult due to the low number of RNs with master’s degrees, universities were contacted to find more participants that matched the inclusion criteria. A total of 25 participants were contacted; no one refused, but four were unable to take part due to timing issues and two dropped out due to illness. One participant was excluded after the interview as the participant had not finished their master’s degree and for this reason did not meet the inclusion criteria. The study included 18 informants, made up of 16 women and two men. Fifteen had master’s degrees in clinical nursing, and three had master’s degrees in disciplines such as community health, public health and nutrition/health. Their specialities included anaesthesia, intensive nursing, acute nursing, geriatric nursing and cardiovascular nursing. They worked at four different hospitals and in different wards.
Data collection
Focus group interviews were chosen to gather data on opinions, values and experiences in a complex situation. 16 Focus group interviews are a good method for collecting data when participants’ experiences can be shared and discussed, and can also produce rich data. 16 , 20 A semi-structured interview guide with open-ended questions was used. 16 The questions posed were: ‘Can you describe your experiences since attaining your master’s degree?’ and ‘How do you perceive your department’s utilisation of your master’s level competence?’ A pilot focus group interview was conducted to ensure that the questions addressed the subject of the study. 18 The interviewers also had the opportunity to practise their interview technique. The results of the pilot focus group interview were not included in the analysis.
Three of the focus group interviews were conducted with a maximum of seven RNs, and two interviews consisted of two participants. In accordance with the wishes of the participants, the interviews were conducted at their workplace, as they lived in different parts of the country. The first and the second author participated in the data collection, and shard the roles of moderator and observer which is in line with Jayasekara. 16 The moderator was responsible for ensuring that the discussion stayed on track and that there was reflective and inclusive group interaction. Participants were encouraged to speak freely about the subject in their own words; the goal being to provide rich, detailed and descriptive data. Meanwhile, the moderator and observer consciously tried not to influence the participants. 16 , 20 The median duration of the interviews was 45 minutes, and the data material was captured in a good-quality audio recording. The authors transcribed the recordings themselves shortly after the focus group interviews, and then reviewed the material thoroughly to increase their understanding, knowledge and comprehension of the text, and to facilitate the analysis. 18
Data analysis
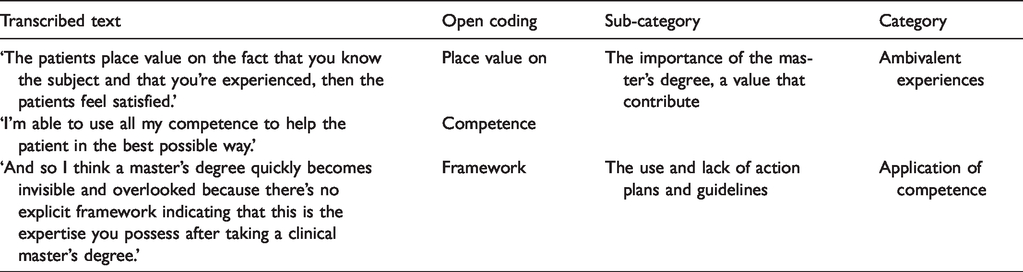
The data were subjected to a qualitative content analysis with an inductive approach, in line with Elo and Kyngäs. 17 The analysis process entailed the material being analysed as a whole in order to safeguard findings and ensure that the analytical process is a true reflection of the interviews and the participants’ experiences. 17 The processing phase entailed selecting meaning units. The organising phase involved open coding, a coding structure, grouping and categorisation. The meaning units were coded, and codes with corresponding content were grouped into sub-categories and generic categories. The manifest content was discussed several times, and it was agreed that each generic category was unique and did not represent the same content. The abstraction led to a latent theme, in accordance with Elo and Kyngäs 17 (Table 1). The results are presented in a tabular format and in running text with quotations from the interviews.
Example from the analysis process.
Ethical considerations
The study was approved by the Norwegian Centre for Research Data (NSD), case number 42234. It was also approved by the data protection officers at the respective hospitals. The principles of autonomy and confidentiality were emphasised, with information given on the right to withdraw. 21 Ethical guidelines were followed throughout the process.
Results
This study aimed to investigate registered nurses’ experiences with how a master’s level education affected their work in the specialist health service. During the analysis the latent content ‘expectation gap’ emerged as a theme. The RNs used the metaphor of the gap, where they considered themselves to be standing on one side while management and the system were on the other. The potential to provide a more professional and comprehensive nursing service to patients was described. The wish was to improve the quality of nursing in clinical practice. They found that their expectations did not always match management’s or other staff’s views on what was needed in the department. Two categories emerged: ‘ambivalent experiences’ and ‘application of competence’, along with underlying sub-categories (Table 2).
Overview result.

Ambivalent experiences
The generic category ‘ambivalent experiences’ reflects how attaining a master’s degree in nursing could be both a positive and a negative experience. The new competence was described as giving RNs greater professional confidence in their dealings with patients and in professional development. They exhibited a dedication to the profession, as well as a desire to provide good-quality comprehensive nursing care for patients. The negative experiences stemmed from others not placing as much value on the master’s level competence as they did.
The importance of the master’s degree, a value that contributes
In the sub-category ‘The importance of the master’s degree, a value that contributes’, master’s degree studies were described as educational, challenging, interesting, exciting and enriching, both professionally and personally. The master’s degree qualification was highlighted as having a positive effect on RNs’ nursing practice in the clinical setting, where they felt they had been providing a higher level of professional nursing care since enhancing their competence. (…) I think I use my competence all the time in patient care, when providing guidance and in discussions with colleagues. Overall, I think I’ve done the hospital and the community a great service. (Interview 5)
Feels like a threat, but also a resource
The ambivalent experiences with the master’s qualification came to light in the sub-category ‘Feels like a threat, but also a resource’. This paradox was manifested in the RNs’ expectations of utilising their professional knowledge and development. Improving the quality of nursing practice and enhancing their competence was one goal. The opportunity to make use of this in their professional development and in projects was another goal, but they also experienced that they were met with indifference. Management and colleagues sometimes regarded the qualification as a threat, since the RNs with master’s degrees were sometimes better qualified than the other staff in the department, with the exception of doctors. The following quotation describes the importance of the master’s degree and the responsibility it entailed, whilst also illustrating the paradox: I can see in our daily work that we need this competence, I feel it’s my responsibility to identify and explain what the patient needs. I don’t think top management see it that way, and I think that’s been the biggest challenge. (Interview 5) (…) if you have a patient on a respirator and you can handle a respirator, it makes no difference if you have a master’s degree or not, because it’s about the number of helping hands and getting the work done. (Interview 4)
Application of competence
This category describes the experiences of returning to clinical practice with newly acquired competence, how this was applied and utilised, and the employer’s desire to utilise and recognise the master’s qualification. Wishes for how the qualification should be used both now and in the future were also described.
Being recognised
The sub-category ‘Being recognised’, describes the desire for the master’s qualification to be recognised and valued in the department. Several of the RNs found that there was no plan for how to deal with the competence they had attained, either in the form of work tasks or pay increases. They described how there was no sense of recognition in terms of feedback from management and other staff in the department. Some expressed the opposite, where their employer had a plan in place that provided for relevant adaptations in the department and financial compensation. Pay was not necessarily the most important reason for enhancing competence, but the following quotation reflects the importance that the RNs attached to the master’s qualification making a difference in the performance of their work: My pay has gone up to reflect my master’s qualification and the wage supplement from my employer, but my tasks haven’t changed. (Interview 2) I know it takes time to change an environment or system … at the hospital they had a strategic plan to encourage people to take a master’s degree. So we did that, and we said what now? Then it was left up to each department, and the head of department says she hasn’t asked for this (…). (Interview 1)
The use and lack of action plans and guidelines
The sub-category ‘The use and lack of action plans and guidelines’ included descriptions of how guidelines and recommendations in the framework documents were implemented at an overarching level in the health trusts, but not necessarily in the department. The respondents found there was a considerable focus on both evidence-based practice in the health trusts and the need for RNs educated to master’s level in the hospitals. However, they saw no conformity between the Ministry’s guidelines and what actually happened in the departments. The mismatch between these guidelines and their experiences in the department is described in the following quotation: They have no idea how to use us. There’s a dualism. Ministries state that we must concentrate on research, quality, knowledge and evidence-based practice – there must be people with master’s level competence in the department. So, RNs acquire these qualifications, and the feedback is often that what we need is staff to do the practical work. (Interview 2)
Looking into the crystal ball
The sub-category ‘Looking into the crystal ball’, describes how respondents hoped master’s level competence could be used in the future. The wish to continue working closely with patients in clinical practice in addition to contributing to efforts to create evidence-based procedures, and to be of assistance in projects and development work in the department, was described. The RNs found that their competence gave them not only a greater ability, but also a responsibility to disseminate knowledge to their colleagues and management. It also gave them more professional weight when justifying nursing choices. Their wish to implement evidence-based practice despite considerable work pressure in clinical practice was highlighted. I wish that there was more leeway to have an evidence-based approach and at the same time work in clinical practice. (Interview 4) (…) I think there’s a mismatch between what the university offers and what the working day entails. Those of us who take a master’s level education are squeezed between the two. (Interview 3) I’m excited about how RNs with master’s level competence will be utilised in the future, because it’s still very new. I find that the university hospital – which is a leading hospital – has no focus on how to use the competence in relation to critical thinking in clinical practice. We need to find our own way to some extent. (Interview 5)
Discussion
The results reflect that the key factor in terms of master’s level competence was used in practice and benefits patients. The ‘expectation gap’ emerged as a theme where the RNs’ expectations did not always match management’s or other staff’s views on what was needed in the department. The value of such a qualification was not always recognised by management. If efforts to enhance competence are to be successful, such competence must be used in practice. 22 , 23 Moreover, when staff are unable to use their relevant qualifications, this reflects an incongruence between their education and their work situation. 24 When the RNs in the study experienced a divergence between their own potential and the tasks, opportunities and challenges they faced, they found this demotivating. Competence enhancement is a managerial responsibility. 24 The results of the present study illustrate the gap that can arise when RNs perceive a failure by management to recognise the usefulness or value of the competence attained from having accomplished a master’s degree.
Meanwhile, RNs had their own expectations for themselves and their responsibility to apply their competence – they did not view this as management’s sole responsibility. The ‘expectation gap’ can be described as non-conformity between the RNs’ expectations and the reality in the department, where they found what was needed was helping hands to carry out the practical work. Is it the case that RNs with a master’s degree find that they are over-educated and superfluous in the department as Støren and Wiers-Jenssen describe? 22 Casey et al. conclude that RNs and midwives with a master’s level education still find that they are over-educated and unable to use their expertise in clinical practice. 12 Yet their newly acquired competence could improve nursing care through better quality and greater cost-effectiveness. 22
It is an interesting paradox that whilst master’s degree competence is a priority area, the value of using the qualification and working with evidence-based projects was little recognised at the final phase – clinical practice. In our study, we identified a potential drain of competence from hospital practice, since many RNs with a master’s degree now work at the universities. This may illustrate the fact that when RNs experience that their competence is not used, they look for other relevant jobs, such as at universities. Conversely, RNs with master’s degrees must themselves be advocates of their newly acquired knowledge and convey how it can be utilised.
The experience of undervalued competence was described. The main goal was that the working day was successfully completed and that there were enough staff to perform the nursing. The findings of this study concur with those of Skogsaas and Valeberg, who describe how clinicians and managers need more knowledge of how master’s level competence can be used. 23 The RNs in the study perceived themselves as pioneers. They had to back up their demands by making specific plans for applying their knowledge, instruction and participating in projects. At the same time, they made it clear that they wanted to work closely with patients. This is confirmed in Andregård and Jangland’s study, which presents the RN as a visionary with a burning desire for change, and an eagerness to identify new pathways and goals in the organisation. 25
The RNs found that master’s level competence enabled them to systematise, reason and not least be respectful of knowledge. Eizenberg showed that RNs with master’s degrees performed evidence-based nursing care better than nurses without this qualification, and that this is emphasised in their education. 26 Utheim and colleagues stress the importance of evidence-based practice in the health service. 27 A lack of organisational structure and culture in the specialist health service is also identified as an obstacle to applying an evidence-based approach. 28 Hole et al. highlight the development of the ability to apply competence as a useful tool. 29
In addition, the master’s degree had given RNs more confidence both professionally and personally, and they also found their competence in critical thinking beneficial for patients, in line with Cotterill-Walker. 7 Drennan states that there is a significant difference in terms of critical thinking between RNs who have completed a master’s level education and RNs without this qualification. 13 Skogsaas and Valeberg, and Shatton et al. confirm that RNs with master’s degrees have more training in critical and analytical thinking. 23 , 30 Aiken et al. identify the association between a higher level of education and patient safety. 3 , 4 Moreover, Teng et al. assert that a higher accreditation level is a prerequisite for patient safety. 31
The findings of The Norwegian Association of Higher Education Institutions 1 indicate that RNs with master’s level qualifications in clinical nursing are particularly well equipped to carry out clinical and more advanced tasks in practice, especially those who also have completed a specialisation in a defined area. According to Gerard et al., 32 nurses educated to master’s degree level are increasingly required to front nursing practice and be able to recognise the potential and limitations presented by technology. Swan and colleagues state that nurses with master’s degrees score far higher on patient satisfaction and cost-effectiveness than doctors carrying out the same tasks. 33 Lerdal regards it as a prerequisite that academisation and clinical practice complement each other for the theory taught in study programmes to have practical relevance. 34 However, a report on specialist RNs in the future describes master’s degrees in nursing education as varying in both quality and content, with differences in focus in terms of clinical placements and structure. This makes it difficult for employers to know what kind of competence an RN with a master’s degree actually possesses. 35
Walter and Curtis conclude that there are no clear parameters for the functional area, title and qualifications of RNs with master’s degree competence in the specialist health service. 36 This may be one of the reasons RNs in this study experienced an expectation gap and challenges. Competence may only contribute to goal achievement when used in a relevant manner, and it is vital that acquired competence is used in practice. 23 The RNs in the study found that their competence benefited patients, and that there is a need to boost knowledge in nursing. They also emphasised the rapid development of society and pointed out that patients make more demands than before and have more updated knowledge regarding their treatment. The RNs were of the opinion that their newly acquired competence helped to satisfy patients’ needs to an even greater degree. This is in accordance with the findings of the Universities Norway (UHR) which concludes that a master’s level education gives added value and greater patient satisfaction for the individual patient. 1
To our knowledge, little research has been carried out either internationally or in Norway that describes the competence provided by master’s studies and the extent to which this benefits patient. Meanwhile, many of the RNs’ collaborating partners have also acquired master’s level competence and this commonality can provide a platform for better communication in interdisciplinary cooperation. In the present study, RNs believed that their competence would increasingly be an integral part of nursing practice in the future. This was based on their experiences in the interviews with the positive benefits of education and competence for patients, nursing practice and for themselves as RNs. They described both positive and negative experiences in respect of the significance of master’s level competence and how it was valued.
Methodological considerations
Lincoln and Guba’s four criteria were used (i.e. credibility, dependability, confirmability and transferability) to ensure the trustworthiness of the findings. 37 Regarding credibility, there were clear inclusion criteria; that the RNs had worked closely with patients and had experience of using their master’s level competence in clinical practice, giving a strategic sample. 18 Those who worked at universities at the time of the interview had worked in clinical practice within the last five years, after completing their master’s level education or still worked part time at the hospital and meet the inclusion criteria. 18 A total of 25 agreed to participate, but seven were unable to participate due to illness. This gave a total of 18 participants, and this was deemed to be a sufficient number in this kind of study in order to elicit depth in the participants’ descriptions. 20 It was planned to have focus groups with three to seven participants. The use of focus group interviews was rearranged as pair interviews in two cases, because of illness. The use of groups with two informants may represent a weakness in the study. However, we considered it more important to include their experiences, and the interviews with two participants provided rich descriptions. 20
The credibility of the study was also ensured by the moderator and the observer having clearly defined roles during the interviews and to ensure that everyone’s voice was heard. 16 Furthermore, dependability was partly ensured by all the participants answering open-ended questions. The use of focus group interviews, with discussions and reflections, strengthens the study. 16 The results categories and sub-categories reflect these discussions. To ensure credibility and transparency a checklist was used at different stages of analysis.19,37 The analysis process is described in detail. It is thus possible to follow the research process so that it is clear how the researchers have arrived at relevant findings, ensuring transparency. 38 The authors have maintained a critical gaze and been conscious of their preunderstanding in order to ensure the credibility of the study. 38 Quotations were used to illustrate the association between the data and the results, strengthening the authenticity and the confirmability of the study. 38 The study was performed in a Norwegian context, and its transferability must be assessed in the light of the fact that the situation of RNs in hospitals may differ across countries.
Conclusions
The expectation gap described by the RNs demonstrates the complexity of the situation when the expectation differs in the department. The application of master’s degree competence and clarification of the learning outcomes are important. Both management and RNs with master’s level competence have a responsibility. Enhanced competence is a priority area aimed at meeting current and future needs for evidence-based practices and effective services. Clinical master’s degrees place emphasis on both the RNs’ clinical skills and their ability to obtain and apply new knowledge. Further cooperation between the universities and clinical practice to develop the content and aims of master’s degree competence, is needed.
Further research is also needed to investigate managers’ opinions about master’s level competence in clinical practice and how enhanced competence impacts on patient safety in the department.
Footnotes
Acknowledgement
We wish to thank all the RNs who generously shared their experiences with us.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.