
Abstract
Social contextual circumstances have an influence on parental transition, and social support has been shown to facilitate the transition to parenthood, among other states. Further knowledge is, however, needed to explore how partners of pregnant women use their social networks during pregnancy. Therefore, the aim of this study was to explore how partners of pregnant women use their social networks when preparing for childbirth and parenting. Within this study, a social network is defined as social connections such as family, friends and significant others. In total, 14 partners (expectant fathers and co-mothers) were interviewed. Data were analysed using qualitative content analysis. EQUATOR Network guidelines and the COREQ checklist were applied. The analysis resulted in one theme of meaning: Partners use their social networks to receive social support, which facilitates understanding about how to prepare for childbirth and parenthood, which was described through three sub-themes. The results highlight the importance of social networks for partners when preparing for childbirth and parenthood. Professionals should aim to strengthen and extend partners’ social networks and access to social support. This could be done not only to support partners to attend parental classes, but also to participate socially as well as engage with other expectant parents within the classes.
Introduction
Pregnancy is the biological path to parenthood, during which an expectant parent usually faces a considerable number of new issues in life. Naturally, the pregnant woman and her partner encounter diverse issues on their way to parenthood. For the pregnant woman, pregnancy is a physiological process, 1 which may lead to a partner feeling excluded because they were not expected to be involved during pregnancy or in early parenthood. 2 However, both expectant parents will experience psychological and social contextual experiences and change. 1 Entering parenthood, or going through the transition to parenthood, includes changing one’s habits of mind and way of living for both the pregnant woman and her partner. 1 Consequently, the parents’ expectations, levels of skills and knowledge, emotional and physical well-being, and social contextual circumstances greatly influence the transition to parenthood; thus, social support is essential. 3
The fact that social contextual circumstances have an influence on parental transition 3 is not unexpected. Humans’ social lives are organised within different social groups characterised by ties of varying strength. 4 Social networks and especially the social support provided within such networks have a positive effect on mental health. 5 , 6 Beyond this, the function and structure of social networks have an effect on interpersonal behaviour through the provision of social support, social influence, social engagement and attachment and access to resources and material goods. 5 Furthermore, social support has been shown to facilitate the transition to parenthood, 7 lower the risk of depression among fathers 8 and strengthen the perceived quality of the parents’ relationship six months after childbirth, 9 just to mention a few effects. In this study, a social network is defined as the web of social relationships that surround an individual and the characteristics of the ties associated with it. 10 Furthermore, social support is defined as support from friends, family or significant others within the individual’s social network. Such support is based on a need for kinship/friendship that each person develops based on congruent expectations. 11 It is widely recognised that social support is a valuable component of strengthening positive outcomes in families experiencing transitional life events, such as the parental transition. 12 , 13 This is essential knowledge since both the pregnant woman and her partner’s relationships with social connections within the network (such as family, friends and significant others) are affected by parenthood, 14 while the significant life change represented by the transition to parenthood sometimes results in social isolation. 3
It is widely known that the expectant mother and her partner use their social networks for learning when preparing for childbirth and parenthood. 15 Not all social support is, however, positive for the parents, since ‘social visiting’ by family members may interfere with new parents’ pursuit of privacy and family bonding. 16 Berkman et al. 5 claim that the structure of network ties influences a person’s health through the provision of different kinds of support. Nevertheless, even though heteronormative ideas of a family still exist, such norms are being challenged as an increasing number of lesbian couples enter a mutual motherhood. 17 In those cases, the partner of the pregnant woman is not the one sometimes acknowledged as the given father, but the so-called co-mother instead. Most previous research on pregnant women’s partners’ experiences of childbirth has focused on fathers, compared to research on the experiences of co-mothers. Previous research based on co-mothers’ experiences from midwifery care reveals that they perceive a lack of parental classes that include only the perspective of lesbian motherhood. 18 For healthcare professionals who care for expectant parents, further research that includes both fathers and co-mothers as partners is needed to increase the knowledge about partners’ social networks during pregnancy. In the following sections, the term ‘partner’ refers to both father and co-mother within the current study. To sum up, social support is valuable for both pregnant women and their partners during the transition to parenthood, but more research is needed to explore how partners of pregnant women use their social networks during pregnancy. Therefore, the aim of this study was to explore how partners of pregnant women use their social networks when preparing for childbirth and parenting.
Method and design
For this study, the authors used a qualitative design with interviews. 19 An inductive approach was chosen to gain insight into the partners’ descriptions.
Setting and participants
The current study was conducted in a county in southwestern Sweden with approximately 280,000 inhabitants and composed of urban, suburban and rural districts. There is one county hospital that has approximately 2,700 births annually. There are also 15 antenatal clinics, all of which were included in the recruitment process. During a prenatal assessment at gestational week 25, midwives in the antenatal units enrolled partners who met the inclusion criteria: (a) partners of expectant first-time mothers with singleton pregnancies; (b) the intention to give birth at the county hospital; and (c) the ability to both understand and speak the Swedish language. Strategic sampling was used to ensure variation in relation to participants’ age, place of residence, education and place of birth. In total, 14 participants were included and contacted by the first author via telephone. Prior to the commencement of the interviews, the participants were provided with written information about the study as well as the interviewer’s profession (midwife/PhD student).
Data collection
Qualitative interviews were used to gather the participants’ descriptions of how they use their social networks when preparing for childbirth and parenthood. All interviews followed a guide that consisted of both an open-ended and follow-up questions. The open-ended question was used to let the participants describe how they used their social network in their preparation for childbirth and parenthood: How have you prepared for childbirth and parenting? The follow-up questions were used to encourage the participants to broaden their descriptions and describe their experiences of the social support they had received from their social networks: Could you explain how you experienced it? and What has it meant for you in your preparation for childbirth and parenting? Before each interview, the interviewer contacted each participant to describe the interview procedure and to let them choose a time for the interview. All interviews were conducted individually via telephone during gestational weeks 36–38, between November 2014 and February 2015. The purpose of conducting the interviews by telephone was to increase the level of comfort for the participants, as this method was assumed to be less time consuming for the participants. 19 All interviews were conducted by the first author, audio-recorded and transcribed verbatim and lasted between 30 and 60 minutes. To test the interview guide and procedure prior to the interviews, two pilot interviews were carried out. During these interviews, the interviewees were also able to describe their experiences of answering the questions and being interviewed on the telephone. 19 The results of the pilot interviews confirmed that the interview guide, procedure and technical equipment were suitable for responding to the aim of the study. The pilot interviews were not included in the analysis for the present study.
Data analysis
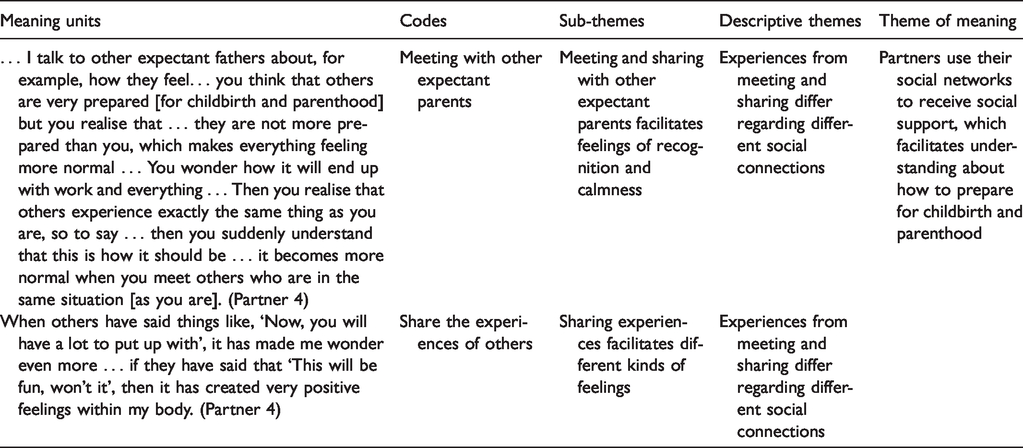
Data analysis was conducted using qualitative content analysis with an inductive approach, as described by Graneheim et al. 20 At the beginning of the analysis, each transcript was read and re-read several times by the authors independently. This was done to ensure that both authors understood the content and would capture the essential structure of the interviews. During the analysis, similarities and differences that answered the aim of the study were searched for in the data. These similarities and differences were described in sub-categories. Thereafter, descriptive themes were identified. These descriptive themes gave direction and nuance to the data. Finally, a theme of meaning arose, which illuminated the comprehensive interpretation of the text. The differences between descriptive themes and the theme of meaning are related to their characteristics and the kind of research question they answer. 20 Two of the authors participated in the different steps of analysis. All three authors, with differing experiences of qualitative research, participated in discussions concerning the analysis and in the process of writing the text. All researchers were female. The analysis process is shown in Table 1.
Overview of sub-themes, one descriptive theme, and theme of meaning, with examples of the analysis process.
Ethical considerations
Prior to data collection, the participants were provided with information about the study and their right to withdraw their consent to participate at any time. The information was provided both in verbal and written formats, and none of the participants chose to withdraw participation. The participants gave their written informed consent, and they were guaranteed the confidentiality of any information they provided in the interviews. To protect the identity of each participant, the findings are partly expressed using anonymous quotations. No one other than the researchers had access to either the electronic files from the interviews or the transcribed material, which were kept in a safe, locked location, both during and after the research. The clinical head of service for the antenatal units gave permission to undertake this study. The Regional Ethical Review Board in Gothenburg, Sweden, approved the study (Dnr: 197–14). The consolidated criteria for reporting qualitative research (COREQ), a 32-item checklist for qualitative research, 21 were followed.
Results
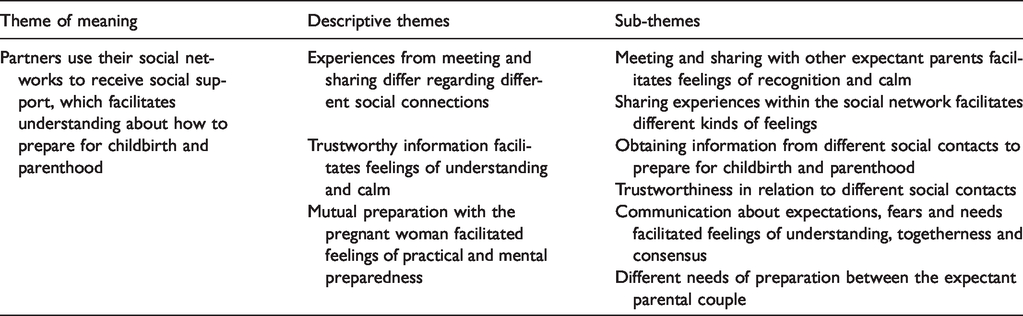
In total, 14 partners (both expectant first- and second-time fathers and co-mothers) participated in the interviews. They were between 26 and 39 years old, represented urban, suburban and rural districts, and their place of birth was Sweden (13 participants) or another European country (one participant). The participants had a high school and/or university education up to seven years. During the analysis of the transcribed interviews, one theme of meaning was defined: Partners use their social networks to receive social support, which facilitates understanding about how to prepare for childbirth and parenthood. The theme of meaning was described through the following three descriptive themes: Experiences from meeting and sharing differ regarding different social connections; Trustworthy information facilitates feelings of understanding and calm; and Mutual preparation with the pregnant woman facilitated feelings of practical and mental preparedness (Table 2).
Overview of themes of meaning, descriptive themes and sub-themes.
Theme of meaning: Partners use their social networks to receive social support, which facilitates understanding about how to prepare for childbirth and parenthood
According to the participants’ descriptions, they used their social networks to gain social support, which facilitated their understanding of how to prepare for childbirth and parenthood. The social networks described by the participants included their partner (i.e. the pregnant woman), family, friends, colleagues or significant others. The participants explained that the social support received could create feelings of increased understanding that made the participants feel more prepared and their approaching parenthood more real. This was especially so when the participants had the opportunity to meet and share experiences with other expectant parents or people they had a close relationship with. This meeting and sharing could reassure the participants and make them feel calm regarding approaching parenthood. Besides this, mutual preparation with the pregnant woman could make the participants feel more prepared for childbirth and parenthood since it contributed to feelings of togetherness between the expectant parental couple. At the same time, the participants reported that people they had a less close relationship with were more likely to share negative experiences from childbirth or parenthood.
Experiences from meeting and sharing differ regarding different social connections
According to the participants, meeting others and sharing experiences differed, depending on how close the different social connections were. On the one hand, meeting and sharing with other expectant parents or social connections with close ties facilitated feelings of recognition and calm, which could be understood as social support, which was reassuring. On the other hand, social connections with less close ties were more likely to share negative experiences of childbirth or parenthood, which precipitated negative feelings among the participants.
Meeting and sharing with other expectant parents facilitates feelings of recognition and calm
According to the participants, meeting other expectant parents created opportunities for them to take part in others’ experiences of pregnancy, the upcoming childbirth and parenthood. This created feelings of recognition among the participants because it made them feel that they were not the only ones expecting a child. Such feelings made the participants understand their situation as being normal. In addition, when other expectant parents shared their experiences of preparing for childbirth and parenthood, it confirmed the participants’ feelings of making the right preparations at the right time.
The participants valued meeting other expectant parents since such meetings offered them opportunities to discuss practical issues for which they needed to prepare. Such practical issues could be about several issues: what the participants needed to purchase and preparing for the baby’s arrival or parental leave. This meeting and sharing with other expectant parents also facilitated feelings of calm for the upcoming childbirth and parenthood among the participants. Participants who did not have other expectant parents within their own social networks experienced that the parental classes offered by midwives within maternity care could be an opportunity for them to create such social connections. In cases where the participants did not have the opportunity to attend such parental classes, they experienced it as negative since they were unable to meet other parents, which they had expected to do. … I talk to other expectant fathers about, for example, how they feel … you think that others are very prepared [for childbirth and parenthood] but you realise that … they are not more prepared than yourself, which makes everything feel more normal … You wonder how it will end up with work and everything … Then you realise that others experience exactly the same thing as you are, so to speak … then you suddenly understand that this is how it should be … it becomes more normal when you meet others who are in the same situation [as you are]. (Partner 4)
Sharing experiences within the social network facilitates different kinds of feelings
The participants described that they used their social networks to share experiences concerning pregnancy, childbirth and parenthood. Taking part in other’s experiences could contribute to different feelings among the participants. For example, it could increase their interest in listening to how preparation for childbirth and parenthood could be carried out. This listening could facilitate feelings of knowledge among the participants. In the following, the participants’ interest in engaging in mutual preparations for childbirth and parenthood together with the expectant mother could be facilitated as well. The participants experienced that people with whom they had a close relationship were more willing to share experiences that contributed to their understanding. Sharing experiences with social connections that the participants had close ties with were also more likely to confirm the participants’ abilities to manage their own situation, compared to sharing with other, less-close social connections. The participants experienced it as easier to speak with people with whom they had a closer, more solid relationship.
Occasionally, people shared their own negative experiences from childbirth and parenthood with the participants. Such negative experiences were described as ‘horror stories’ by the participants. Furthermore, the participants experienced that some people more or less appointed themselves as experts on childbirth and parenthood-related issues. People who did this were mostly people with whom the participants had less-close ties. To manage such horror stories, the participants tried to choose which experiences and information they should remember and which that they should try to forget. When others have said things like, ‘Now, you will have a lot to put up with’, it has made me wonder even more … if they have said that ‘This will be fun, won’t it’, then it has created very positive feelings within my body. (Partner 4)
Trustworthy information facilitates feelings of understanding and calm
The participants used their social networks to obtain information about childbirth and parenthood. Such information was obtained in the process of preparation, and the trustworthiness of the information differed in relation to the different social contacts used.
Obtaining information from different social contacts to prepare for childbirth and parenthood
The participants described that they used their social contacts (i.e. their pregnant woman, relatives, friends, colleagues or significant others) to obtain varying information about pregnancy and birth, pregnancy-related physiological changes of the female body, how to help the expectant mother manage physiological changes during pregnancy, food recommended during pregnancy, foetal development in the uterus, and how to support the mother during birth (i.e. massage techniques, pain relief and emotional or reassuring support). The participants also used their social contacts to obtain information about the needs of the newborn child related to breastfeeding, formula, diapers and caring; parental leave issues; baby buggies; how to keep the baby safe during car transport; how parenthood would affect their daily lives; and influence on the parental couple’s relationship. The participants described that increased knowledge about such issues facilitated feelings of preparedness and calm.
On the other hand, they expressed a need for more information about possible complications during childbirth (i.e. premature births; caesarean sections; partum-related haemorrhage; vaginal ruptures; and breastfeeding complications), as well as for information about how to care for the child practically. Unsatisfactory informative support needs could cause feelings of uncertainty. How we should act at home and … how often they [the babies] should get bathed and so on … we haven’t talked about that [with healthcare professionals] … I do not feel prepared … I feel very insecure … I think I will have to ask my parents … afterwards, when the baby is born … what if there will be skin rashes … and what about the food … how can I see when the baby is not well … stuff like that … (Partner 14)
Trustworthiness in relation to different social contacts
The participants expressed a need for obtaining information through sources that were trustworthy. They thought that people within their social networks most often could provide trustworthy information, especially those who were expecting a child or who already had small children. Sometimes, the information obtained was unexpected to the receiver. I have talked with my friend, for half an hour or so. [He said] hug her and cut her nails so she will not tear your skin with them … it was different from what I expected … but I have decided that I will just stay close to her and hold her hand [during birth] … I have never been in such a situation before [as birth]. (Partner 3)
Mutual preparation with the pregnant woman facilitated feelings of practical and mental preparedness
The participants explained that their partner (i.e. the pregnant woman) was part of their social network, whom they depended upon in their preparation for childbirth and parenthood. According to the participants’ descriptions, they received social support from the pregnant woman when preparing together with her. Such support facilitated feelings of practical and mental preparedness among the participants. Occasionally, the participants had different needs of preparation compared to the pregnant woman.
Communication about expectations, fears and needs facilitated feelings of understanding, togetherness and consensus
When the participants were able to share in the pregnant woman’s expectations, fears or needs for the upcoming birth, the result was often an increase in the participants’ understanding of how they could support the woman during birth. In such situations, the participants were able to take part in the preparations that the pregnant woman had made for childbirth and parenthood. In that manner, the participants were able to engage in issues that the woman had read about or obtained from her social network or professionals. Some participants experienced this as positive because it increased their own knowledge and facilitated feelings of togetherness with the pregnant woman. In addition, the participant and the pregnant woman could develop a mutual mental model (or consensus) for parenthood, based on the communication between them. This was especially so when the communication concerned issues about parental leave or childrearing.
Occasionally, the participants were unaware or uncertain about what was possible to communicate with the pregnant woman. From time to time, the participants were unwilling to tell the pregnant woman about their own needs, feelings or experiences of pregnancy, the upcoming childbirth or parenthood. This was because the participants did not want to burden or worry the pregnant woman. … obviously, it is really important that you [the expectant parental couple] have a consensus about what will happen … so we have talked a lot about the time afterwards [after birth] and prepared us for that … such talks have been going on continually during the pregnancy. I want us to do this together … so that we will become materially, mentally and physically prepared. Material and physical preparation means that we have prepared everything that we need … yes, everything between a fever thermometer, bed, changing table and a trolley … mental preparedness means that you have made yourself set to make a change since it all will end up with another person within this family. (Partner 7)
Different needs of preparation between the expectant parental couple
The participants described that they sometimes had different preparation needs for childbirth and parenthood compared to the needs of the pregnant woman. Most commonly, the pregnant woman was more willing to prepare in early pregnancy, compared to the participants who started to prepare in later pregnancy. On the other hand, the participants also stated that they expected the pregnant woman to be the one who should be responsible for the preparation. At the same time, the participants described that they sometimes prioritised the pregnant woman’s need for talking about her experiences of the pregnancy, her need for preparation and having control above their own needs. The partners’ needs could be about focusing on the ongoing employment, for example. These different needs between the expectant parental couple could lead to frustration and conflicts between them. She is very organised and … she is searching for facts. I am more … what should I say … I take it all for granted … I understand anyhow … that’s what is a little difficult between us … I do not feel as stressed in that, compared to what she is, and that has caused … some adversities, so to speak … probably you could say small conflicts … nothing serious but a moment of irritation. (Partner 11)
Discussion
The main finding of the present study was that partners use their social networks to receive social support, which facilitates understanding about how to prepare for childbirth and parenthood. Previous research has revealed that pregnant women and partners use their social connections for learning. 15 The fact that partners use their social networks to prepare for childbirth and parenthood is valuable knowledge for healthcare professionals who care for partners of pregnant women, since parents’ levels of skill and knowledge affect the transition to parenthood. 22 In the views of the participants within the current study, their increased understanding about how to prepare for childbirth and parenthood made them feel more prepared and convinced that the upcoming parenthood was real. The results highlight the value of partners having social connections that provide social support during pregnancy. The transition to parenthood involves changing habits of mind and thinking for the parents. 1 Perceiving oneself with knowledge about how to prepare for childbirth and parenthood might influence the parents’ expectations, which include that the expectant parent has an influence on the transition to parenthood. 1 The partners within the current study stated that sharing experiences within their social networks generated feelings of recognition because it made them feel that they were not the only ones expecting a child. It also made them perceive their own feelings as more normal, which could be described as reassuring support. 23 , 24 This was especially so when they shared experiences with other expectant parents. In situations where the partners did not have other expectant parents naturally within their social networks, they wanted to get into contact with other expectant parents through parental classes within midwifery care. This is valuable knowledge for healthcare professionals who care for pregnant women and partners since professional support for partners during pregnancy has previously been confirmed as facilitating contact with other expectant parents. 18 However, for expectant parents to be able to extend their social networks to include other expectant parents, it is vital that such classes are offered to meet the desires of this cohort. This is because group norms and identities may exist that prohibit group members from interacting and developing positive ties within the group. 4 According to the results of the present study, the partners were willing to engage in preparations for childbirth and parenthood. They wanted to gain information that was trustworthy. Therefore, healthcare professionals who care for expectant parents should make every effort to meet the needs of the partners as well. The results of this study can assist healthcare professionals in their further knowledge about how partners use their social networks and experience the social support received when preparing for childbirth and parenthood. Besides this, the results can serve as a reference for healthcare professionals about how to provide partners with opportunities to extend their social networks during pregnancy.
The results of the present study show that social support that included communication with the pregnant woman could result in the development of a shared mental model between the expectant parents. This shared mental model could be understood as ‘integrative power’, which is the ability of the couple to gather their joint power. 25 According to Berkman et al., 5 even deeper than support are the ways that social relationships provide a basis for intimacy and attachment that have meaning not only for relationships between spouses but also among more extended ties. Previous studies have shown that both partners and expectant first-time mothers perceive that professional support during pregnancy will create a feeling of togetherness within the expectant parental couple, as well as access to other expectant parents. 18 , 26 This could be understood as professional support that could strengthen the parental couple’s joint power and extend their social network. Therefore, the results of this study could contribute further knowledge to healthcare professionals on how to focus care interventions on extending partners’ social networks during pregnancy. This could be done through parental classes, for example, since the results show that partners who lack a social network that includes expectant parents gain from meeting with other parents during such classes.
The current results revealed that social support from the pregnant woman could facilitate practical and mental preparedness between the partners. On the other hand, the partners sometimes experienced themselves as having different preparation needs compared to the pregnant women. This could cause frustration between the expectant parental couple. Occasionally, the partners put their own needs of expressing their experiences or thoughts on hold to prioritise listening to the experiences of the pregnant woman instead. Apparently, the social support that the expectant parental couple could provide each other was a challenging act of balance. The partners’ need (or choice) not to prioritise their own needs but to prioritise the pregnant woman’s needs might be a source of growth for ‘disintegrative power’ between the parental couple. Such power is an ego-centred power that disintegrates other forms of power. 25 Therefore, partners should have access to support that facilitates their abilities to handle the act of balancing between their own and the pregnant woman’s needs. Such support has previously been shown to be provided by midwives within antenatal care. 18 , 26
However, becoming a parent involves changing relationships within the social network. The social network surrounding the expectant parents is a large system embracing different sub-systems like the dyads of father/mother or co-mother/mother, parent/foetus, parent/infant, parent/grandparent, grandparent/infant and others. These sub-systems could be described as subjects that influence the parent from the outside. 27 According to Mercer et al., 28 this means that family functioning and health status are affected by these external influences. Parents’ emotional and physical well-being have an influence on the transition to parenthood, 22 and partners who perceive higher social support during pregnancy also perceive a higher quality of couple relationship, six months after childbirth. 9 This indicates that partners are in need of a social network with ties that provide different kinds of support to better handle the challenges that arise with parenthood. What is the best way of meeting the needs of the partners in practice? Nationally, in Sweden and in several countries internationally, expectant parents are cared for within midwifery practice. Bryar and Sinclair 27 claim that theories or models for midwifery practice should contain the following concepts: the person (the woman, child, partners and others), health, the environment and midwifery. Subsequently, midwifery practice occurs within a complex social context, and it is important for midwives to focus interventions on strengthening couple relationships and parents’ feelings of worthiness. 29 Previous researchers have, for example, suggested counselling and support not only for the pregnant woman but also for her partner, to decrease the risk of postpartum depression. 8 Besides this, professional support for partners during pregnancy has been revealed as strengthening the parental couple’s ability to communicate with each other, as well as to feel togetherness. 18 However, some pregnant women or partners might suffer from a lack of social connections who are able to provide them with social support. Further exploration, therefore, is needed to gain more knowledge regarding this issue.
Methodological considerations
The number of participants included in the current study was deemed satisfactory since the strategic sampling ensured variation among the participants, and data saturation was achieved. For data analysis, a qualitative content analysis 20 was considered appropriate. The different steps in the analysis process were performed jointly, as well as individually, among the authors, which enhanced the credibility of the study. 30 To establish dependability, the same author conducted all the interviews, which followed the same interview guide. This was formulated with the intent to minimise the risk of a change in the interview technique. To increase the confirmability of the study, the different steps of analysis have been presented within tables. In addition, quotations have been presented with numbers showing which participant gave which quotation, to allow transparency of the reporting of the results. When considering the transferability of the findings, 30 it is important to consider that the participants were a limited number of partners in a limited region in Sweden. However, the participants included were considered representative of descriptions of how partners use their social networks during pregnancy both nationally in Sweden and internationally. Altogether, this contributes to the trustworthiness of the study. 31 However, using the telephone for data-collection interviews might have been challenging for the research process and could be considered a study limitation. This is because doing so makes it impossible for the interviewer to analyse body language or facial expressions, for example. On the other hand, using the telephone for data-collection interviews has been proven to increase the level of comfort for both the interviewer and the participant, which could result in a more relaxed interview. 32 In the present study, at the end of each interview, the interviewer asked the participant about his/her experience of being interviewed via telephone. Several of the participants stated that they found it as follows: comfortable, time-saving and/or relaxed. Nevertheless, a mutual assumption among the authors was that the interviews were rigorous and met the aim of the present study. For this study, data were collected between 2014 and 2015, which could be seen as a study limitation. This is because in recent years, it has become more common that expectant parents use the internet as a source of information. 33 , 34 Therefore, it is important to consider that partners might use the internet differently in 2020 compared to 2015. However, the results from this study showed that the participants used social connections on the internet when preparing for childbirth and parenthood, which is in line with previous research 33 , 34 and therefore should be considered as a study strength. The results from this study highlight how partners use their social networks when preparing for childbirth and parenthood, and there are reasons to believe that partners use their social networks in a similar way in 2020, compared to 2015. Nevertheless, the results from this study emphasise the value of partners having a social network when preparing for childbirth and parenthood. The results could be used by healthcare professionals in their further understanding of how to focus on care interventions and professional support to strengthen and extend partners’ social networks and access to social support during pregnancy.
Conclusion
The results from the current study highlight the value of the partners of pregnant women being well connected with a social network that includes social relationships that provide a basis for social support when preparing for childbirth and parenthood. Such social support should consist of opportunities for the partners to meet and share with others and gain trustworthy information, as well as prepare mutually with the pregnant woman. From the partners’ descriptions, it could be concluded that such support is provided from solid relationships with close ties (i.e. the pregnant woman, friends and family), as well as from social relationships with less-close ties (other expectant parents included within a parental class, for example). However, the structure of different partners’ social networks differs, since some partners explained that they lacked access to other expectant parents. Therefore, healthcare professionals should support expectant parents not only to attend parental classes (i.e. parental groups) but also to participate socially as well as engage with other expectant parents within the classes. Subsequently, the results of this study contribute knowledge about how healthcare professionals can focus interventions on strengthening and extending partners’ social networks and access to social support during pregnancy.
Supplemental Material
sj-pdf-1-njn-10.1177_2057158520943379 - Supplemental material for How partners of pregnant women use their social networks when preparing for childbirth and parenthood: A qualitative study
Supplemental material, sj-pdf-1-njn-10.1177_2057158520943379 for How partners of pregnant women use their social networks when preparing for childbirth and parenthood: A qualitative study by Caroline Bäckström, Therese Larsson and Stina Thorstensson: for the Groupe de Réflexions sur la Cardiologie Interventionnelle in Nordic Journal of Nursing Research
Footnotes
Author contributions
Caroline Bäckström: conceptualisation, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, software, validation, visualisation, writing the article which is an original draft. Therese Larsson: conceptualisation, formal analysis, funding acquisition, methodology, validation, visualisation, writing the article which is an original draft. Stina Thorstensson: conceptualisation, formal analysis, funding acquisition, methodology, supervision, validation, visualisation, writing review and editing. All of the authors made substantial contributions to the conception and design of the study, analysis and interpretation of data, as well as drafting and/or revising the article critically and approval of the version to be submitted.
Acknowledgements
The authors wish to express their gratitude to the partners who participated in the interviews. We also wish to thank the funding sources as well as the heads and midwives at the antenatal centres in the geographical area where the study was conducted, who approved the study and assisted in the valuable recruitment of participants.
Funding
This work was supported by: the School of Health Sciences, University of Skövde; the Department ‘Woman, Child (K3)’ at Skaraborg Hospital Skövde; the Research Fund at Skaraborg Hospital; the Skaraborg Research and Development Council; and the Skaraborg Institute for Research and Development.
Conflict of interest
The authors declare that there is no conflict of interest.
Supplemental data
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.