
Abstract
A divergence exists between registered nurses’ (RNs’) intention to document together with the patient and their actual documentation practice; a practice that also diverges from official intentions of patient participation. This study aimed to explore and describe RNs’ reflected experiences on patient participation in nursing documentation. A descriptive qualitative study was conducted based on three focus groups with 14 registered nurses from an acute medical ward. Content analysis and conversational analysis were performed. The reporting adhered to the COREQ checklist. The findings showed that nurses made little mention of patient participation in nursing documentation due to challenges in meeting both the patients’ expected needs and nurses’ needs. However, patient participation was important for time accurate and summative nursing documentation. This study adds to a critical debate on patient participation and contributes to a practice-based understanding of the challenges that registered nurses experience concerning patient participation in nursing documentation.
Background
Patient participation is a core concept in official international and national steering documents within the healthcare system.1,2 The World Health Organization describes patient participation as being closely related to patients’ rights and patient safety. 1 Within nursing, the concept of patient participation has been explored in reviews, 3 in concept analyses4,5 and from nurses’ 6 and patients’ perspectives. 7 An integrative review showed a passive approach to patient participation on medical wards due to patients’ unwillingness and nurses’ confusion around expectations and roles. 3 Patient participation is a complex concept 4 with multiple understandings. In a concept analysis it was concluded that patient participation in nursing practice could be defined as an established relationship between nurse and patient, a surrendering of some power or control by the nurse, shared information and knowledge, and active engagement together in intellectual and/or physical activities. 8 Nurses’ explicated patient participation in terms such as: an interactional process, mutuality, patients as partners, negotiation based on interpersonal procedures, and focus on resources.5,6 Nationally, in Denmark, patient participation is prominent and operationalized as ‘the patient’s experience is being involved in decisions’ and that ‘the patient’s knowledge of his own health situation is accounted for in the care trajectories’. 9 However, a national yearly report on patient satisfaction states that only half of the patients held that the health professionals invited them to participate in decisions regarding their own care and treatment. 10 Patients’ experience of participation in decisions was found to be increased by ‘bedside reports’ 11 or bedside blackboards with clear goals for nursing care. 12
Documentation of patient care is fundamental to communicate the current status of a patient’s individual needs and responses to care. 13 Like patient participation, nursing documentation is also explicated as a tool for improving patient safety. 13 Nationally, nursing documentation is subjected to specific governmental standards that outline its purposes and mandatory content. 14 These standards state that nursing documentation is a working tool for registered nurses (RNs) to enhance continuity in nursing care. In addition, it is supposed to outline conducted and planned care as well as relevant observations of the patient’s conditions, to include the information delivered to the patient and the identified nursing problems. Besides, nursing documentation should serve as data for quality and research purposes and as a basis for decision making in cases where patients complain about issues related to treatment and care. 14
Existing knowledge on patient participation and nursing documentation showed that RNs spent half of their working hours on documentation, which gave rise to a dilemma between time being together with the patient and time spent on documentation. 15 Even when it was possible to carry out documentation as an integrated part of the nursing care inside the patient’s room, RNs found it difficult to share their attention between the patient and the computer. 15 Nursing documentation in electronic health records was found to benefit nurses’ time together with the patient, to reduce administrative time and documentation errors.16,17 However, research also indicated that electronic health records might displace the focus to answering the computer’s question instead of addressing the patient’s questions and uncertainties, 15 and the latter should be a prerequisite for patient participation. Also, others found a lack of patient resources, abilities and judgements in nursing documentation, where a neutral objective description was favoured.18,19 This was further underpinned by the finding of the patient’s perspective as comprising only 3% of the documentation, while organizational information and instrumental interventions made up the rest.20,21 Overall, a lack of the patient’s perspective in nursing documentation is well documented and, even though RNs raised patient participation as important for nursing documentation, 22 patients did not always experience it. 10 Documenting and sharing the patient’s perspective on care and treatment was expected to be a prerequisite for enhanced patient participation. Nevertheless, only 33% of the RNs expressed the view that they involved the patient in documentation, though 65% of the RNs stated that it was possible to carry out documentation as a part of direct patient care. 23 No studies were found which addressed this specific discrepancy, which led to the motivation for initiating the present study. Hence, its aim was to explore and describe RNs’ reflected experiences on patient participation in nursing documentation, because this knowledge might add possibilities for the improvement of patients’ experiences of participation and enhance clinical decisions based on their preferences.
Methods and design
A qualitative descriptive design was applied to explore RNs’ reflected experiences on patient participation in nursing documentation. The consolidated criteria for reporting qualitative research checklist was applied to ensure the best possible reporting of the study. 24
Setting
The study was performed at an acute medical ward at a Danish university hospital, with 15 single bedrooms, each with a computer with direct access to the patient’s electronic health record. Twenty RNs, with bachelor’s degrees in nursing, were employed at the ward. The nursing care was organized as primary healthcare, which meant that each RN planned, performed and evaluated all nursing care for 4–6 patients during a shift.
Data collection and participants
Data were collected in three focus groups as this method could provide a broad range of knowledge about nurses’ reflected experiences of patient participation in nursing documentation.25–27 The sampling strategy was purposeful to seek variation in the participants’ age and professional experience in each group to obtain variety in nursing experience. 25 The nurse manager planned the time and place for the interviews, which all had a duration of one hour. In total, 14 RNs participated in three focus groups (n = 6 + 4 + 4), which is a recommended group size when participants know each other and are talking about a well-known topic. 26 The remaining six RNs were impossible to reach due to night shifts, vacation or illness. The RNs had from three weeks to three years of experience on the acute medical ward. Most of the RNs (11/14) were employed at this ward directly after finishing their nursing education, the remaining three RNs had from five to 22 years of experience as RNs.
The first author (PhD) facilitated the focus group discussions and the second author (Master’s degree) acted as an observer. The observer’s role was to record notes on interactions in the group as well as adding supplemental questions. Both were female RNs working full time at the university hospital in research and development activities, and experienced in conducting focus groups. Although employed at the same university hospital the facilitator was unknown to the participants, while the observer was known by the participants, but not directly involved in patient care at this ward. During the focus groups, the facilitator’s role was to stimulate the participants’ discussions in the direction of the focus of the study according to a prepared facilitator guide including topics and open-ended starting questions. 27 The initial question was, ‘Will you tell me about your experiences with documentation inside the patient’s room?’ The RNs’ experiences of patient participation in nursing documentation were explored through discussions concerning their reflections on where and when they carried out documentation. This was due to the underlying assumption of enhanced patient participation when documentation was carried out inside the patient’s room.
The focus groups were audio-recorded and transcribed verbatim, including notes on pauses, voice levels, other sounds and simultaneous speech. The data material consisted of 59 pages.
Data analysis
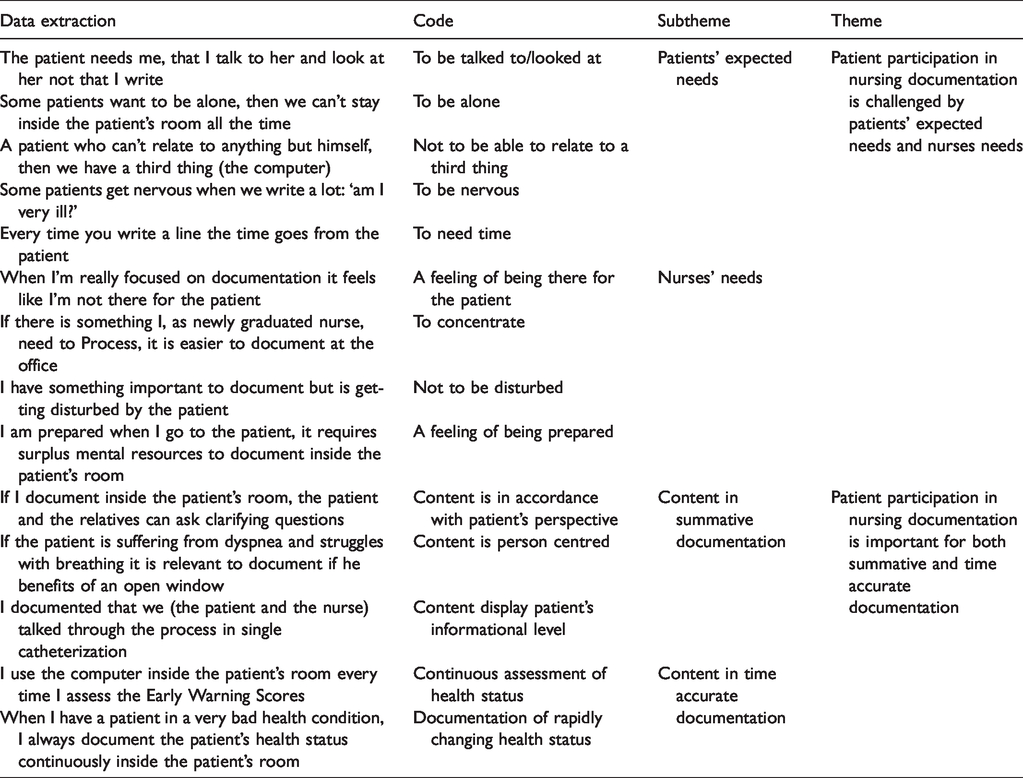
A systematic analysis was performed in order to convey the participants’ reflected experiences in a coherent and useful manner. 25 The systematic performance of content analysis was inspired by Graneheim and Lundmann28,29 and involved a back-and-forth movement between the whole and the parts of the texts. First, the authors read the interview texts several times to get a sense of the whole. Next, they independently coded data extractions representing aspects related to patient participation in documentation. Subsequently, the codes were linked and formulated into subthemes which further constituted the themes (Table 1). 29 The formulation of subthemes and themes included a low level of interpretation and provided a description that stayed close to the data.25,28 The qualitative description was expanded with conversational analysis, 30 in which the data were systematically searched for conversational features such as emotional expressions, turn-taking and laughter. An investigation of the features in their context enabled an interpretation of the RNs’ values and priorities 30 to be made (Table 2). While there is no description without interpretation, the descriptions depended on the researchers’ perceptions and sensitivities, 25 which needed to be discussed in order to reach consensus. This process encompassed bridling and reflexivity and was aimed to support rigor. 31 Focus groups were conducted in Danish and the quotations were translated with care to sustain the messages. In the presentation of findings ‘(1/1)’ indicates focus group one/participant one etc.
Examples of data extractions, codes, subthemes and themes from content analysis.
Example of analysis of the conversational feature, Laughter, showing how analysis of expressions followed by laughter could illuminate registered nurses’ (RNs’) professional values.
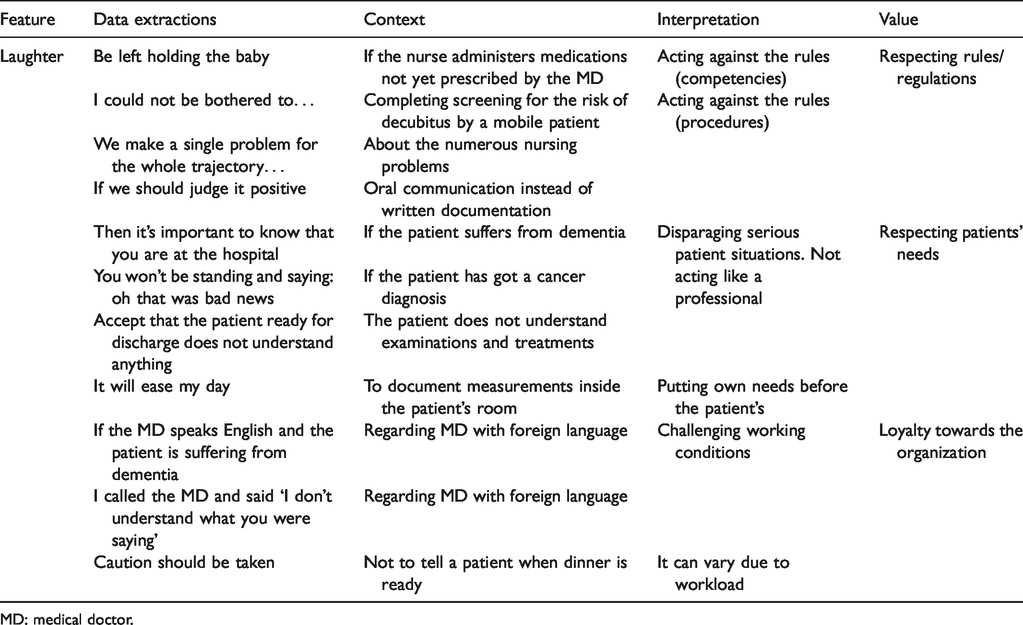
MD: medical doctor.
Ethical considerations
The study was registered at the North Denmark Region’s list of ongoing research projects (id-number: 2019-59) and conducted in accordance with ethical guidelines for nursing research.32,33 Prior to the study, the participants received written and verbal information about the study. The facilitator and observer were presented as RNs and researchers who were interested in exploring the participants’ experiences. At the beginning of each focus group, the principles of voluntariness, anonymity and confidentiality were summarized and the participants gave written informed consent.32,33
Findings
The analysis revealed that nurses made little mention of patient participation in nursing documentation, which was found to be both difficult and important. This is presented in two themes: 1) Patient participation in nursing documentation was challenged by patients’ expected needs and RNs’ needs and 2) Patient participation in nursing documentation seemed to be important for both summative and time accurate documentation.
Patient participation in nursing documentation was challenged by patients’ expected needs and RNs’ needs
This theme illustrated that patient participation in nursing documentation carried out inside the patient’s room was challenged by meeting the patient’s expected needs and meeting the RN’s own needs, which are presented separately.
Meeting the patients’ expected needs
The choice of documenting nursing care inside the patient’s room depended on the RN’s expectations of the patient’s individual needs, which they described as varying substantially. Most patients were described as being ‘confused’ (1/5) or unable to ‘handle anything else than themselves’ (2/1). As such, patient participation in documentation was perceived as impossible due to the patients’ cognitive status and their expected need to rest in a quiet environment. Some patients became afraid when RNs documented a lot inside the patient’s room as illustrated in the following quotation of a patient saying: ‘oh, you write a lot, is it so bad with me, am I very ill?’ (2/4). In these situations, patient participation in nursing documentation was ignored, because it could disturb and distress the patient, and leave the patient with a feeling of the nurse not being attentive. An RN said: When I am inside a patient’s room, really concentrated on documenting, it feels like I am not present and I do not care for them (the patients) or want them (the patients). One tries one’s best to be present while being inside the patient’s room. (2/2)
Meeting the RNs’ needs
The RNs’ personal situations and needs influenced the ignoring of patient participation in nursing documentation. RNs expressed the feeling that they could be disturbed by the patients as illustrated in the following quotation, When I am documenting inside the patients’ rooms, they (the patients) start talking to me and then I can’t concentrate at all, … ‘Oh! Yes! Okay, What did you say … ’, because … I concentrate when I document nursing care, and then they talk beside me. Then I feel totally NOT caring for the patients when thinking: ‘Can’t you just stay quiet, I need to get this written’. (2/2)
Patient participation seemed to be important for both summative and time accurate documentation
The analysis also showed that patient participation seemed to be a prerequisite for both time accurate documentation during the shift and summative documentation at the end of the shift.
Summative documentation
At the end of a shift, documenting outside the patient’s room enabled the RNs to reflect with colleagues on the content in the nursing documentation and to ‘sum up’ the medical plan. The RNs specified that junior medical doctors often went back and forth several times a day after conferring with senior doctors about the patients’ situations and prescribed more tests or treatments. Likewise, it was possible to sum up RNs’ observations and activities with the patient at the end of the shift, which could induce intensive and emotional discussions among the RNs regarding the appropriate level of detail. As such, the advantage of documenting that a specific patient suffering from dyspnea benefitted from an open window, was followed by emotional expressions such as ‘then we can write ourselves to death’ (2/3). Although such content would require interaction with the patient, the RNs did not make mention of it as patient participation. Similar situations appeared regarding lower-leg oedema in which the discussion encompassed whether the nursing documentation, in the case of the oedema observations, was supposed to contain recommended actions such as, ‘Advise the patient to walk and elevate the patient’s legs’ (2/4), ‘instruct in feet exercises and report to the doctor’ (2/3). Whether these suggested activities were dependent on patient participation were not discussed, because they were quickly raised as being ‘common nursing knowledge’ (2/1) and hence not necessary to document. In addition, they were commented on with the quotation ‘I would vomit if reading such content’ (2/1). As such, the emotional expressions regarding summative nursing documentation revealed disagreements among RNs both regarding documentation of performed versus planned care and regarding the level of detail in care plans. Whether a detailed care plan would require interaction and patient participation was not a part of the dialogue.
When the RN prepared the care of the patients at the beginning of a shift, she read the nursing documentation. When this was done at the office, it implied that the RNs felt more prepared when going to the patient. An RN said, ‘Otherwise I am meeting the patient and it appears as if “Oh, I don’t know anything about your situation”’ (2/4). This quotation showed the value of professionalism in ways of knowing the patient’s situation. However, reading nursing documentation inside the patient’s room was mentioned as a possible enabler for patient participation. The rationale was that this could support patients and relatives to ask questions. In addition, the RN and the patient could set out the plan for the coming hours, which the RNs seem to perceive as patient participation. Reading nursing documentation together with the patient was expressed as a possibility: ‘It would be’ (1/4), ‘We could practice doing that’ (2/1) which indicated that it was a sort of fictive or wished situation that had not happened very often.
Time accurate documentation
A kind of patient participation was required for the immediate and time accurate documentation of biomedical measurements, such as blood pressure or saturation inside the patient’s room during the shift. The reasons for documenting these measures inside the patient’s room were, ‘it is efficient’ (1/3), ‘you save time’ (3/2), which showed efficiency as being a value for the RNs. The quotation ‘it is easy to tell the patient “your blood pressure was fine”’ (2/3) showed that documentation of measurements could include information for the patient, which was perceived as patient participation. In acute care situations, where the patient’s health status changed rapidly, the RNs preferred to document inside the patient’s room too, because it seemed impossible to reconstruct such situations afterwards. In these situations, the rationale for time accurate documentation was the ability to reconstruct the sequence of events in case of later complaint cases. This was expressed in the quotations, ‘I want to cover my back’ (3/1) and ‘it can’t hit me’ (3/4) which meant that the RN could not be accused of not fulfilling her responsibility. This was also the reason for some of the RNs arguing for documenting ‘the patient is sleeping’ (3/2) every second hour during a night shift.
Discussion of findings
Patient participation in nursing documentation was found to be challenged by patients’ expected needs and nurses’ needs but at the same time to be important for both summative and time accurate nursing documentation, no matter where and when this was carried out.
The RNs assessed that the majority of the patients either needed to rest or lacked the resources to participate in documentation. This was due to their unstable condition and decreased cognitive function, which meant that the RN would not disturb the patient or demand participation in nursing documentation. This was supported by Freil et al.’s study of health professionals’ understanding of patient participation, in which it was specified that health professionals, in general, tended to assess patients’ resources to participate in decisions regarding their own care and treatment as inadequate. 34 These findings suggested the necessity for nurses to reconsider patients’ abilities to participate also in nursing documentation.
The RNs emphasized the importance of their physical and mental presence by the patients’ sides, which they perceived was incompatible with carrying out documenting inside the patients’ rooms. This was evident when RNs expressed the view that they were not caring for their patients when they concentrated on the computer instead of on the patient. The importance of RNs’ physical and mental presence with the patient was underpinned by their emotional expressions of the importance of seeing and hearing the patient. This corroborated Kossman and Scheidenhelm’s finding that RNs experienced a dilemma between time spent with the patient and time spent on documenting nursing care, 15 which was also outlined by Björvell et al. as the dilemma between the roles as ‘hands-on clinician’ and ‘secretary’. 35 However, in the present study, the RNs did not explain why their physical and mental presence with the patient was important. According to the understanding of patient participation as ‘involvement of patients’ knowledge in decisions’, the reason might be that RNs’ physical and mental presence provided an opportunity to obtain knowledge of the patient’s preferences, which might enable clinical decisions based on these.9,36,37 Further, Myklebust raised that documentation systems did not support the reporting of patients’ resources or patient–nurse interactions. 21 This indicated that documentation systems did not support documentation of the patients’ perspectives which could further challenge patient participation in nursing documentation. This was in line with Campbell, who suggested that electronic health records displaced RNs’ work processes, for example, the importance of nurse–patient interaction for clinical judgement and action was displaced in favour of focus on the medical plan. 38 This has been further raised to possibly transform RNs’ professional beliefs about cure and care, 38 which meant that nurses could give more attention to the medical plans than to the patients’ needs and preferences. In order to improve patient participation, Freil suggested that increased emphasis on the involvement of patients’ preferences in care trajectories had a huge potential for improved patient participation. 34 These findings suggested the necessity for nurses to continue the dialogue on the importance of the involvement of the patients’ preferences and of the processes of obtaining knowledge of these preferences and how to share them in the documentation systems in order to improve patients’ experiences of participation.
Although patient participation in nursing documentation was uncommon, it seemed to be important for both summative and time accurate documentation, although divergent opinions existed regarding the level of details in care plans. This was underpinned by the RNs’ emotional expressions regarding documentation of detailed and individualized suggestions for care activities which would require interaction with the patient but were judged as common nursing knowledge. The divergence regarding the content in nursing documentation might be enhanced by its multiple purposes. 14 As such, the purpose of using documentation in complaint cases was the reason for the RNs to document every second hour that a patient was sleeping. However, it could be discussed whether this information benefitted either the patient or the nurse. The divergent opinions regarding detailed and individual care plans further underpinned the above suggestions of electronic health records as not supporting the reflection of nurse–patient interaction as important for clinical judgement.21,38 On the contrary, electronic health records were found to support efficiency, because they shaped healthcare towards a calculated, effective and efficient form. 38 Efficiency was further supported by financial incentives, which rewarded activity at hospitals. 39 At the acute medical ward patients suffered from a wide range of illnesses and on this specific ward many newly graduated RNs and junior medical doctors strove to fulfil the stated objective of efficiency in diagnosing and initiating treatment, 39 which also explained their need to concentrate on documentation. Hence, the sparse explication of patient participation in nursing documentation could be explained by both medical 40 (patients’ wide range of illnesses) and social conditions 40 (newly graduated health professionals) despite the ideal physical conditions for documentation inside the patient’s room 40 for patient participation in nursing documentation at the acute medical care ward. This meant that in future activities aimed to improve patient participation physical, social and medical conditions must be considered.
Methodological considerations
Transferability judgement of this qualitative study was sought to be enhanced by the description of the setting and the participants’ educational background. To further ensure rigor, descriptions of data collection and analysis were outlined in detail. Although data collection by focus groups might provide broad and nuanced information of the situation or experience under study, there is a risk of data representing social desirability rather than the reality. This was addressed during the focus groups by asking elaborating questions and asking for specific care situations. In the analysis process, the authors’ experiences and sensitivities were dealt with by use of bridling, slowing down and reflection in order to reach common agreement on themes. 41 This process was important and time-consuming and was aimed to prevent premature closure of the analysis and to support rigor. 31 Triangulation by the combination of content analysis and conversational analysis strengthened the findings 31 and numerous quotations were used in order to demonstrate that the findings were grounded in data. Overall, the study showed that research on complex concepts, such as patient participation, could pose difficulties due to different definitions and understandings and thus the research team endeavoured to be reflexive in all parts of this study, which included continuous self-critique and self-appraisal. 42
Conclusion
Patient participation in nursing documentation was carried out sparingly by RNs and was challenged by meeting the patients’ expected needs and the nurses’ needs at an acute medical ward, despite ideal physical locations for carrying out documentation inside the patient’s room. Besides physical conditions, medical and social conditions as well as the assessment of patients’ ability to participate need reconsideration in order to improve patient participation. Patient participation seemed to be important for both time accurate and summative nursing documentation, which relied on interaction and obtaining knowledge of the patient’s preferences. However, incentives for efficiency as well as electronic health records might impede the documentation of patients’ preferences, which could potentially reduce their involvement in clinical decisions.
This study adds to a critical debate on the concept of patient participation and whether existing electronic health records support official intentions of patient participation, such as decisions based on the patients’ preferences. The study pointed to the need for nurses to reconsider their expectations of patients’ ability to participate. In addition, considerations are needed concerning how knowledge of the patients’ preferences could be obtained through physical and mental presence by their sides and, further, how it could be documented in order to base decisions on care and treatment. Whether patient participation in nursing documentation would enhance clinical decisions based on patient preferences is still not certain. The study illustrated how multifaceted concepts in healthcare, such as patient participation, might be difficult to transform from policy level to direct patient care.
Footnotes
Acknowledgements
The authors want to thank Head Nurse Connie Elbeck Van der Kooij for initiating this study and also all the participating nurses for their willingness to openly share experiences and views on nursing documentation and patient participation.
Author contributions
Study design: MGK, KKV, LJ. Data collection: MGK, KKV. Data analysis: MGK, KKV, LJ. Drafting of manuscript: MGK, KKV, LJ. Critical revisions of manuscript: MGK, KKV, LJ.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.