
Abstract
There is scarce research studying healthcare professionals’ and users’ perceptions in relation to creating coherence in intersectoral collaboration between psychiatric centres and community mental healthcare. Drawing on the discourse analysis framework of Fairclough, this study aimed to explore how healthcare professionals and users could perceive coherence in intersectoral collaboration between psychiatric centres and community mental healthcare. But also to explore their perception of how coherence could be maintained through an intersectoral journey, and what discourses manifested themselves within the field of mental healthcare. Data were collected through 11 focus group interviews, five of which with healthcare professionals (n = 20) and six with users (n = 18). Fairclough’s three-dimensional model for the studying of discourse was used to analyse the transcribed texts. This study is reported in accordance with the COREQ checklist. Coherence in intersectoral collaboration was interpreted to exist in tension between being predominantly steered by the healthcare professionals while the users had a desire to be more involved in decisions regarding their own intersectoral journey. The users were subjected to a paternalistic steering, expressed by the power of the healthcare professionals to select the right efforts as well as the purpose of the users’ journeys. The findings showed that coherence in intersectoral collaboration in general was articulated from an overall discourse of neoliberal governance, with its embedded discourses of rationality and structure, and discourses of linearity, objectivity, paternalism, biomedicine and evidence have a controlling influence on how users should guide themselves based on the discourse of self-care.
Keywords
Introduction
Coherent patient journeys between psychiatric centres and community mental healthcare is viewed as a milestone to be reached within psychiatric treatment in Western societies. The World Health Organization has set as a goal that there must be a coordinated effort for psychiatric treatment and rehabilitation across multiple public sectors such as healthcare, education, employment, judicial, housing, social and other relevant sectors as well as the private sector, as appropriate to each country. 1 At the political level, a higher extent of coherence in intersectoral collaboration in mental healthcare is seen as the key to improving and developing the healthcare system.2–6 Despite such political aims, heightened awareness and numerous initiatives, there are still challenges within and criticisms of the mental healthcare systems due to a lack of coherence within intersectoral collaboration in mental healthcare.3,7,8
Healthcare professionals are responsible for creating coherent transitions for users between psychiatric centres and community mental healthcare, although it is not clear how such a transition should be understood. 9 In Denmark, mental healthcare treatment is organised on a regional level and at the level of community mental healthcare, leading to the specific interest in creating coherence between sectors. Coherence in intersectoral collaboration between psychiatric centres and community mental healthcare is articulated as an ontological practice, as something that exists in reality and must be implemented in a social practice. This can be seen as an expression of a social construct because these notions of reality are based on the perception that a particular reality exists.10,11
In general, coherence in intersectoral collaboration in mental healthcare can be considered from two different perspectives: an organisational perspective or a user perspective. Often, the organisational perspective is seen in the regulatory healthcare agreements which set the framework for health services between government, health regions and community mental healthcare. The agreements are documents including, e.g. descriptions of the available services, programmes, and package pathways. However, should a user perspective be involved, users will often understand their treatment and rehabilitation episodically, where their relation to the healthcare professionals is important for the users’ understanding of and coping with their own recovery process.12–14 Reports on Danish mental healthcare show that some users experience being haphazardly transferred from one department to another in mental healthcare. At the same time, many users seem to have many different points of contact, which increases the complexity for the individual user, who must thus assume a coordinating role between the various sectors.7,15
The healthcare system can be viewed from the perspective of controlled services based on a neoliberal framework11,16 with its main discourses being ‘privatising’, ‘emphasising individual freedom’ and ‘responsibility for own health’. The users are regarded as consumers who seek knowledge about treatment and demand the correct form of help.11,17 Similarly, researchers in Western countries identify dominant discourses in mental healthcare as ‘rational control mechanisms’, ‘effectivity’, and ‘cost benefit’, e.g. customer satisfaction evaluation.18–21 Healthcare professionals and users are caught in institutional silo-style thinking which becomes a barrier to creating coherence in a collaboration that stretches across different sectors.22–25
There exist only a few studies that directly investigate the perspectives of healthcare professionals and users in relation to coherency creation through intersectoral collaboration in mental healthcare.18,20,26–30 These studies highlight problem areas such as: insufficient information sharing across sectors; uncertainty about who is responsible for healthcare before/during/after discharge; as well as coordination and cooperation issues. A few studies show how discourses are unfolded in mental healthcare and municipal contexts, but these studies largely focus on one sector alone.21,31,32 Intersectoral collaborations can be viewed as discourses of multidimensional and social practices which unfold under specific political, socio-cultural, economic and historical circumstances. This study is therefore constructed as a critical discourse analysis to explore how discourses can be practiced in order to sustain the social world and social relations, which inevitably involve uneven and submissive power relations. Identifying the unfolding of discourses can lead to a greater understanding of how coherence is constructed in intersectoral processes from the perception of healthcare professionals and users. Accordingly, this study aimed to explore how healthcare professionals and users could perceive intersectoral collaborations between psychiatric centres and community mental healthcare. But also to explore their perception of how coherence could be maintained through an intersectoral journey, and what discourses manifest themselves within the field of mental healthcare.
Methods
The study’s epistemology focuses on the concept of coherence in intersectoral collaboration between psychiatric centres and community mental healthcare. The social realm is seen as being centred around intersectoral collaboration, where these collaborative structures appear as social practices through which texts are constructed, received and interpreted. Likewise, psychiatric centres and community mental healthcare can be viewed as social constructs, where the subjects appear as social practices through which texts are constructed, received, and interpreted.33–35 In accordance with this, we used a social constructivist framework to analyse healthcare professionals’ and users’ perceptions of coherence in intersectoral collaborations, collected through focus group interviews. The framework considers the real world as a series of social constructs, where language and the way we talk about the world and the things within it constructs the social realm.35,36 Conducting a critical discourse analysis supports us in exploring how discourses can be practiced in order to sustain the social world and social relations, which inevitably will involve uneven power relations.34,37 The consolidated criteria for reporting qualitative research (COREQ) checklist was used for reporting this study. 37
Recruitment and sampling
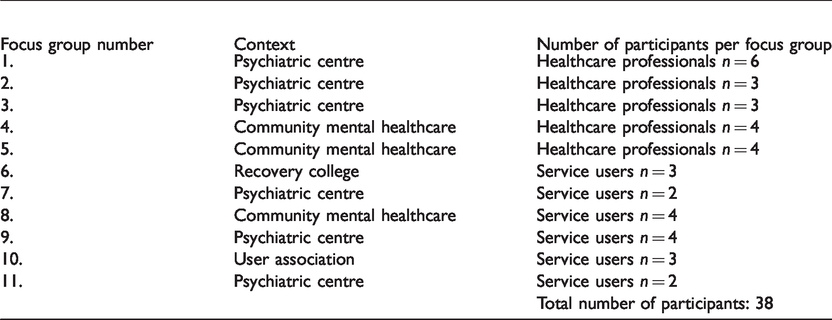
A purposive sampling technique 38 was used to establish contacts and recruit participants for this study. An invitation was sent to the management of the psychiatric centres, recovery colleges, user organisations and community mental healthcare. Management agreeing to take part acted as point of contact and mediated information regarding the study. Healthcare professionals were required to have experience and/or knowledge of intersectoral collaboration between psychiatric centres and community mental healthcare in order to be eligible for the study. Users’ eligibility rested on them having experience with admissions in both psychiatric centres and community mental healthcare. In total, 38 informants agreed to participate, 18 of whom represented a user perspective. Among the healthcare professionals, 12 assisted with treatment in inpatient or outpatient psychiatric centres and eight were employed in community mental healthcare (Table 1).
Overview of focus groups.
Data collection: focus group interviews
Data were collected through focus group interviews. Focus group interviews do not aim to reach agreements or present solutions to the issues of discussion, but rather to obtain different views on the matter. They were therefore a suitable choice as the lively, collective vocabulary can bring out more spontaneous, expressive and emotional views than when using individual interviews. Confronted with sensitive, taboo topics, the group interaction can make it easier to express views that are usually withheld.39,40
Initially, 11 focus groups interviews with four to eight participants in each where planned. However, at the time of the interviews nine subjects dropped out, mainly among the users. Reasons given were, e.g. having a bad day, not being able to be part of a social group, feeling that they could not contribute anything. This resulted in some groups consisting of only two participants. The focus group interviews were conducted with a set time of one hour and were conducted in the environment preferred by the participants.
Two researchers were present at all interviews to conduct and facilitate the process. While one was in charge of creating a dynamic dialogue and being a moderator the other provided assistance in asking in-depth questions and validating the content at the end of the discussions. 40 Before the focus group interviews started participants were once again informed about the aim of the interview: to explore their perceptions on coherence in intersectoral collaboration between psychiatric centres and community mental healthcare. A topic guide was used to organise the interviews (Table 2), but during the interviews the thoughts of the participants where followed through to gain a more nuanced understanding of their views.39,41 The interviews were audiotaped and lasted approximately 60 minutes. The interviews were transcribed by a research assistant and resulted in a total of 250 pages of text for the analysis. All authors were given the opportunity to review and approve these verbatim transcripts.
Focus group topic guide.
The research group reflected on and discussed our positions in the research field. The first author had a widespread experience from psychiatric nursing, and was therefore an important gatekeeper for facilitating the interviews, because of a rather closed and, for many good reasons, protective practice. One author had no experience of psychiatry and one had long experience as a relative. All three researchers are nurses, two with PhDs and the other with a master’s degree.
Data analysis
Fairclough’s three-dimensional model for the studying of discourse was used to analyse the transcribed texts from the focus group interviews (Figure 1). Within this framework, the texts were analysed as 1) text, 2) discursive practice, which involves the production and consumption of the text, and finally 3) as a social practice.34,37,42,43 In Fairclough’s understanding, texts cannot be understood or analysed in isolation. They can only be understood through the meaning contained in other texts and their relation to their social context – discourses are dialectic.37,44–46
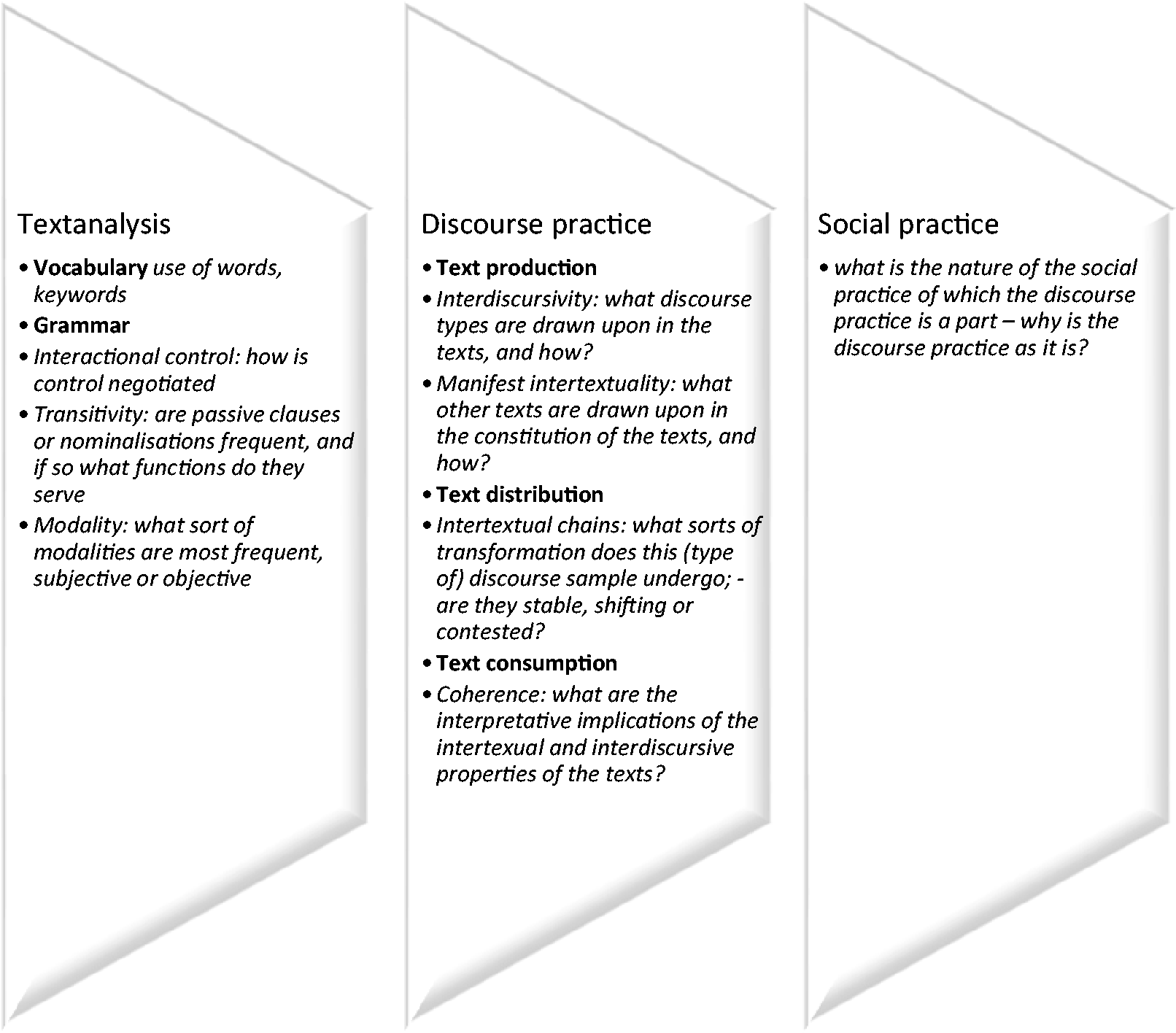
During the analysis, different aspects of linguistics need to be considered in the text. Therefore, the documents were read several times to understand how the participants’ perceptions on coherence in intersectoral collaboration could be textually activated, and what discourses manifested themselves within the study context. The linguistic features of the texts were analysed line by line, word for word. First, focusing on the vocabulary; words and wording describing perceptions of coherence in intersectoral collaboration. Texts expressing this were transferred to an Excel sheet visualising the textual syntactic horizontally, and vertically. Second, focusing on the grammar of the texts. Provisions by clauses, sentence by sentence, line by line, we searched for interaction control, transitivity, and modality in the texts while inspired by Fairclough’s analytical main questions. 34
Ethical considerations
This study was conducted in adherence to the ethics of scientific work. The study was approved by the Danish Data Protection Agency (j. no. 2017-41-5191). According to the Helsinki Declaration 47 and Danish law, 48 no formal permit from a biomedical ethics committee was required, as the purpose of the research was not to influence the informants, either physically or psychologically.
Informed consent was obtained from all participants after they had received verbal and written information about the purpose of the study. The participants were informed that participation could be halted at any time, and that all data would be treated so that no unauthorised person would have access to the material. Data were treated confidentially and anonymously, and audio files were erased after transcription of the material. All other data material will be destroyed after publication. The users in this project can be considered to be vulnerable. Therefore, there are extended ethical commitments in ensuring an equivalent, transparent and participatory research collaboration. 49 For this reason, we met the users one hour before the focus group interviews to have a dialogue about the project and give them plenty of time to consider their participation. We supported the users who did not feel comfortable about being in the room together with us or with the other users to refrain from participation or to come and go as they were able to, even if it meant we had to compromise on the size of the focus groups.
Findings
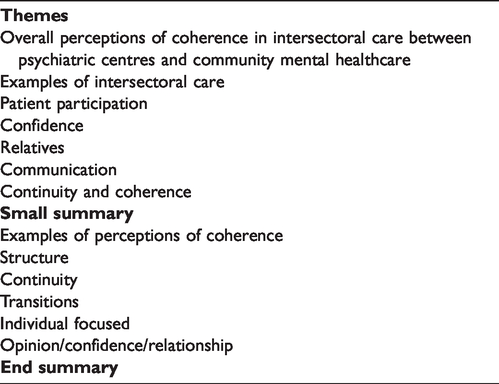
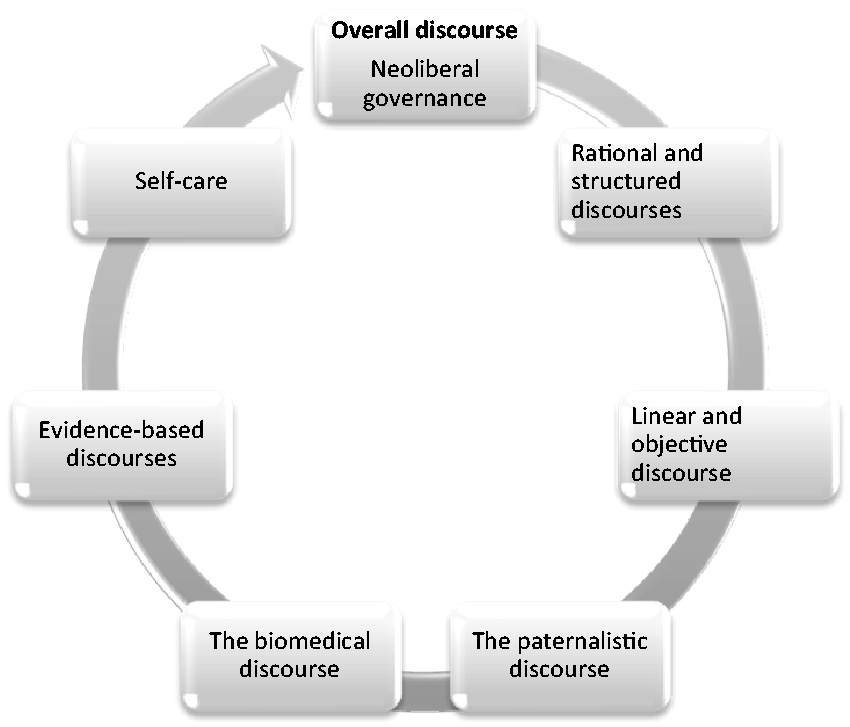
Here we will present the findings from the three-dimensional analysis following Fairclough’s framework of analysis.34,37,42 Text will occasionally be used to illustrate the development of the found discourses (Figure 2), reflecting the participants’ perceptions of coherence in intersectoral collaboration between psychiatric centres and community mental healthcare.
Coding tree.
The vocabulary of the texts
According to the healthcare professionals, the users were subjected to a paternalistic structure, where predetermined methods and structural conditions defined the coherence in intersectoral collaboration. When the healthcare professionals talked about coherence in intersectoral collaboration they used wording such as ‘paranoid thought’, ‘depression problems’, ‘anxiety problems’, ‘ADHD’, ‘autism’, ‘schizotypal’, ‘psychosis’, ‘wrong cast patient’, ‘patient with externalising behaviour’, ‘psychoeducation’, ‘evidence-based’, ‘OPUS manual (outreach treatment of psychotic young)’, ‘problem/aim list’, ‘treatment plan’, ‘interdisciplinary discussions’, ‘status meetings’, ‘SFT group (social skills training)’, ‘healthcare platform’ and ‘recovery as a method to treatment’.
The healthcare professionals also used linear and objective language when discussing coherence in intersectoral collaboration. Regarding the treatment and rehabilitation, the language was distant. The wording around coherence in intersectoral collaboration was steered by the healthcare professionals’ perspectives, as the following quotations show: We have a very specific way in which we work with our patients. (IW 1) The major challenge to the coherence of intersectoral collaboration is that the units that work together have different ways of structuring the work. (IW 1) We work with CBT (cognitive behavioural therapy); the patient is given some responsibility for the treatment and rehabilitation. (IW 3)
The users imitated such professional language when they talked about the intersectoral collaboration, typified by the following quotations: I have had internal depressions since 2001 and followed a package process of psychoeducation programmes, so I will hopefully pass into social psychiatry. (IW 6) I didn’t really get any information on why I was admitted to the closed department. So, I was pretty confused about that. And then the next day I came down to the open section, so I don’t know if it was because there were not enough beds for me. (IW 6) I wanted them to actually know who I was when I came. Not necessarily my whole life story, but at least they know my name. They know what your diagnosis is. (IW 6)
Grammar of the texts: Interactional control
Among the healthcare professionals, interactional control was generally demonstrated by a hierarchical and asymmetrical power relationship, where healthcare professionals know what is best for the users. The healthcare professionals had great confidence in systematic and structured treatment, e.g. as performed through an evidence-based package process. The users were subject to the power of the healthcare professionals to decide what the treatment should consist of and how long it would be expected to last before discharge, as these quotations point to: Poke round, where I was told, ‘You need to be discharged today’. Well, I can’t, I do not feel well. I don’t want to be discharged. ‘It’s something we decide. And you shouldn’t be here anymore.’ Then I have said you can count on you seeing me again in fourteen days. ‘No, we don’t.’ And what did they do, they saw me fourteen days later. (IW 10) I was treated as a product. ‘Take these pills so many times, then you can cope with your daily-life work.’ At that time, I wished to return to the closed ward. There they listened to me, and there they were around me, taking care of me. (IW 10)
Grammar of the texts: Transitivity
The healthcare professionals used a kind of transitivity where they normatively related to what a coherent intersectoral collaboration should be. The intersectoral collaboration that moves between the psychiatric centres and community mental healthcare was described as problematic. Various perceptions and assumptions of user problems were referred to as using different approaches, located between biomedical and social pedagogical knowledge. There was no consensus between the two sectors regarding the aim of coherence in intersectoral collaboration. It was not obvious whether the focus was on the users becoming symptom free and functional and achieving self-care or whether the focus was on the aim to help them live a good life despite their illness. These different perceptions addressed the lack of a common language among the sectors: In community mental healthcare, the employed are social-pedagogically educated. There are also many unskilled employees, and this means that we do not understand the same things about users, and this lack of common knowledge and understanding makes collaboration between psychiatric centres and community mental healthcare difficult. (IW 3) Many of our users have delusions and negative symptoms. They are unable to formulate what they would like. (IW 2)
Grammar of the texts: Modality
Several of the healthcare professionals and users used a linear and objective modality, which implied a structural and organisational language regarding coherence in intersectoral collaboration. They used universal modalities from a psychiatric biomedical understanding and framework, for example, ‘the user does not have the necessary resources for involvement’, rather than subjective modalities, such as ‘I perceive that the user does not have the necessary resources to be involved’. Furthermore, the healthcare professionals used an imperative language which emphasised their position of power, as evidenced by the following: ‘The user must’, ‘the user should accept our offer’, and some truth modality with high affinity, such as: You teach the user about the disease and medicine; it is important that they understand their disorder and treatment. (IW 3) As a healthcare professional I work with the cognitive model which is performed in the way that we have conversations and structure an agenda including what topic we need to address, e.g. medicine. (IW 2)
The users applied a medical and objective language when sharing their experiences from intersectoral treatment and rehabilitation. Most applied a critical modality to professional efforts, such as: In all of the transitions, I have been surprised at how little I actually had an impact on it. Also, in relation to the lack of influence on when I felt ready. (IW 10) They said this is going to take four months and then we are working towards you being on your own legs and then you will be discharged and then you move on to your psychiatrist. And there I could sense from the very beginning that I was not at all prepared for it to go so fast. Because I know how bad it has been and such things. (IW 10) I do not like cognitive therapy, one must be very strong to undergo cognitive behavioural therapy. (IW 7)
Discourse practice
The linguistic analysis identified several interrelated dominant discursive patterns (Table 3). Coherence in intersectoral collaboration between psychiatric centres and community mental healthcare drew on rational and structured discourses, which are subject to what we claim is neoliberal governance. The healthcare professionals’ and users’ self and subjectivity were constituted in power relations and various forms of governance, partly discursively in the form of scientific theories, and partly in the form of technologies developed in various institutions. The rational and structured discourses of linearity, objectivity, paternalism, biomedicine and evidence had a controlling influence on what users should focus on to achieve the discourse of self-care.
Example of the analysis of health professionals’ perceptions.
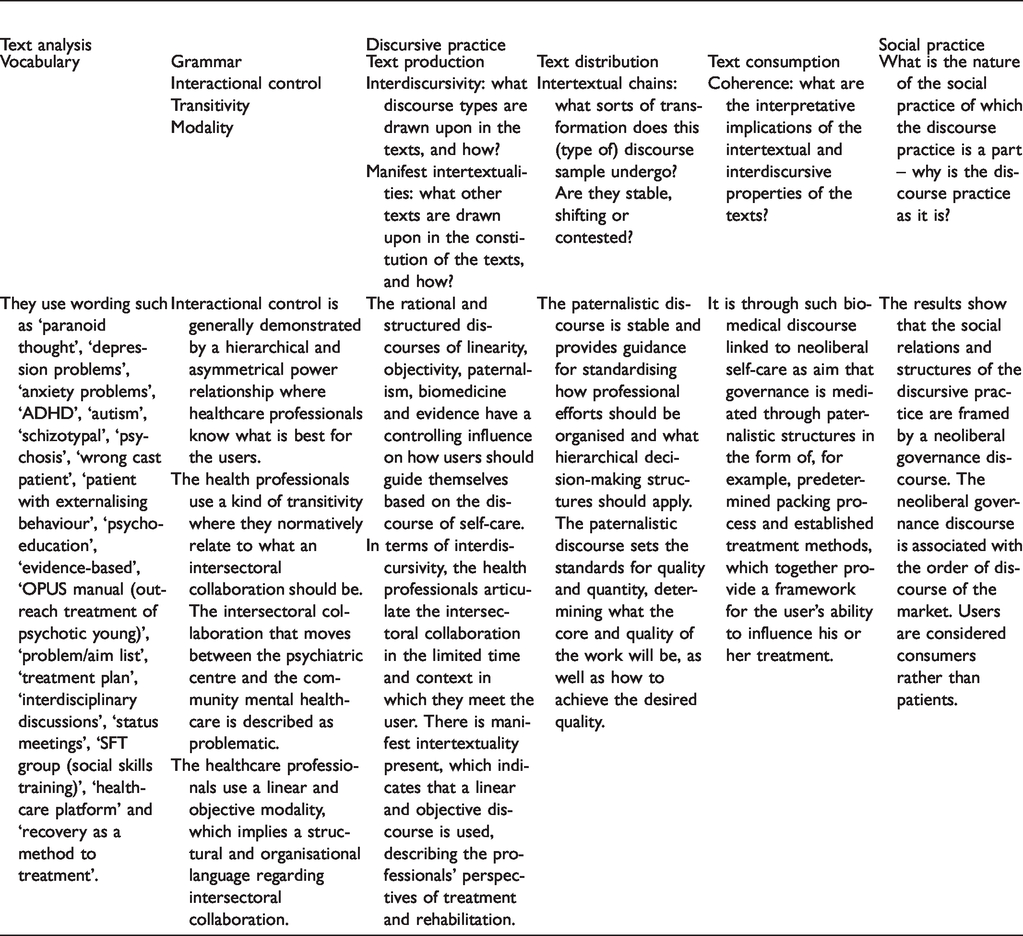
In terms of interdiscursivity, the healthcare professionals articulated the coherence in intersectoral collaboration within the limitations of which they interacted with the users, i.e. limited time in the context. In descriptions of the healthcare professionals’ perspectives of treatment and rehabilitation, there was manifest intertextuality present, which indicated that a linear and objective discourse was used. For example, We have a definite way in which we work with our patients, with CBT (cognitive behavioural therapy). After all, there can often be inconsistencies in what the patients think they need and what we think we can offer. (IW 1)
Users were minimally involved, and they did not perceive being consulted in the transition between the two sectors. ‘For example, network meetings are held without the users’ participation’ (IW 8). This practice, where healthcare professionals chose not to involve the users in network meetings, was an expression of a paternalistic discourse. The paternalistic discourse is stable and provides guidance for standardising how professional efforts should be organised and what hierarchical decision-making structures should apply.
The interpretative implications of the intertextual properties of the texts revealed how the healthcare professionals argued within a biomedical framing, which defined the possibilities of working across different logics in mental healthcare service and social psychiatric institutions. The biomedical discourse was particularly prominent at the psychiatric centres, but healthcare professionals in community mental healthcare, as well as users, also used biomedical language when addressing users’ health problems. It was through such biomedical discourse, linked to neoliberal self-care as aim, that governance was mediated through paternalistic structures in the form of, for example, predetermined package processes and established treatment methods, which together provided a framework for the user’s ability to influence his or her treatment. This reflected the power structures that link political and economic structures to governance of treatment regimens in biomedical and evidence-based discourses.
Social practice
Placing the previous two elements of the three-dimensional model in the broader social practice of which they are a part opens up the possibility to highlight the relation between the discursive practice and the order of discourse that it is part of. Particularly, the institutional and economic conditions that frame the discursive practice is an important part of critical discourse analysis. Our findings implied that the social relations and structures of the discursive practice were framed by a neoliberal governance discourse. The neoliberal governance discourse is associated with the order of discourse of the market. Users are considered as consumers rather than patients. This can be seen as a reflection of, and a driving force in, a change in the wider social practice that Fairclough terms the ‘marketisation of discourse’ – a social development in late modernity, whereby market discourse colonises the discursive practices of public institutions.34,35
Initially, the healthcare professionals wished to contribute to a more coherent intersectoral treatment and rehabilitation for the users. However, the texts reflected that they maintained a treatment structure subjected to a paternalistic and biomedical discourse. This discourse will, according to Woods, 50 award more status, power and authority to the healthcare professionals than perhaps other fields. The discourse’s structural methods are grounded in evidence-based logic and their inherently linear structures enable the economy to be managed and to ensure the lowest possible cost level. Coherence in and across users’ intersectoral journeys is a political goal, which healthcare professionals are expected to meet. 52 There is also an expectation to involve the users in the process, to promote them to take ownership of their treatment and to master their own symptoms. This must be done by actively complying with the professional agreements and by making rational choices, regardless of the user’s mental diagnosis and symptoms. The professionals spoke within discourses of rational (economic) governance, biomedicine and paternalism. The users were subject to a discourse of self-care. We will further discuss the relation to power in the social practice and the coherence in intersectoral collaboration in management and organisation from our analysis.
Discussion
Coherence in intersectoral collaboration was interpreted to exist in tension between being predominantly steered by the healthcare professionals while the users had a desire to be more involved in decisions regarding their own intersectoral journey. The users were subjected to a paternalistic steering, expressed by the power of the healthcare professionals to select the right efforts as well as the purpose of the users’ journey. The healthcare professionals articulated the treatment and rehabilitation through linear and objective discourses that were evidence-based and perceived as providing the best basis for healthcare services to create coherence in intersectoral collaboration. Previous studies, focusing on patient participation in mental healthcare, corroborate our findings of paternalistic steering in which the professionals chose which efforts and goals were the right ones for the users’ intersectoral journeys.21,52–55 Also, in accordance with others,22–25 our findings reflected that the healthcare professionals worked in a silo structure where the long-term perspective of the user’s intersectoral journey disappeared. Much of the existing research mainly focuses on the transition itself, e.g. discharge from regional psychiatric centres to community mental healthcare, and not on whether the long-term intersectoral collaboration is perceived as a cohesive effort.18,20,27,28,30,55 In addition, differences in the laws of psychiatric treatment and of municipal services have led to a situation where the professionals try to meet the law that applies to their specific context, and to a lesser extent focus on what happens next. Our findings implied that discourses of rationality, structure, paternalism, biomedicine and evidence, were the dominant approaches. Self-care was articulated as the ultimate goal for users, and through organisational treatment methods and social pedagogical efforts, users’ self-care was to be improved so that they became independent of professional help and could cope with their own illnesses.
Our findings, and those of others,17,23,56,57 reflect a shift in the Western welfare system, characterised by social scientists as a suppressive neoliberal governance,58–60 or in the Foucauldian description as embedded power with some edifying potential in governmentality. 61 The distinction between these terms is not quite clear in health research. The term ‘governmentality’, taken from Foucault, is often used in order to understand power relations as a constructive process. However, we have used the term neoliberal governance to explain our findings where the paternalistic treatment, healthcare professionals’ power in decision-making, and marketisation of healthcare seemed to become a domineering force in action on a vulnerable group of users.58,59,62 In this approach, the system becomes punitive to the weak and vulnerable, and liberal to the strong and self-reliant. 60 Both approaches involve new forms of practice and new ways of organising the welfare system, where values such as efficiency, self-responsibility, freedom, empowerment, self-help, etc., are central. 16 In healthcare, this development means that users are assigned a more active role. They must not only take responsibility for their own health, they must also be well informed and be able to make ‘free choices’.17,63,64 Users are expected to act as consumers, and in this context also ensure coherence across sectors.21,65 We found, in addition to other studies, that the user became the key to how healthcare should be managed from a political point of view both in terms of efficiency and productivity, and in terms of delivering the desired service.11,32,66
Politicians even hold that the user has become a management tool in the healthcare system, where the aim is to have active, competent and responsible users, and a healthcare system that meets the users’ demands and expectations.
Although the stated aim in policy is to improve coherence in healthcare for the benefit of the users, various ambiguities within the policy-producing institutions tend to maintain a certain order rather than introduce changes. 67 This development is not primarily linked to humanistic ideals, but to the efforts to provide quality and create efficiency in the healthcare system, i.e. neoliberal governance ideals. 58 However, the picture is not clear when you take a closer look at equality and inclusion between the healthcare professionals and users.
The political solution is to assign users a greater responsibility for their own illness and health, ideas which we and others will categorise within a neoliberal discourse.11,32 Within this framework of understanding, users are constructed as clients/consumers of healthcare services, where they themselves must be able to select from an array of options. Rose emphasises that the neoliberal view focuses on an individualisation of the user and his or her problems, which implies that the user must act ‘responsibly’, ‘wilfully’ and ‘controlled’, and ‘agree’ to play the main role in solving his or her own problems. 11
However, this imposes great responsibility to the healthcare professional’s reflexivity to act in a person-centred manner and not on the behalf of the healthcare system or professional ideologies. The view of the user’s role has not always been focused around the user as a consumer, but cast in this role today, the user is expected to be able to act, demand, choose, participate, etc., on their own initiative and on the basis of individual preferences. The change has put users in an active role, which demands that the person contributes and takes charge of his or her own recovery process.68,69 From a political point of view, a liberalisation of healthcare is to be sought competitively, which is happening through an increasing market orientation, where users, through free choice, become an important part of the solution. This modern consumer view is legitimised through the recognition of the user’s own judgment to assess the needed services and select the hospital that will ensure the best treatment. Thus, psychiatric centres and community mental healthcare should market themselves in such a way that users find them attractive and capable of delivering the product that the users themselves consider the correct one. 64
Methodological considerations
In the epistemological perspective, we have used Fairclough’s critical discourse and gained results despite a number of theoretical ambiguities contained in Fairclough’s model of the relationship between language use and broader societal practices. Here, the strength of Fairclough’s approach in performing the analysis made on text-material only, lacks the insight that could be gleaned using historical or structural approaches from, for example, Foucault, Laclau and Mouffe or Bourdieu. It is unclear how to handle the dialectic between the discursive and the non-discursive dialogue, leaving a practical analytical problem with the chosen approach. However, we have supported the trustworthiness and transferability of the study by including quotations as examples of the analysis. In accordance with the social constructivist approach, the results are an expression of how we as researchers, accompanied by Fairclough’s discourse analysis, were co-constructors of the discourses we found, for example, the perspectives of the discourses obtained through focus group interviews from a co-construction approach. According to the constructivists, the aim is to counteract the traditionally objectivist position of the researcher by building meaningful in-depth relationships with participants. With the considerations made in the recruitment and sampling, we sought to obtain in-depth answers in the study, but we acknowledge the possibility that informants may have felt limited when sharing their perceptions, and that healthcare professionals tend to be very disciplined by the dominating ideology. The data consisted of 11 focus group interviews, in some of which we did not manage to obtain our desired number of participants, especially among the user groups. For ethical reasons, we chose to conduct these focus group interviews despite their low attendance, but acknowledge that these groups did not achieve the same dynamic conversation that typically characterises focus group interviews. 39 However, despite the few informants in some of the focus groups, these smaller groups had the unpredicted benefit of including users who did not wish to join a large interview group, and they ended up providing rich answers that helped form the basis of the analysis.
To ensure the validity of this study, we carefully selected a rigorous data material and systematically treated the material to in-depth exploration using critical discourse analysis. The results are in line with existing research and are transferable to clinical practice as they contribute to a greater understanding of the challenges associated with healthcare professionals’ and users’ perceptions of coherence in intersectoral collaborations between psychiatric centres and community mental healthcare. We experienced some users regretting their wish to participate. Several reasoned that they would not talk in a group. To include the most vulnerable users, we could have chosen to conduct semi-structured interviews or observational studies. This would have made it possible to respect the desire for integrity and confidentiality and thus include the most vulnerable groups.
Conclusion
This study has shown how users, despite official aims of making the patient journey more user-driven, can be subject to paternalistic control. The users, as evidenced in discussions by both health professionals and the users themselves, were involved in treatment and rehabilitation on conditions determined by the health professionals who were predominantly focused on treating diseases and enabling the users to live a life independent of professional help. Rather than involving users’ perspectives, the health professionals were focused on treatment and rehabilitation based on evidence, and they relied predominantly on standardised effective approaches. Also apparent was that local discussions about the substance and form of the individual users’ treatment and rehabilitation appeared to be missing within psychiatric centres and community mental healthcare. In order to operationalise the aim of fostering a more coherent intersectoral collaboration, we advise that the current split system, where psychiatry is divided between two sectors, should be combined into one. Healthcare professionals should follow users across sectors rather than being limited by systemic boundaries. In addition, we want to question whether the market-oriented model of self-care is meaningful to the vulnerable groups in society at all. There is a need for humanisation and de-medicalisation of psychiatry, putting the recovery of users at the centre.
Footnotes
Author contributions
KJ was responsible for the coordination, data generation, data analysis, and drafting the manuscript. JF and MBD participated in the iterative analyses, interpretations of the data, drafting the manuscript and revising and approving the final manuscript.
Acknowledgements
Thank you to Associate Professor Tanja Thinggard Andersen and Associate Professor Astrid Reinhardt Birch Nielsen from the Psychomotor Training department of University College Copenhagen, who contributed to the pilot study. Thank you to former programme manager at University College Copenhagen Simon Simonsen, who supported the project. We sincerely wish to thank the service users and health professionals who participated in the study for their hospitality and willingness to share their time and thoughts. The study was financially supported by the University College Copenhagen.
Funding
This work was financially supported by the University College Copenhagen.
Conflict of interests
The authors declare that there is no conflict of interest.