
Abstract
Surviving a cardiac arrest is a tumultuous experience. Although the incidence of cardiac arrest and influencing factors are well researched, little is known of survivors’ experiences as they return home from hospital. This article aims to explore survivors’ experiences of returning home after surviving a cardiac arrest. Four females and 13 males, all independently living cardiac arrest survivors, were recruited using purposive and snowball sampling techniques and participated in individual in-depth interviews over a six-month period. This inquiry follows COREQ guidelines and data were analysed using narrative inquiry where key threads were identified. Findings indicate that a cardiac arrest is a catastrophic event where the survivor has to accept and adjust mentally, physically and socially, often leading to insecurity about the future. The cardiac arrest impacts all aspects of life on return home, including the ability to work and to drive, accepting added medical appointments and medication regimens. Healthcare professionals can learn from survivors’ narratives to support holistic care, considering survivors’ experiences in their transition home and back to reality as a cardiac arrest survivor.
Introduction
Cardiac arrest (CA) is a large public health problem, claiming approximately 300,000 lives in Europe and 3.7 million lives worldwide each year. 1 Global survival rates to discharge among out-of-hospital CA patients who received cardiopulmonary resuscitation (CPR) have increased from 8.6% in 1976–1999 to 9.9% in 2010–2019. 2 There are, however, differences in survival rates depending on location. Europe has an estimated survival rate of 11.7%, North America 7.7% and Asia 4.5%. 2 Although mortality remains high there are positive trends with better education in CPR, bystander participation and the availability of automated defibrillators, as well as improved medical interventions, increasing the number of CA survivors. 3 As the number of survivors rises, the exploration of the survivors’ experiences in the transition between the hospital and the home environments becomes of interest.
Experiencing a CA is a defining moment in the life of the survivor, where their previous reality is compared with their current situation and an altered future. Commonly, survivors’ physical and psychological capacities have changed and the adaptation to a new reality can be a challenge; frustration and dissatisfaction are common in adjusting to this new reality. 4 , 5 Although survivors are considered to have an acceptable quality of life (QOL), 6 , 7 it has long been known that many CA survivors experience anxiety 8 and that insufficient care after the event can amplify the problem. 9 Many survivors of CA have cognitive impairment 10 and experience psychological distress. 8
Often, quantitative research is used to explore QOL using validated tools 6 and survivors report an acceptable QOL. 7 , 11 In comparison, qualitative explorations of the phenomena of surviving CA are few. 6 Qualitative research gives the participant an opportunity to express their views without the constraint of questionnaires and allows depth of experience to come to light that is not exposed in quantitative research. Knowledge about survivors’ experiences will benefit nurses and health professionals in supporting their patients in their transition to the home environment. This article explores the narratives of 17 CA survivors with the aim of exploring their experiences of returning home after surviving a CA.
Methods and design
Stories are an integral part of human life; they create order and string together experiences to form an understandable and meaningful whole. 12 , 13 By telling and re-telling experiences, a greater understanding of the phenomena under study occurs. 14 Clandinin and Connelly 14 and Clandinin’s 15 framework of narrative inquiry (NI) informed this study, as NI is well suited to explore health-related topics with a focus on the individual’s experience of illness. 16 In this framework, the three dimensions of time (where past and present experiences are explored as well as the influence they may have on future experiences), place (where the event happened and where the story is told), and sociality (personal circumstances, feelings, desires and hopes, as well as cultural, social and institutional knowledge), influence the individual’s story. 14 , 15 These three dimensions need to be understood and contemplated; they intertwine and are not separate entities. 15 , 17 Themes are commonly used to describe findings in qualitative research; however, Clandinin’s NI framework replaces themes with the term threads to explore re-occurring feelings and thoughts in the participants’ stories, and like threads they are intertwined and woven within the three dimensions. 14 , 15 The ontological stance of NI reinforces the epistemological assurance that experiences, through the telling of and listening to stories, provide knowledge. 14 , 17 – 19 Narrative inquiry aims to create an engaging text that ‘… resonates with readers so that they reflect on their own lives, their own values and beliefs’, 15 (p.xii) therefore findings from this research provide health professionals with an opportunity to engage in reflection over CA survivors’ experiences and, most importantly, their care needs. This research follows the consolidated criteria for reporting qualitative research (COREQ) checklist. 20
Sampling and recruitment
The study was open to adults who had survived a CA, were living independently in the community and were proficient enough in English to provide written consent and have a conversation. Twelve participants contacted the first author after an article introduced the first author and her interest in survival of CA. A further five participants were recruited through snowball sampling. 21 The number of people expressing interest in participating was more than expected and more than what would be required for NI. However, as all participants fulfilled the inclusion criteria, no participant was denied inclusion in this study. All participants initiated contact with the first author, ensuring their participation was voluntary, and all received a printed information pack, which included information about how to contact support services should they be needed following the interview.
Participants
The study included four females and 13 males, aged 48 to 92 years at the time of interview. Level of education spanned from high school to doctoral studies, and employment was equally broad, including self-employment, home care duties, office work, academia and health professions. The experience of a CA had occurred between three months and 36 years prior to the interview. Twelve participants had experienced an out of hospital CA: eight during exercise (gardening, jogging, surfing, playing golf and team sports) and four during sedentary activities at home or in the community. Five participants experienced their CA in hospital. The participants’ characteristics are presented in Table 1.
Characteristics of participants who were interviewed about their experience of a cardiac arrest (n = 17).
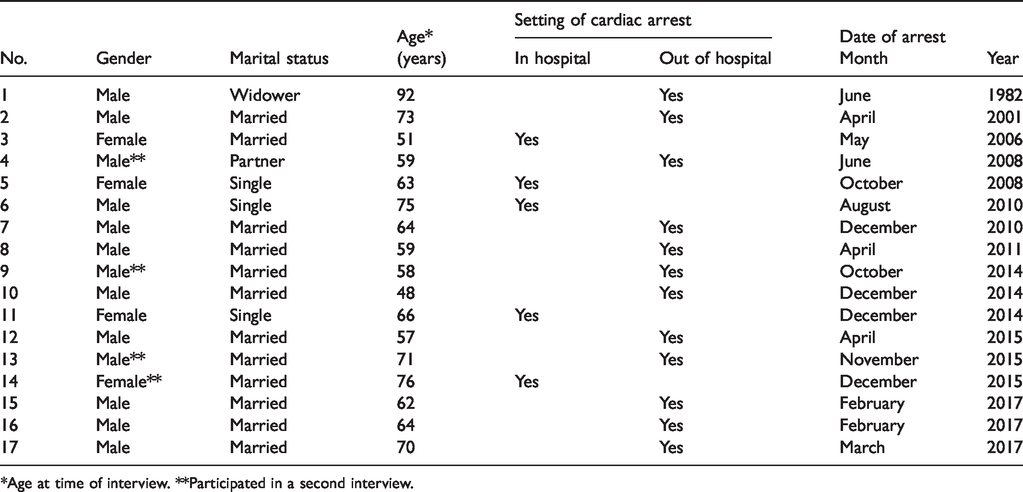
*Age at time of interview. **Participated in a second interview.
Data collection
The first author, who has experience in intensive care and education, conducted the individual interviews during November 2016 and June 2017. The duration of first interviews ranged between 52 minutes and 3 hours 49 minutes with a median time of 73 minutes. Second interviews ranged from 44 to 63 minutes. These interviews were held at a time and place chosen by the participants: fourteen were face to face and three on video chat using Skype (Skype Communications). All interviews were audiotaped with participant permission and field notes were completed after the interview. The first author transcribed all interviews verbatim. Questions such as ‘Tell me about coming home?’ and ‘What was the biggest difference in “before” and “after” the CA in returning home?’ kept the conversation focused. Before and after the main interview contact was maintained via email and phone calls, consistent with the relational aspects of NI. 14 , 15 Participants were offered a second interview, however, they were advised that there was no obligation to take part in this. Four participants took part in a second interview, providing them with the opportunity to add information included in the inquiry, and a chance to extend the researcher–participant relationship as recommended by Clandinin and Connelly. 14 Transcribed material was returned to the participants for review before analysis commenced. Due to the large amount of field text, data obtained from the interviews were divided into three sections: The immediate time before and after the CA, Transition from hospital to home, and Long-term survival. Each section has been analysed and presented separately. This analysis focuses on the transition from hospital to home and findings are presented below.
Data analysis
The analysis of collected narratives using Clandinin and Connelly’s 14 three-dimensional framework of time, sociality and place, was central in identifying the narrative threads and answering the research question of the survivors’ experiences of returning home after surviving CA. Participants were assigned pseudonyms to maintain confidentiality. Language used and highlighted words were closely checked to determine their fit with potential threads. 22 In line with the dimension of sociality and its personal conditions, participants’ statements about their feelings and their hopes for the future were examined carefully. The first author observed the body language and other non-verbal communication of the participants during the interview to enhance the interpretation of the narratives and noted these in a journal. The transcribed stories were read, re-read and listened to multiple times and field notes were included to create a narrative of the experience for each participant. Analysis was a prolonged iterative process where the three dimensions were central in identifying emerging threads. 15 Before meetings with co-authors, transcribed interviews and emerging threads were circulated among the authors checking that the threads stemmed from the transcribed material. In NI, findings are fluid and experiences change over time, therefore ‘final research texts do not have final answers’. 15 (p.51) The findings are intended to engage the reader ‘to rethink and reimagine the ways in which they practice and the way they relate to others’. 15 (p.51)
Ethical considerations
This inquiry conforms to the principles outlined in the Declaration of Helsinki 23 and before recruitment of participants, ethical approval was received from the authors’ university human research ethics committee (reference number: H-2015-0132). Given the potentially sensitive nature of the inquiry, the interviewer was alert to any signs of distress from participants during the interviews. Written consent was obtained from participants and no reimbursement for time was offered. The researchers did not know any of the participants prior to the interviews and no participant withdrew from the inquiry during or after the interviews.
Findings
Five threads emerged from the data analysis: A new reality in coming home, Emotional turmoil, Restrictions both internal and external, Navigating medication regimens and Support systems. The three dimensions were closely intertwined 14 , 15 and central in identifying the narrative threads. For the dimension of time survivors recalled the past, before the CA and what was a known reality, and then faced the time of coming home, a transition to a new reality and an unknown future. The social transition from being, what many of the participants considered a healthy person, to a CA survivor with prolonged health concerns was mentally challenging. Questions of future employment and health were central, with the threads emerging from the sociality dimension. The final dimension, place, highlighted the change from hospital to home and was a stark reminder that their reality had changed. What they used to be able to do at home with ease was now a tiresome task.
The presentation of findings related to each thread uses quotations from the participants, creating an ongoing narrative starting with the transition from the hospital to home. The number within the brackets immediately following a participant’s quotation represents the participant number listed in Table 1.
A new reality in coming home
To leave the hospital routine and return home after a CA was often daunting. The external aspects of independence, work and participation in society were now apparent. There was a realisation that they were different from before the CA. The following quotations reflect the difficulty of and adjustments to a changed life. Participants reflected on the sociality dimension of inquiry with a specific focus on personal conditions involving feelings and emotions. You have your CA and all that hospital stuff — and you think, that is it. I have survived all of that. The hardest part is afterwards, to come home. (12) It was difficult to come home. (5) Wondering what does this mean for me in terms of my future and how my life might be compromised. (3) I was out of hospital, but I was still slow mentally and physically. (9) I had to re-evaluate a lot of things, including work. (4) I used to run a community centre for 25 years and within four weeks I went from actively working to nothing. (10)
Emotional turmoil
As the survivors came to terms with the reality of surviving a CA, it became an emotional roller coaster. There was a joy of survival. I am amazed I survived. (5) A happy ending is a good cure for trauma. (2) Some nights you lay there thinking about it – listening to your heart beat. It is just fear. (10) I was in a spiral of more anxiety. (13) To have a CA is to be very close to death – it is not that easy just to get over it, or told it will be alright. (16) I know this is a life event and people go through it. (2) The biggest obstacle is not knowing what might happen next. (6) I thought your heart broke, you get something fixed and everything is right again. (9) I don’t like the concept of being defined by an illness and the sick role. (4), I want to get to the end of this, I want to get back to normal! (17)
Once home, during the early recovery period, participants described a vulnerability in their encounters with the healthcare system where the many medical appointments participants attended reminded them of their ordeal. I was so sick, I would be in hospital every three or four days. (10) I sat there waiting and said ‘if I die here is that all right?’ They replied ‘Don’t die here – too many forms to fill out!’ (12) I live rural, it was an issue! Because the cardiac support was in town. (5) After the CA I remember no one had the answers, which meant I felt this could happen again. (4) I was trying to read everything I possibly could. (8) They gave me a pack of brochures – read this, do this. (11)
A recurring thread in the survivors’ narratives was the importance of fitness for their survival and their surprise that they had actually had a CA. I have been healthy my whole life, I thought that would be enough to keep me on the safe side. (7) I do not think you find many individuals more health conscious than me, more pedantic about health and diets, to the point to having blood tests done every six months, so for this to happen to me it was a surprise, I was quite angry for a while. (10) I had a fit body, I was returning to normal. Look after your body! (1)
Restrictions both internal and external
Participants realised that their lives were not the same as before their CA, their bodies had new limitations. I felt completely entrapped in illness within myself. (4) I got back to my job, but I could not handle it. (9) I was chomping at the bit to do things. That was the hardest thing. (14) I was out of hospital but I was still slow mentally and physically. (9) I never felt old before the CA. (17) At the moment I am sort of half treating myself as an invalid. (13)
A leading restriction coming home was the driving ban, causing the participants to depend on others. The worst – I was not allowed to drive! To me driving is essential! If I can’t drive, who am I then, I’m no help to anybody. (9) I thought the ban was excessive, I couldn’t get around. (4) It just hurts – I cannot just duck into town and do something. (6) It was difficult to all of a sudden to have to rely on other people, especially with the driving. (10)
Navigating medication regimens
For many of the participants there was a drastic change from no, or few, medications, to multiple medicines. I came from having hardly any medication to having a plethora of bloody pills. (12) I never took a tablet before, I am 70 years old! It is bloody terrible. I went from sublime to ridiculous – a massive lifestyle change. (17) I was on no heart medication. Now I am probably on more medication than most people. (2) I was out and I had forgotten my tablets so I turnaround. (10) Maybe it is fear – I will not miss a dose of my medication. If I can do something to promote a longer life, I can do all the soul-searching, but if I don’t follow the strict medication regimen, all of the other things are pointless to some extent. (4) My GP told me I would be on aspirin for the rest of my life. I stopped probably after nine months. I take no tablets! (7) I wrote down every time I had a painkiller. I knew they could be dangerous so I stopped taking them, but I kept them, if I don’t feel good I can take them. (13)
Support systems
To adjust and navigate their way through the health system was, for many, a stressful experience and there was often a disjointed relationships between survivors and support services after the event. A lot of frustration was battling the health system. I am spending a good part of my life sitting in the waiting room, waiting for something to happen and I get frustrated. (17) Nothing was smooth, you become involved in a health fight. I just had this major CA and they say ‘Two weeks from “someday” we have an appointment’. (16) I was lucky, I knew the system – I have been helping others through the system. (12)
Part of the support system offered to survivors following CA was rehabilitation sessions. There were mixed feelings over the benefits of attending cardiac rehabilitation (CR). I went to rehab. I tried to be a good patient and do all the things I was supposed to do. (2) It was only exercises. They lecture you! Very similar in what they did on the ward. (5) There is a group at community health. It was supportive. (8) They wanted me to go to rehab. I did not see myself needing it, I felt fit and healthy. (7)
Discussion
To survive a CA is an unexpected experience and the consequences for the individual and society are huge. 2 This inquiry explored how survivors experienced the transition from hospital to home and how they settled into their new roles as CA survivors. Using Clandinin and Connelly’s 14 three-dimensional NI framework of time, sociality and place, this study explored the narratives of four female and 13 male CA survivors about their experiences of leaving hospital and returning home. The main findings highlight the disruption of participants’ lives and how the return home made the changes palpable both mentally and physically.
The participants expressed a positive attitude towards their survival, although they viewed the transition from hospital to home as uncoordinated. Our findings indicate that nurses and health professionals need to have a broad knowledge of support services available for the survivor, and the ability to guide the patient to engage with the most relevant services. The geographic location of their home was an important factor in the level of support available, as those in rural areas expressed frustration that living in a rural area meant support was limited. This is not only a rural dilemma; available support for CA survivors varies among health services and often there are limits to follow-up treatment after a CA. 24
Although there was support for CA survivors as they returned home, long waiting periods and miscommunication between different support services created a feeling of frustration, possibly creating emotional barriers to the willingness to implement changes in practice as part of a daily routine. There was a perceived lack of information, which could be magnified by the survivors’ state of recovery, as memory is often affected after a CA. 24 – 26 Information needs to be provided in such a manner that the survivor can comprehend the information and may need to be repeated or provided in writing. The survivor’s response should guide the information provided so that the content is adjusted to the individual’s requirements. 27
The restrictions that survivors experience, both internal and external, highlighted the enormity of the event. The CA survivor had to adapt to a different lifestyle and the uncertainty of physical limits created insecurity. Not to be able to carry out common everyday activities at the same level as before was a new experience; this is also described by Swedish research. 25 , 28 Driving restrictions, especially for men, were a limitation causing frustration among survivors as they became dependent on others for transport – the loss of independence was mentally distressing and difficult to accept. Nurses and health professionals need to take into account that the male stereotype of independence, strength and as a provider may influence how male CA survivors perceive the care given. 5 , 28 The new increased medication regimen was a daily tangible reminder of the CA and of a failing body; it could be burdensome for respondents to accept that they now had a chronic illness. This was more prominent among male survivors and might also be influenced by the male stereotype. 5 Often the CA survivor felt that health professionals did not understand the enormity of surviving a CA for the individual, there was a perceived lack of empathy and understanding from health professionals. Survivors felt dismissed, this was not only described by participants in this study but is a common theme in qualitative research exploring CA survivors’ experiences. 4 , 24 , 28 – 30
Mostly research about CA focuses on the actual event 31 and less is known about how best to provide care for survivors. Acknowledging the internal and external difficulties experienced by the CA survivor and providing essential services to meet these needs will allow them to return to an optimal level of activity. Cardiac rehabilitation (CR) encompasses all cardiac conditions including acute myocardial infarction and acute coronary syndromes. There is limited research focusing solely on rehabilitation for CA survivors. However, with similarities in recovery, the benefits of CR are transferable to CA survivors.
Individuals’ perceptions of health levels influence participation in CR as seen in participants’ conversation fragments. Opinion about the importance of participation in rehabilitation was divided, as some participants did not find it to be an important part of their recovery. Factors such as physical, logistical (for example, driving bans), and health system factors influence participation in CR. 27 There is a need to personalise information to CA survivors as those who did participate in CR expressed that the sessions were not aimed at their level of recovery. Increased knowledge of the benefits of CR and support from health professionals to coordinate strategies to achieve efficient care and follow-up for CA survivors should increase CR participation. 32 , 33
Holistic care is important in the recovery after a CA and has positive outcomes for the individual. 7 , 30 Holistic care involves the whole person, their physical, emotional, social, economic, and spiritual needs, 34 and is inclusive with a focus on the interaction between health services and the patient. 35 Often, nurses are the health professionals that communicate most frequently with patients and have a coordinating role in planning care. As such nurses need to be familiar with other health professionals’ different roles. 35 Research indicates that individuals who received holistic care had an increased physical activity level, returned to work to a greater extent and reported a higher QOL. 36 A holistic care approach improves the partnership between nurses, other health professionals and their patients, which leads to an improved patient experience of care.
Empowering the CA survivor enables them to take a larger part in the decision-making process. 33 For the individual experiencing a CA it is a life-changing event. 24 , 28 , 37 Learning from CA survivors’ narratives, an understanding of CA survivors’ experiences of returning home should influence the holistic care needed to improve the transition from hospital to home. 38 , 39 Often the full extent and reality of the CA is not obvious for the survivor until they have returned home. Participants’ home routines were altered, and the experience of coming home was a daily reminder that their life had changed. The realisation that their heart had failed, and their body was no longer functioning as usual, created feelings of insecurity and fear. While health professionals often place emphasis on medical knowledge, the person’s feelings about their changed body need to be central to provide holistic care. 40 , 41 Leaving hospital, some participants worried that they might experience another CA, creating insecurity and although they might have lived alone before the CA, they now had family or friends living with them. This feeling of insecurity during the transition to home is common 4 , 25 , 28 and must be considered when care is planned. There is evidence that lifestyle changes and medication adherence are important in CA survivors’ recovery, and the support provided in CR increases the likelihood of both lifestyle changes and medication adherence. 25 , 42 Therefore, recovery plans after a CA should include an automatic referral process to CR and a plan that clearly emphasises the benefits of participation to the survivor.
Strengths and limitations
There are limited findings exclusively from CA survivors’ rehabilitation experiences, and often research includes all cardiac ailments such as myocardial infarction (MI) and acute coronary syndromes. In an article comparing QOL between CA and MI there was no difference between the two groups, 43 suggesting the generalisation of findings among cardiac conditions. Participants in this inquiry included both genders across a wide age span, with broad education levels, working experience and living conditions, providing validity and reliability of the data. 44 This inquiry’s rigour, trustworthiness and validity is founded on the reflexivity of the researchers’ open approach and thoughtfulness towards the participants’ narratives, supported by Clandinin’s 16 and Clandinin and Connelly’s 15 framework. Further to reflexivity, a reflective journal was kept throughout the research process by the first author to prevent unintended pre-conceptions and conclusions. 44 To uphold rigour and ensure credibility and dependability, meetings with participants were held over a prolonged time and included emails and phone calls to support accuracy in the study. 16 , 44
Although participants with a less favourable view of their survival were eligible to participate, only participants who regarded their survival with a positive outcome contributed. Survivors with less favourable experiences may have told a different story. Participants selected what they were willing to share in the conversation with the researcher and may have adjusted their stories to include only what they perceived as important. The generalisability of these results is limited as the participants in this study lived in a society with a high level of technological hospital care. CA survivors living in a society with reduced access to care might have other social and cultural narratives not found in this study.
Clinical implications
Nurses and health professionals need to consider the enormity of surviving a CA as it has broad consequences for the individual. Survivors may need extra encouragement and support in the transition home when confidence over their ability to participate in society might be low. Both clinical and logistical needs must be taken into account to provide opportunities for participation in suitable activities. Interdisciplinary holistic care may support survivors to cope with the transition to home, increase survivors’ QOL and improve health outcomes. The perceived lack of support from health professionals during the survivors’ transition to home life could be resolved through transition programmes in hospitals, where dedicated nurses and health professionals follow the CA survivor during the transition from hospital to home. 4 , 33 , 35
Conclusion
Returning home after surviving a CA is an emotional roller coaster experience, where survivors have to accept that their bodies may not be as capable and dependable as before. The realisation that their bodies had unexpectedly failed them made them anxious when they returned home, indicating a need for support from health professionals, including information addressing their concerns and available support services. The transition home was a stark reminder of their new reality where they could not perform at the same level as they previously did, questioning their sense of being. Nursing interventions and support need to address the time of transition home and nurses need to emphasise the importance and benefits of participation in CR. Returning home may be a chaotic and bewildering time; however, nurses and health professionals can learn from survivors’ stories and play an important part in optimising the transition back to a new normal life by providing holistic care.
Supplemental Material
sj-pdf-1-njn-10.1177_2057158520932348 - Supplemental material for The experience of returning home after surviving cardiac arrest: A narrative inquiry
Supplemental material, sj-pdf-1-njn-10.1177_2057158520932348 for The experience of returning home after surviving cardiac arrest: A narrative inquiry by Gunilla Haydon, Pamela van der Riet and Kerry Inder in Nordic Journal of Nursing Research
Footnotes
Acknowledgments
The authors are grateful to all the participants for their willingness to share their experiences and participate in this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.
Supplemental material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.