
Abstract
The aim of this study was to describe nurses’ opinions regarding assessments of oxygen requirements and which modes of cognition they used about oxygen treatment in ventilated children aged 0–3 years. The method was survey design with descriptive statistics. The sample included 90 nurses from intensive care units within all university hospitals in Norway. The questionnaire covered use of physiological, clinical, and technical observations in assessments, and the Nursing Decision-Making Instrument was used to map the mode of cognition. Respondents perceived they used many of the physiological criteria except for the haemoglobin–oxygen dissociation curve, pulse and blood pressure. Most respondents used clinical and technical criteria to assess oxygen needs, but more than half would exceed 10% oxygen at each regulation. They considered written guidelines to be necessary. A majority demonstrated a flexible use of analytical and intuitive modes of cognition in the decision-making processes. The results indicate that assessment of children’s need for oxygen may be based on insufficient information, and written guidelines should be developed.
Keywords
Introduction
In hospitals, supplemental oxygen is one of the most common treatments administered to paediatric in-patients.1–3 Oxygen is a necessity for aerobic cellular function in the organism, 4 and it is administered to correct or prevent hypoxia.5,6 Associations between hypoxia and poor outcomes are well known. 7 However, oxygen is considered a potent and potentially toxic drug. 8 Hyperoxia, meaning too much oxygen in arterial blood, can be harmful1,9 because hyperoxia is associated with cellular damage. 10 Thus, nurses need to be aware that excessive use of oxygen is the only cause of hyperoxia among critically ill infants. 11
Oxygen should be added according to the patient’s need, but it is not always administered appropriately in practice. 12 The understanding that too much oxygen could be harmful to premature infants dates back over 60 years, but the knowledge that even brief exposure to oxygen causes damage to full-term newborns is also well established. 9 There have been several studies regarding oxygen treatment in premature children, 13 but there is a lack of evidence regarding how to optimize oxygenation in ventilated full-term newborns. 14 Oxygen treatment is often given to acutely ill medical patients because of insufficient collaboration and discussion between doctors and nurses. 15 Physicians have the legal responsibility in patient care, including oxygen treatment, 13 but nurses are still responsible for titrating oxygen within the prescribed limits of peripheral oxygen targets.16,17 It is recommended to administer oxygen with caution. Titrations of oxygen concentration by 5–10% when adding or 2–5% when decreasing at each regulation are suggested; 18 when exceeding 10%, the child is exposed to the risk of hyperoxia. 19 To ensure the quality of oxygen treatment, consensus and established criteria are necessary,20,21 but there is no evidence to guide the administration of oxygen to full-term newborns. 3 A shortage of research literature to guide nurses in the assessment of oxygen treatment in critically ill children aged 0–3 years is a reality as well. 22
Hyperoxia and its consequences
Hyperoxia is defined as arterial pressure of oxygen (PaO2) above 10.7 kPa in full-term newborns 23 and above 13.3 kPa in children in general.24,25 Hyperoxia is caused by high levels of the fraction of inspired oxygen (FiO2), which results in oxygen toxicity. 26 If oxygen is added without the knowledge that peripheral capillary oxygen saturation above 95% may lead to high PaO2 levels, the child could potentially be exposed to danger. 27 Regarding consumption, oxygen is released loosely or transported bound to haemoglobin, and each haemoglobin molecule can bind four oxygen molecules. If all haemoglobin molecules have bound four oxygen molecules, the blood will be saturated with 100% oxygen. 28 Thus, hyperoxia leads to the accumulation of free oxygen radicals as a result of more oxygen molecules being added than each haemoglobin molecule can carry. 29
Hyperoxia increases the risk of absorption atelectasis,6,26 pulmonary oedema and acute respiratory distress syndrome in general. 10 In addition, hyperoxia may lead to cardiovascular responses such as decreased heart rate accompanied by a parallel decrease in cardiac output, systemic vascular resistance and increased blood pressure. 10 Hyperoxia can also result in oxidative stress associated with both tissue damage and DNA damage, and cell death is a prominent feature of hyperoxia-induced lung injury.30–32 The cause of these types of significant cellular damage is reactive oxygen species reacting with molecular components, such as lipids, DNA and proteins. 10 Hyperoxia is also associated with increased mortality in critically ill adults 7 as well as in medical patients in hospital in general. 15 The mentioned factors and the harmful consequences of too much oxygen underscore the complexity and importance of correct oxygen administration.
The complexity of assessment when administering oxygen treatment
There are variations in the criteria for assessing oxygenation. 21 Oxygenation is characterized by the availability of oxygen to meet the metabolic demands of tissues, which include oxygen transport in the blood and oxygen delivery to the tissue. 33 There are several criteria for measurements described in professional and research literature that should be assessed when the child’s oxygenation is judged by nurses. First, nurses need to assess physiological criteria, such as the PaO2, pH and arterial pressure of carbon dioxide (PaCO2) measured in blood gases, and the child’s temperature, pulse, blood pressure and haemoglobin count. 16 To correctly assess oxygenation, an understanding of the haemoglobin–oxygen dissociation curve (Hb–O2 curve) is required. 30 As the Hb–O2 curve reflects haemoglobin’s affinity for oxygen, haemoglobin will bind oxygen more strongly if the PaO2 is low, resulting in less oxygen being released to the tissue. 16 Furthermore, nurses need to be aware that changes in the physical positions of the child during treatment could make a difference in the oxygenation status, as children have less surface for gas exchange than adults. 34 Children also have a smaller functional residual capacity and higher oxygen consumption, 10 but oxygen delivery to the tissue does not differ between newborns and adults. 8 Second, clinical aspects and the patient’s condition are criteria that need to be assessed, as these factors may have an impact on oxygenation. 35 Such clinical observations include the colour of the child’s skin, the increment of the thorax, auscultation, and the child’s satisfaction and interactions with the ventilator.16,18 The third condition that needs to be assessed is technical settings affecting oxygenation during mechanical ventilation. Appropriate oxygenation in ventilated children could be achieved by titrating FiO2 and regulating the mean airway pressure (MAP). 36 In addition, assessing tidal volume (TV) continually is essential because TV indicates how much air enters and exits the lungs with each respiratory cycle. 37 Thus, nurses must assess whether the FiO2 or ventilator settings should be regulated to optimize the child’s oxygenation status. For example, the peak inspiratory pressure (PIP), positive end-expiratory pressure (PEEP) or inspiratory time can be used to regulate MAP, 13 and changing PEEP is an effective way to improve oxygenation. 36 The use of large TV and high airway pressure can also improve oxygenation considerably in acute situations. 38 In addition, advantages and disadvantages associated with ventilator settings should be assessed. In patients with severe lung failure, where treatment lasts for days and weeks, it is recommended to choose combinations of TV, airway pressure and FiO2 that ensure appropriate oxygenation while keeping the risk of harmful effects as low as possible. 38
Peripheral capillary oxygen saturation targets
In order to achieve an adequate oxygen treatment practice, a peripheral capillary oxygen saturation (SpO2) range of 90–94% is suggested for most patients, and a range of 88–92% is suggested for patients at risk of hypercapnic respiratory failure. 15 The British National Formulary for Children recommends that SpO2 be maintained at above 92% for most critically ill children, but it is emphasized that some clinicians may aim for a target of 94–98%. 39 In addition, SpO2 of ≤ 96% is a strong recommendation for patients receiving oxygen treatment in general. 15 It is argued that guidelines can improve the maintenance of SpO2 targets. 11
Theoretical perspective
This study was guided by Kenneth R. Hammond’s cognitive continuum theory (CCT), as the questionnaire is partly based on the CCT. According to his dynamic cognition theory, individuals move along the continuum over time or oscillate between various modes of cognitive processes.
40
On the cognitive continuum, judgements exist at a point between two opposite poles: analysis and intuition. Modes that combine the analytical and intuitive modes have been defined as being quasirationally or flexibly orientated modes of cognition. Flexible modes may be more or less analytically or intuitively orientated; therefore, these modes are a matter of different degrees of analytical and intuitive modes of cognition.
40
The nature of the task, the time available and the complexity of the task will influence the assessment. In the CCT model, a well-structured task, more time and systematic assessment characterize an analytical mode during decision-making, whereas the opposite would characterize an intuitive mode of cognition.
40
Research indicates that CCT has the potential to make major contributions towards understanding decision-making processes in clinical nursing.
41
The theory allows researchers to describe and explain judgemental behaviours, and it provides knowledge about the relationship between task properties and cognition.
42
Findings from an international study that measured decision-making in different nursing fields among 1460 nurses revealed that the majority of the nurses had a flexibly orientated mode of cognition.
43
Nurses’ mode of cognition is essential in assessments of oxygen treatment because a high degree of analytical thinking includes all criteria that indicate a good assessment. The aim of this study was therefore to describe nurses’ opinions regarding assessments of oxygen requirements and which modes of cognition they used for administering oxygen treatment in ventilated children aged 0–3 years. The research questions were as follows:
1. What do nurses report about assessing oxygen treatment in children? 2. Which physiological, clinical and technical criteria do nurses report using when assessing a child’s oxygenation? 3. What degree of cognition is most prominent when nurses assess a child’s need for oxygen treatment?
Methods
Design
This was a cross-sectional study with a descriptive design. A convenience sample of nurses was recruited from intensive care units (ICUs) in Norwegian university hospitals. In Norway, there are three paediatric ICUs and three general ICUs where children are treated occasionally. Respondents from all of these hospitals are represented.
Sampling
The selection criteria for inclusion in the study were that participants were registered nurses, were employed in at least a half-time clinical position and had experience with ventilated children. Nurses from Western, Eastern, Southern, Central and Northern Norway are represented. Approval was granted by the Norwegian Centre for Research Data and the hospitals’ local ethical committees. Written information about the study was distributed to clinical department heads, nurse managers, other relevant contacts and potential participants. We regarded the returning of the completed paper-and-pencil questionnaire as implying consent to participate. The procedure for distributing the questionnaire was slightly different from unit to unit out of practical consideration for the contacts. The form was distributed either via the staff room or post boxes, or was given directly to potential respondents. The collection procedure was completed in a congruent way, as completed questionnaires were collected in closed boxes at all units.
Measures
The questionnaire consisted of three parts. Part A comprised questions about demographic data, information about years of experience, specialist competence and whether or not the unit had written guidelines regarding oxygen treatment. In addition, six items covered questions about administering supplemental oxygen in clinical situations; for instance, whether time use was important since oxygen should be titrated with caution, and what percentage of FiO2 should be added at each regulation when administering oxygen.
Part B consisted of the Nursing Decision-Making Instrument (NDMI) questionnaire. The NDMI was chosen because it has been tested for reliability and validity.43–45 It has a total of 24 items, including six items related to four stages of the decision-making process: 1) data collection, 2) data processing and identification of problems, 3) plans of action and 4) implementation of the plan and evaluation. Respondents answered each item in Parts B and C on a five-point Likert-type scale with the following endpoints: 1) almost never and 5) almost always.43,46 In line with the developers’ instructions, the NDMI scores were added up, and the sum total was interpreted as follows: 1) under 67 points, decision-making was analytically orientated; 2) between 68 and 78 points, decision-making was flexibly orientated; and 3) above 79 points, decision-making was intuitively orientated. In order to measure the sum total score, all items had to be answered. 46
The questionnaire in Part C consisted of 17 items that measured physiological, clinical and technical criteria that are essential to observe in oxygen assessment. For example, Part C assessed the use of physiological aspects, such as SpO2, PaO2, pH and PaCO2 levels, the Hb–O2 curve, and the child’s temperature, pulse, blood pressure and haemoglobin count when in need of oxygen supply. Clinical conditions, such as skin colour, increment of the thorax, auscultation, the child’s satisfaction and interactions with the ventilator were also measured. In the end, we asked how often observations within technical settings affecting oxygenation during mechanical ventilation – PIP, PEEP and TV – were included in the assessments.16,18
Parts A and C of the questionnaire were developed and used with the NDMI in a study of premature infants in Norway, 18 and were then adjusted to the age group in this study.
Analyses
The data were first entered into the statistics program SPSS version 23, and data from every fifth respondent were double-checked. Data are presented using descriptive statistics. Continuous variables (such as age) are described with mean, median and standard deviation (SD) when normally distributed, or with median and range for data with skewed distributions (such as years of experience). Categorical data are presented as proportions and percentages in the text, frequency table and figure. Cronbach’s α was performed on data to assess the internal consistency of the NDMI.
Results
A total of 90 nurses participated in the study. Demographic data showed that 92% (n = 83) were specialist nurses in intensive, paediatric or newborn care, including 80% (n = 72) being in intensive care. The nurses’ mean age was 45 years (SD = 9.27), with a range of 29–65 years. The range in experience was 0–36 years (median = 12, SD = 8.78) for specialist nurses and 6–41 years (median = 19, SD = 8.92) for nurses in general. In addition, experience with ventilated children ranged from 0–33 years (median = 8, SD = 8.77).
Assessments regarding oxygen administration
Considering the question about what percentage of oxygen the respondents would have added at each regulation after desaturation related to patient care, 77% of the respondents (n = 69) reported that they would not give more than 30% oxygen at each regulation, including 44% (n = 40) who would not have exceeded 10%. However, 9% (n = 8) indicated that they would add 100% oxygen after desaturation, and 6% (n = 5) wrote comments on the form instead of responding to a specific choice. These respondents stated that the administration of oxygen was based on individual differences and variations from child to child, depending on continuous oxygen concentration, the child’s condition and how the situation was affected: illness/emergency versus stable situation. Some of the other respondents who responded to a specific choice also wrote that individual inequalities, the state of the illness and what percentage of FiO2 was added at each regulation after desaturation were situation-based. In addition, 51% (n = 46) and 38% (n = 34) respectively stated that it was ‘important’ and ‘very important’ to use time when administering supplemental oxygen. Written guidelines for the administration of oxygen treatment were considered necessary by 73% (n = 66). With regard to guidelines, 46% (n = 41) of the respondents reported that their unit did not have guidelines, and 40% (n = 36) stated that they were unsure whether or not their unit had guidelines.
Use of criteria when assessing oxygenation
Nurses’ use of criteria when assessing oxygenation (N = 90).
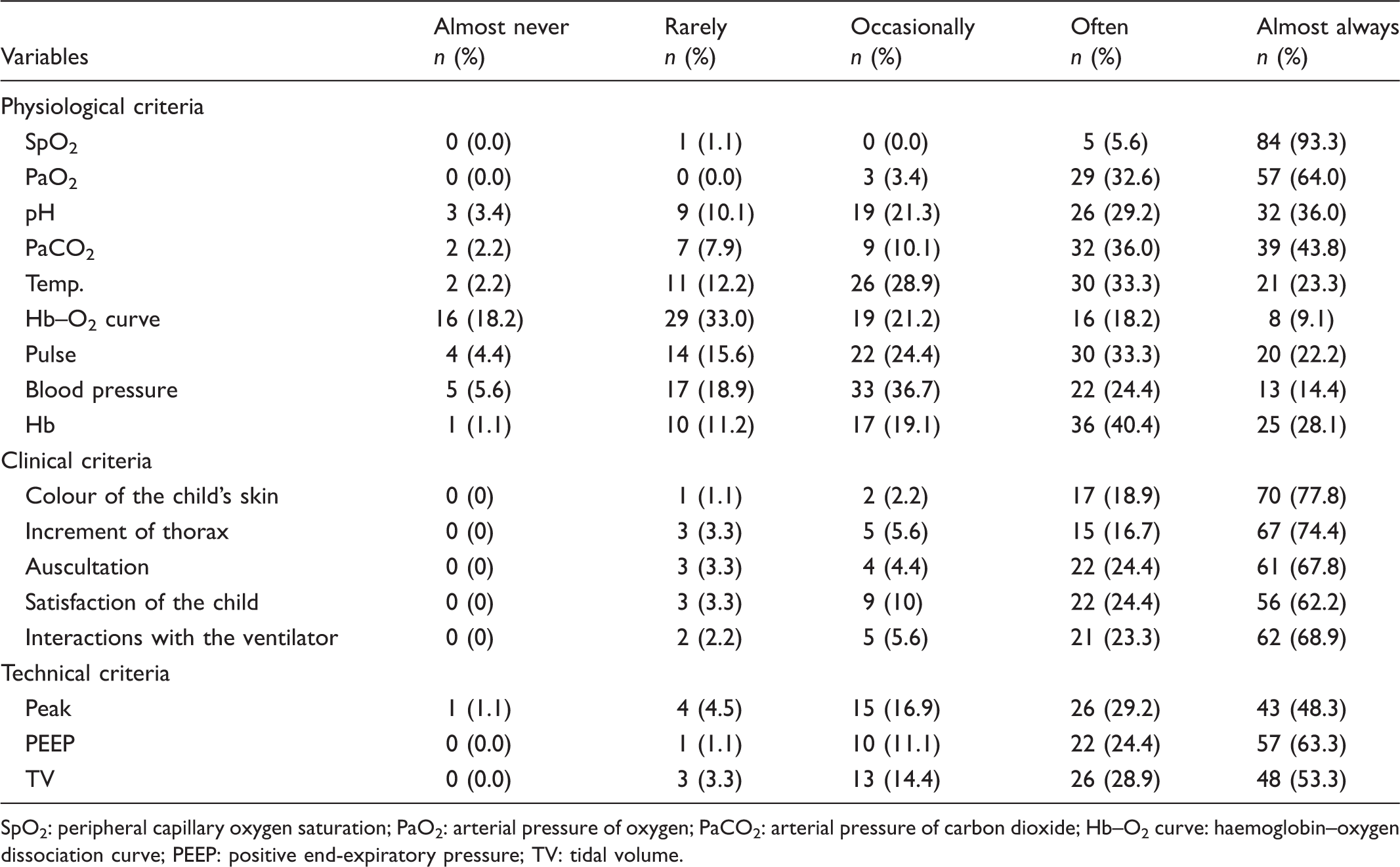
SpO2: peripheral capillary oxygen saturation; PaO2: arterial pressure of oxygen; PaCO2: arterial pressure of carbon dioxide; Hb–O2 curve: haemoglobin–oxygen dissociation curve; PEEP: positive end-expiratory pressure; TV: tidal volume.
Cognitive decision-making processes and assessments of the need for oxygen treatment
Seventy-six of the 90 respondents (incomplete forms = 14) reported cognitive decision-making processes when assessing the need for oxygen treatment for children. According to the NDMI instructions, the sum total score could not be measured if not all items had been answered. There were between one and five missing items in the incomplete forms. Approximately one-third of respondents were in the ‘intuitively orientated’ mode of cognition category, and very few nurses were in the ‘analytically orientated’ mode of cognition category (Figure 1).
Nurses’ degree of cognitive modes during decision-making of need for oxygen treatment.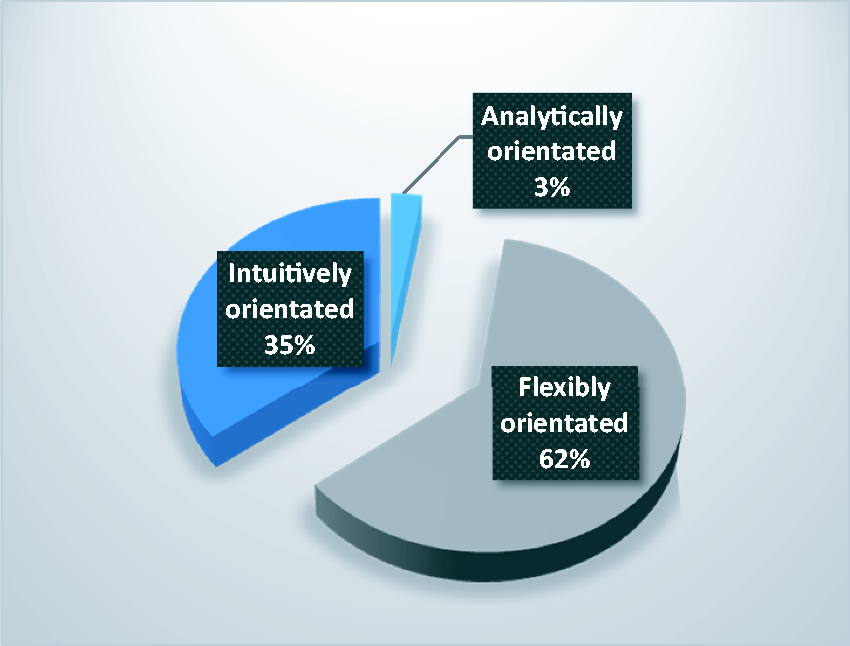
Discussion
Our major finding shows that the majority of the respondents reported using several of the selected physiological, clinical and technical criteria in their assessments of oxygenation. However, there is potential for improvement, as some assessments of oxygenation were based on insufficient information. Some of the respondents lacked important criteria for performing the assessments at a sufficiently high cognitive level when assessing the need for oxygen for critically ill children.
Administering supplemental oxygen, and the need for guidelines
More than half of the respondents would have exceeded 10% FiO2 at each regulation after desaturation. Interpreting the written comments in the filled-in forms, we identified some uncertainty regarding what percentage of FiO2 should be added at each regulation. Some of the respondents drew attention to the complexity of oxygen administration tasks, including aspects that influence the assessment, such as individual inequalities or situation- and disease-related conditions. Results from the present study reveal that the majority of the respondents emphasized using time when FiO2 was regulated; in contrast, 9% reported that they added 100% FiO2 after desaturation, which may indicate that these nurses did not use time when administering oxygen. In clinical practice, there have been statements arguing that the over-use of oxygen is primarily a concern regarding premature infants. Both uncritical use of supplemental oxygen and limited knowledge regarding hyperoxia have been observed as well. 22 For older infants, there is indeed a stronger focus on avoiding hypoxia than hyperoxia, 3 but the over-use of oxygen can be harmful as well.1,9,12 Although hyperoxic children seem to have a higher crude mortality rate, there is a lack of evidence regarding the increased mortality of critically ill children. 7 The uncertainty regarding oxygen administration can probably be explained by the fear of under-using oxygen. A cohort study and systematic review of the relationship between the PaO2 at intensive care admission and mortality in critically ill children concluded that hypoxia was associated with increased mortality in children younger than 18 years of age. 7 Additionally, patients who are already critically ill are exposed to the risk of organ damage from hypoxia. 12 Identifying the need for oxygen and how much is needed to achieve the desired SpO2 target is considered good oxygen management, 12 but nurses should not withhold oxygen treatment for fear of oxygen-associated complications. 6
A total of 73% of the respondents considered written guidelines a necessity, but 40% were still unsure whether or not their unit had guidelines. This finding can be compared to a Norwegian study on nurses in neonatal ICUs that had 111 respondents, two-thirds of whom did not know whether their unit had guidelines for oxygen treatment. 16 In our study, there were more specialist nurses (92%) than in the study on neonatal ICUs (72%), which was conducted ten years ago. 18 Despite these differences, the result raises the question of why specialist nurses working in ICUs were unsure whether their units had guidelines. It is suggested that nurses should adapt an evidence-based nursing practice, 47 and evidence-based practice is a requirement in Norwegian heathcare in general. 48 By making use of guidelines, knowledge-based practice can be carried out because the nurses can rely on the available professional knowledge and research literature. However, there is a lack of evidence to guide nurses in the administration of oxygen treatment in critically ill children. 22 Although guidelines themselves do not ensure quality in patient care, clear guidelines for oxygen treatment can be supportive when performing qualified assessments for individual patients. 20 Guidelines contribute to consistent, evidence-based nursing practices as well as safe patient care, 12 and standardization can help with avoiding variations between different institutions. 6 Such guidelines may also result in establishing consensus regarding the administration of oxygen treatment in critically ill children. 21
Assessing oxygenation based on the use of criteria
The majority of the respondents reported using the selected criteria in their assessments of oxygenation, but some of the nurses did not include pulse (44%) or blood pressure (61%) when assessing the child’s oxygenation status. To compare, 30% did not include the infant’s pulse and 41% did not include the infant’s blood pressure when assessing oxygenation in the neonatal study. 16 This calls into question whether the nurses understood the importance of assessing the blood’s capacity to deliver oxygen to organs and peripheral tissue. In addition, our study shows that the assessments of oxygenation were based on insufficient information, as the use of the Hb–O2 curve was not included. Preferences in oxygenation assessment among neonatal staff members revealed variations within and between units in the Netherlands as well. 21 Findings from the Dutch study indicated that it was quite accidental which criteria were used when assessing oxygenation, and our results also show that respondents did not use all physiological criteria in their assessments. Nevertheless, both the complexity and all criteria should be considered when nurses make oxygenation assessments. For instance, an understanding of the Hb–O2 curve and the relationship between the PaO2 and SpO2 is essential when assessing oxygenation. 30 If the child has satisfactory SpO2 and PaO2 levels, but low haemoglobin count and/or blood pressure, the child can be at risk of hypoxia if these criteria are not included in the nurse’s assessment. 16 High PaCO2 levels, acidosis and elevated temperature can also have an impact on the Hb–O2 curve, which results in oxygen being released more readily to the tissue. Consequently, when nurses notice normal SpO2 levels in these conditions, they risk ignoring excessively high PaO2 levels. 16
Cognitive processes in clinical decision-making when assessing oxygen treatment
The present study indicates that one-third of the respondents had an intuitively orientated degree of cognition related to decision-making when the child’s need for oxygen was assessed, and analytical orientation showed low levels of reporting. There are many criteria within an analytical assessment, and the complexity of the task will determine which modes of cognition are involved. 40 Our findings show that the majority of the nurses had a flexible mode of cognition during decision-making when the need for oxygen was assessed. Our results are in accordance with findings from Lauri and Salanterä, which revealed that 60% of nurses employed a flexibly orientated mode of cognition. 43 Possessing sufficient knowledge is important, and the nurses’ knowledge base is essential when they assess children’s need for oxygen treatment related to decision-making. Consequently, the level of knowledge about respiratory physiology can provide a rationale for decision-making among ICU nurses, and an increased professional competence may contribute to better patient outcomes. 49 Our findings revealed that most of the nurses used the selected assessment criteria, except for the Hb–O2 curve, pulse and blood pressure, which indicates improvement areas. In order to practice nursing at a high analytical mode of cognition, all criteria should be included in the assessment of oxygen need.
Strengths and limitations
The results from this study contribute to the limited body of research on nurses’ assessments and cognitions regarding oxygen treatment in ventilated children from 0–3 years of age. The primary strength of this study was the use of the NDMI, as it is a validated instrument that has demonstrated a high internal consistency, with Cronbach’s α = 0.84. Cronbach’s α above 0.8 indicates good internal consistency. 50 Respondents from all of the Norwegian university hospitals treating ventilated children were included, and the convenience sample probably reflects the heterogeneity of nurses taking care of sick children needing mechanical ventilation. However, the selection of respondents was not random, and convenience sampling may generate the risk of bias.
Conclusion
This study showed that the nurses’ assessments for need of oxygen administration were based on insufficient information because all criteria were not included in their assessments. One-third of the nurses also had an intuitive mode of cognition when assessing oxygenation. Decision-making and assessment were therefore not at a high enough cognitive mode. This calls for the development of guidelines for oxygen administration. Education should emphasize the pedagogic methods used when students are learning about the complexity of oxygenation in decision-making tasks. Future investigations can focus on the consistency between what nurses say that they do and what they actually do when assessing and administering oxygen treatment.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.