
Abstract
This study elicited perceptions of nurses, doctors and allied health staff in rural and remote health facilities, about working with children and parents. This was a quantitative study using ‘Working with Families’, a validated and well-tested questionnaire, in the setting of seven rural and remote hospitals in North Queensland, Australia. The participants were 123 health professionals from the seven hospitals. The ‘Working with Families’ questionnaire consists of demographic characteristics and two questions about working with children and with their parents. Scores were compared and correlations sought with demographic characteristics. Scores were as follows (1 = least positive, 5 = most positive): working with children: 3.35 (95% confidence interval [CI] 3.22, 3.47), with parents 3.79 (95% CI 3.66, 3.92), mean difference –0.44 (95% CI –0.54, –0. 53; p < 0.001). No significant relationships occurred between scores and demographics. Family-centred care is the cornerstone of paediatric healthcare. People work in paediatrics and child health because they like children. Respondents were more positive about working with children than with parents. If staff find working with parents more difficult, the implementation of family-centred care may theoretically be negatively affected. Support and education about family-centred care and the newly emerging model, child centred care, may assist in overcoming less positive attitudes.
What is known about this topic
Family-centred care is difficult to implement effectively. The ‘Working with Families’ questionnaire, used in several countries consistently demonstrates a dissonance between how health professionals feel about working with children and working with parents. This may compromise the effective implementation of family-centred care.
What this paper adds
This is the first use of the ‘Working with Families’ questionnaire in rural and remote hospitals. These results show that rural and remote health staff may feel the same as their counterparts in paediatric healthcare settings about working with children and working with parents. The study needs a much larger sample to yield more reliable results.
Introduction
Many child health services declare they use family-centred care, defined as ‘a way of caring for children and their families within health services which ensures that care is planned around the whole family, not just the individual child/person and in which all the family members are recognised as care recipients’1(p.1318) as the model for care delivery. Previous studies in acute paediatric hospitals in several countries and, more recently, an Australian community child health service, have all shown that health professionals (nurses, doctors and allied health practitioners) prefer working with children than with parents.2–7 The authors of those studies have proposed that if care delivery were truly family-centred, then there would not be these significant differences. A recent study in an Australian emergency department caring for adults and children, also using the validated ‘Working with Families’ questionnaire, has also demonstrated that the multidisciplinary staff prefer working with children to working with parents. 8
A new model for the care of children in health services is emerging – child-centred care. 9 Its proponents and supporters agree that family-centred care, with the family as the unit of care, really takes the focus away from the child, who is, after all, the one who is being admitted and cared for, and whose voice is often unheard if the family is the focus.9,10 The tool used here, and its results in a range of countries,2–8 supports the idea that family-centred care is not working, and that another model centred on the child instead of the family is timely.
While staff working in a regional community child health service had high scores both for working with children and their parents, there was still a statistically significant difference toward a preference for working with children. 7 The researchers had anticipated that perhaps there would not have been this difference, because staff working in the community child health service had received education about the Family Partnership Model, 11 which is closely aligned with the family-centred care model and emphasises supported communication and partnership.
This current study measured whether the staff working in generalist rural and remote hospitals that provided inpatient and outpatient care for people of all ages, not restricted to children, held similar perceptions to those reported in previous studies. None of those facilities had a dedicated children’s ward. Rural and remote healthcare brings a range of factors that do not apply in metropolitan services, such as equity of access, long distances to travel to seek healthcare, restricted availability of services, and differing populations, to name a few.12–14 We found only two studies – one a quantitative pilot for a larger study, and one qualitative – that specifically examined family-centred care in rural and remote areas, and these were about children with cystic fibrosis.15,16 Results indicated that rural and remote location, distance and the range of factors listed did, indeed, affect how family-centred care is both delivered and perceived by those receiving it.
Methods
Setting
The setting included seven rural and remote hospitals in regional North Queensland, Australia.
Data collection tool
The ‘Working with Families’ questionnaire, previously used in other settings, has been shown to be valid, reliable, stable and easy to use.2–8 Following some initial questions about demographic characteristics, are the prompts ‘I find working with children …’ and ‘I find working with parents of children …’. The scoring system uses semantic differentials for the scores. 17 There are ten paired adjectives for each of the scales (working with children, working with parents), such as fascinating/dull, agreeable/disagreeable. With only two prompts and a simple (but highly effective) scoring system, complicated reliability statistics are not practicable. However, in other studies in this series, Cronbach’s alpha scores of 0.8 and above were consistently found2–7 and in a study using the questionnaire in the United States, Australia and Turkey 5 the scores were found to be sensitive to differences in the demographic characteristics tested between groups and countries, and so demonstrated its reliablity in measuring real differences.
Sample size, recruitment and data collection
All doctors, nurses and allied health staff working at the hospitals were invited to participate. Survey packs – 469, containing a questionnaire, the participant information sheet, and a reply-paid return address envelope – were prepared by the research team. Distribution of survey packs was coordinated by a nurse in one of the hospitals who was not part of the research team. Consent was implied by return of the questionnaire. The exact number of staff who received a questionnaire is unknown, reflecting the movement of staff within the health service, periods of staff leave at the time of survey distribution, and the vagaries of the internal mail system. One hundred and twenty-three completed questionnaires were received. This represented a response rate of 26% if all survey packages prepared were actually distributed to and received by staff.
Ethics approvals
The Townsville Hospital and Health Service Human Research Ethics Committee approved the study (Ethics approval number HREC/14/QTHS/38) and Research Governance authorised the study (site specific authorisation number SSA-14-QTHS-102).
Data analysis
The data were analysed in a similar way to previous studies that have used the ‘Working with Families’ questionnaire.2–8 The statistician in our team (AM) used Stata version 13.0 (Stata Inc., College Station, Texas) for the analyses, as with all the studies in this series.2–8 Because data were not usually normally distributed, both mean and median values of the outcomes by demographic characteristic were used. Median tests were more appropriate than mean scores where the data were not normally distributed. For comparison purposes, we have presented both mean and median scores. A p-value of <0.05 was considered statistically significant. The non-parametric Wilcoxon signed rank test was used to compare the overall mean difference between the scores for working with children and working with parents; ANOVA was used to test mean differences by categories of demographic characteristics, and the median test was used to compare mean scores of the prompts ‘Most of the time, I find working with children … (score)’ and ‘Most of the time, I find working with parents of children … (score)’.
Results
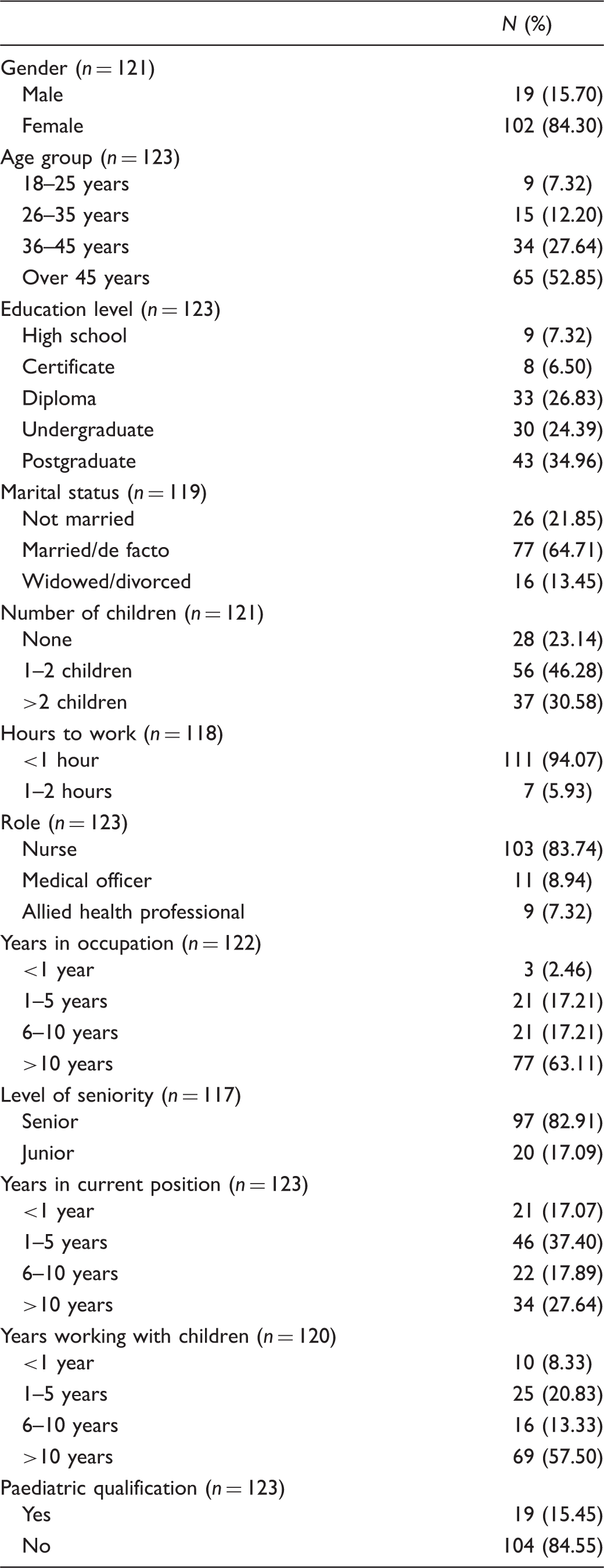
Characteristics of the sample
Demographic characteristics of respondents.
Comparison of scores for working with children and working with parents
Overall, the mean score for working with children was 3.79 (95% confidence interval [CI] 3.66, 3.92), and for working with parents 3.35 (95% CI 3.22, 3.47), with a mean difference of –0.44 (95% CI –0.54, –0.35; p < 0.001). The most positive possible score was 5, and the least positive was 1; hence, although this sample gave a more positive score for working with children than for working with parents, neither scores were very positive.
Mean and median scores for (a) working with children and (b) working with parents, by demographic characteristic.
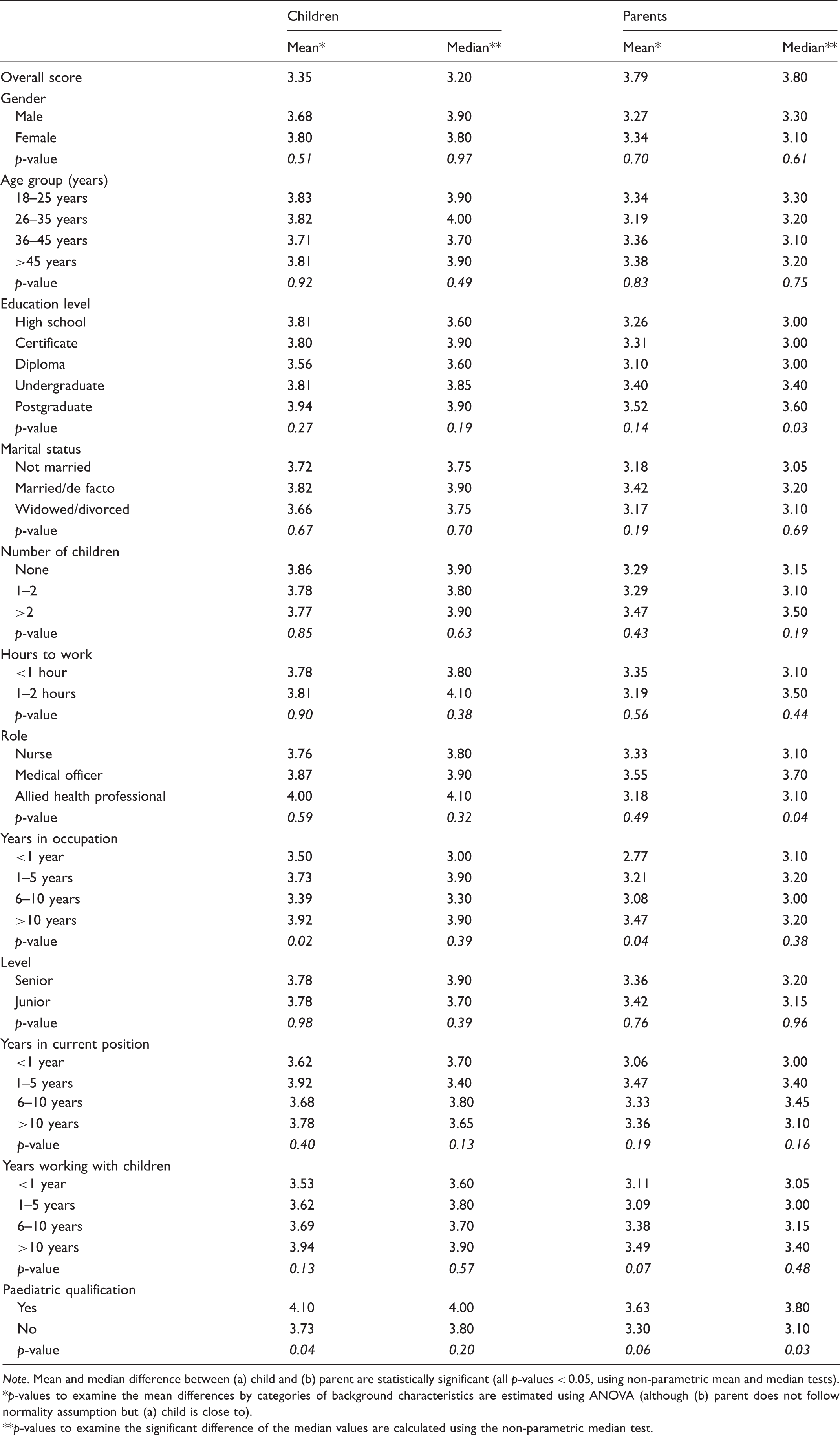
Note. Mean and median difference between (a) child and (b) parent are statistically significant (all p-values < 0.05, using non-parametric mean and median tests).
p-values to examine the mean differences by categories of background characteristics are estimated using ANOVA (although (b) parent does not follow normality assumption but (a) child is close to).
p-values to examine the significant difference of the median values are calculated using the non-parametric median test.
Discussion
The demographic characteristics of the sample were similar to those of the health workforces in many developed countries. 18 Similar to previous studies using the ‘Working with Families’ questionnaire in Australia,3–8 the health professionals gave a more positive score for working with children than working with parents. For example, the overall mean scores for working with children in those other Australian settings ranged from 4.30 (a specialist paediatric hospital), 4.29 (community child health services), 4.26 (hospitals that had a children’s ward) to 3.81 (an emergency department with a small paediatric section). Similarly, the overall mean scores for working with parents in those other Australian settings ranged from 3.90 (community child health services), 3.80 (a specialist paediatric hospital), 3.70 (hospitals that had a children’s ward) to 3.29 (an emergency department with a small paediatric section). The low overall scores in the current study may well be a reflection of the fact that rural and remote hospitals are generalist facilities without a clearly espoused family-centred model of care as there is in child health, and do not have a specific paediatric focus or specific paediatric wards. Working in small rural and remote hospitals in country Queensland often means working across multiple areas/specialties in a day/week, forever on alert for unexpected emergencies that arise in such locations. In addition, at facilities located in small towns, the staff may well know patients (adults and children) from other community activities. These pre-existing relationships may affect scores provided by staff working in rural and remote hospitals. It is unknown what difficulties may arise from such relationships and this is beyond the scope of this article.
Although family-centred care is widely espoused as the model of care in specialty paediatric settings, implementation of the model has been shown to be difficult,19–26 despite the fact that there is evidence that family-centred care improves outcomes for at least some children, most notably those with special healthcare needs. 27 Theoretically, if health professionals felt as positive about working with parents as they do about working with children, implementation of family-centred care principles might be more successful.
This is the third study conducted in the same health service in northern Australia, though in different care settings – other studies were conducted in community child health 7 and an emergency department. 8 The results contribute to the growing body of evidence that, although family-centred care is an honourable ideal, the attitudes of health professionals may influence its effective implementation. A clearly espoused model of care, scrutinising the consistency between organisational policies and the principles of family-centred care, education of staff and the adoption of other strategies known to influence implementation of a more family-centred approach may assist with the implementation of family-centred care in practice.28,29
Whether or not family-centred care is the best model for rural and remote facilities to continue to promote is too difficult to declare at this stage. The emergence of child-centred care as an alternative to family-centred care9,30 may help to answer some of the questions raised by this, and related studies. Our work has demonstrated that, overwhelmingly, health professionals prefer working with children than with parents.2–8 The new model of child-centred care returns the child to the centre of focus. 9 This does not mean that the family is ignored or excluded; rather, the family remains a vital and integral part of any child’s admission to a health service. By focusing on the child within the supportive family, we realign our perspective to ensure the child’s voice is heard and is made central. 10 Parents and other important family members are still included, 31 but if the child is the focus, then health professionals working with children may find that they are better able to employ all their skills, be they clinical, communication, and advocacy, if they promote the child’s voice within the family.
To the best of our knowledge, this is the first study of family-centred care in the specific rural and remote environment. Further testing using tools such as this one, supported by strong qualitative research, would help tease out the efficacy of the model in rural and remote care.
Limitations
This study was undertaken across several small rural, remote hospitals in northern Australia. Each facility is unique, and thus the results cannot be generalised across other rural/remote settings. The use of convenience samples limits the application of the findings; however, such a procedure was practicable given the sometimes small groups working in the included health facilities.
An important sideline to these studies is the international perspective that they bring,2–8,30,31 and they strongly support the new and emerging model of child-centred care. This allows for a network of researchers in the area across the world to work together to ensure evidence exists for implementation of models of care that suit the whole family. 32
Conclusion
Rural and remote health hospitals are structured and resourced very differently to metropolitan hospitals or specialist children’s hospitals. These differences may add another layer of difficulty to implementing the principles of family-centred care. Even though the scores were lower than in other studies using the same questionnaire, it is unknown whether these attitudes translate to less parental involvement in decision-making about the care their children receive whilst in those hospitals. It is acknowledged that the questionnaire gives limited information about health professionals’ attitudes toward working with children and their parents. The results of this study will in the future be combined with results of all other studies using the ‘Working with Families’ questionnaire. Once those results are known, future research, ideally qualitative research, could explore barriers and enabling factors that health professionals experience in delivering family-centred care in various hospital settings, thus supporting the implementation of family-centred care.
Supplemental Material
NJN881745 Supplemental Material - Supplemental material for Multidisciplinary perceptions of working with children and their parents in small rural and remote Australian hospitals
Supplemental material, NJN881745 Supplemental Material for Multidisciplinary perceptions of working with children and their parents in small rural and remote Australian hospitals by Wendy Smyth, Abdullah Al Mamun and Linda Shields in Nordic Journal of Nursing Research
Footnotes
Acknowledgements
We thank all the participants who took the time to complete the questionnaire, and we thank Ms Kay Newman who assisted with administration and editing during the project. We acknowledge the assistance of Ms Kindee Lawty, formerly Director of Nursing, Townsville Hospital and Health Service, with questionnaire distribution.
Author contributions
LS conceived and planned the study; WS prepared the ethics and governance submissions, oversaw the conduct of the study, entered data, contributed to data interpretation and manuscript writing; and AM analysed the data and contributed to data interpretation. All authors were involved in editing and writing the article and have approved the final version prior to submission.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Guarantor
Linda Shields
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.