
Abstract
The participation of patients in their treatment and care is perceived as desirable; however, patients with mental illnesses experience limited opportunities to participate in their own care. As nurses play a key role in taking care of patients with mental illnesses, this study aimed to investigate how nurses within psychiatric care settings experience patients' participation and how they act to increase it. Semi-structured interviews were conducted with eight registered nurses, four of whom worked in a psychiatric institutional care setting and four of whom worked with outpatients. Data were analysed using a qualitative content analysis approach. The analysis identified a theme: a caring relationship is a prerequisite for patient participation. This theme was further developed through five subthemes. The findings illustrate critical aspects of the caring relationship by which the nurse–patient relationship can either facilitate or impede patient participation. A caring relationship builds trust and increases the patient's sense of responsibility for their own condition. Because patients with mental illness are cared for in many different contexts, the results of the present study have implications for a broad range of healthcare environments.
Background
This article is about patient participation in the context of psychiatric care. The participation of patients in their treatment and care is perceived as desirable in many Western countries. 1 In Sweden, for example, patient participation is regulated by the Patient Act (2014: 821). 2 Among other things, this Act ensures access to healthcare, the patient's right to participation and information, the right to self-determination and the protection of integrity. Several researchers have outlined the importance of this concept.1,3 The core dimensions of patient participation have been described as learning, the caring relationship and reciprocity. 4 In the psychiatric context, participation has been described as the intertwining of personal recovery coexisting with an evidence-based biomedicine approach. 5 Within a caring relationship, nurses can create opportunities for patients to influence their own care and treatment.1,3 However, some studies suggest that patients with mental illnesses experience limited opportunities to participate in their care. This is mainly due to the nature of the illness; for example, patients may lack an adequate awareness of their own situation.6,7 A lack of concentration and the inability to focus can make it difficult for some psychiatric patients to hold a conversation. 8 This can make it difficult for the patients to convey their thoughts and wishes about their treatment and care.7,8 In such a situation, any participation needs to be adapted to the patient's health condition, but it is still desirable to encourage participation, even when the patient's input to the decision-making processes is limited. 7 Compulsory care presents a particular challenge. However, one study has shown that if healthcare professionals can embrace an attitude of reflection rather than correction, patients are more likely to perceive their care to be meaningful, albeit compulsory. 9
Studies indicate that patients with mental illnesses may fail to enter into useful dialogue with caregivers about the goals and intentions of their treatment and care. 10 In some situations, patients say that their caregivers ignore them, and they perceive that the caregivers' attitudes towards them are influenced by their preconceptions. Such circumstances can lead to the patients feeling that they are reduced as human beings and that the caregivers pay little or no attention to their concerns, perceptions and needs. 11
The quality of the relationship between nurse and patient is key to facilitating effective care and treatment; however, the absence of reflection may bring about an opposite result. Showing respect for patients and encouraging them to play an active role in their care is construed as a form of partnership, leading to support for further participation.6 Open dialogue involves a process of interaction that can assist healthcare professionals as they work with patients and their relatives in the psychiatric context. 12 Dahlberg et al. 13 argue for the need to integrate a lifeworld perspective when providing care, allowing the focus to extend to patients’ well-being rather than to their illness only. Caregivers need to hear and embrace the lifeworlds of their patients. Participation can be declared ‘successful’ when patients feel that their healthcare providers take their stories seriously.
Further studies are needed to investigate patient participation in psychiatric care. 5 Nurses play a key role in taking care of patients with mental illnesses. It is therefore important to investigate how nurses respond to patients’ participation in their treatment and care and to determine what ‘participation’ means in the psychiatric context. Psychiatric care takes place in a variety of contexts, varying from outpatient care to intensive psychiatric care, and including compulsory care. Irrespective of context, patients often find it difficult to be involved in their own care and treatment. Many patients in psychiatric care experience a lack of information about their treatment and care.11,14 At the same time, healthcare professionals working in psychiatric care struggle to meet the needs of their patients in a culture that is often characterised by biomedical and paternalistic beliefs. 5 The aim of this study is to investigate how nurses within psychiatric care settings experience their patients’ participation and what they do to increase it.
Method
This study uses a qualitative design with an inductive approach.
Participants
The participants were selected through purposive sampling15,16 due to their having experience relevant to the study's aim. The participants consisted of eight registered nurses, five females and three males, who ranged in age from 25 to 65 years. The length of their experience in psychiatric care varied from 2 to 43 years. At the time of the interviews, four of the nurses worked in an institutional care setting and four worked in a psychiatric outpatient setting.
Data collection
The interviews were conducted in a private area of the participants' places of work. All interviews consisted of three open-ended questions: What does patient participation mean to you? What are your thoughts about patient participation in your daily work? and How can patient participation be facilitated? The participants were encouraged to talk freely and to elaborate on their replies, with the interviewer asking follow-up questions, such as: What do you mean? Can you say a bit more about that? and Please give an example. The interviews were tape-recorded and transcribed verbatim.
Analysis
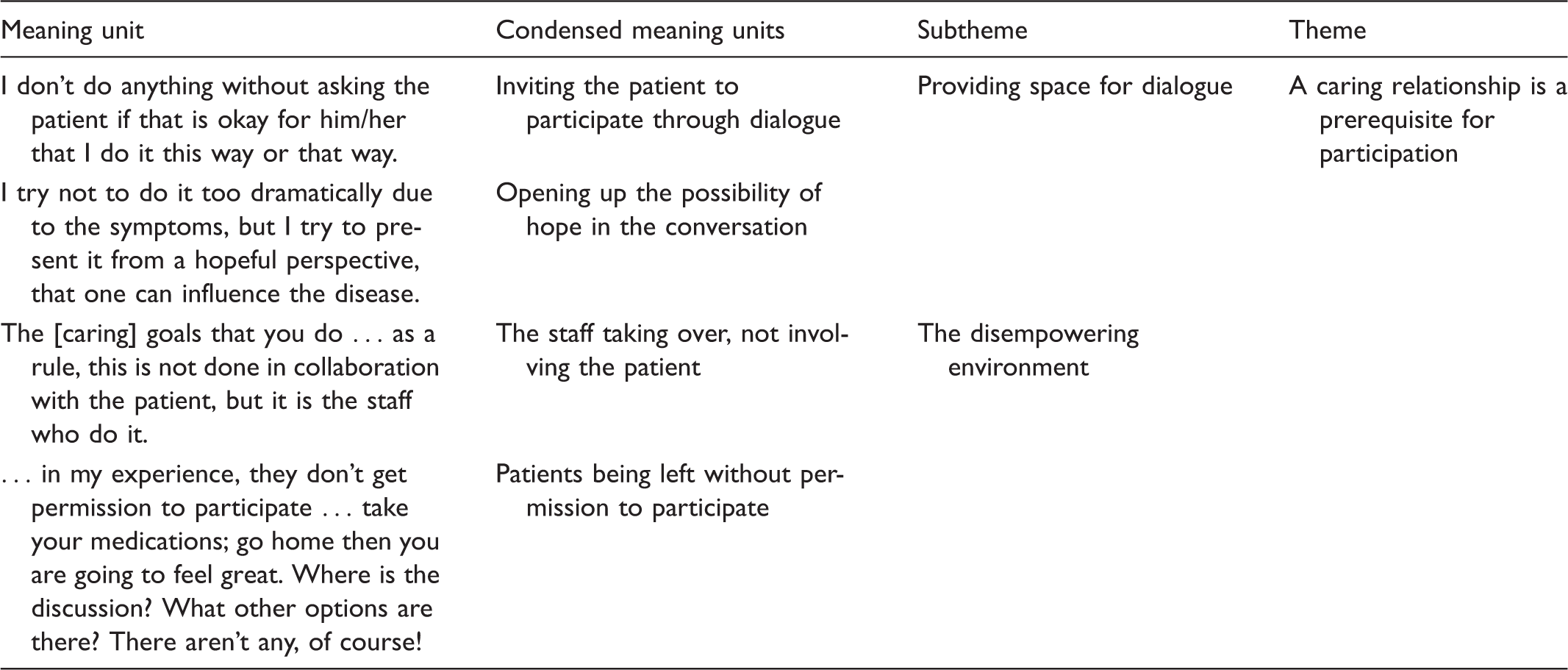
Example from the analysis process.
Overview of the theme and subthemes.

Ethical considerations
This study followed national guidelines for ethical principles in research (Swedish law concerning the Ethical Review of Research Involving Humans). 18 All ethical requirements were strictly applied. This study was conducted in accordance with the principles of the Declaration of Helsinki 19 and the Swedish Personal Data Act 20 (which, at the time of data collection, were the ruling laws, now replaced by the European Union's General Data Protection Regulations (GDPR)). 21 Permission to conduct the interviews was granted by the heads of the departments: they received an information letter about the research and were asked to recommend experienced nurses. The first author contacted the nurses recommended, and they received written and verbal information about the study. Before signing a written consent form, all participants were informed about the voluntary nature of their participation and advised that they could withdraw at any time. They were also given an opportunity to ask questions. The information given included the fact that the data would be treated confidentially, and participants were assured of confidentiality and that their privacy would be protected. No persons outside of the research group had access to the data, the data were held safely and locked away and no identifying data, such as names or places, were transcribed into writing. The analysis and presentation of the data were done in such a way that the informants' identities were completely concealed.
Results
How nurses within psychiatric care settings experience patients' participation and how they act to increase it are expressed in one overall theme: A caring relationship is a prerequisite for participation. This has five subthemes: providing space for dialogue, creating an open and welcoming environment, the patient's dependency on others, patient vulnerability prevents participation, and the disempowering environment. An overview of the theme and subthemes are presented in Table 2.
A caring relationship is a prerequisite for participation
The quality of nurse–patient relationships can either facilitate or impede patients' participation in their care. To a great extent, the caring relationship is influenced by the nurse's attitude and approach to care. Due to the vulnerability of psychiatric patients, facilitation depends on the nurse's ability to identify situations and opportunities that are suitable for patient participation. When nurses are open-minded, permissive and responsive, patients are more likely to open up and take an active part in their treatment. The caring relationship is critical, but it can easily be perceived as non-caring, especially when patients are dependent on the nurses and perceive themselves as being in an inferior position relative to the healthcare providers. Even when patients are experiencing a severe state of illness, they can still discern failures to respond to their needs. Patient participation can be influenced, even unconsciously, by the nurse's interpersonal skills in a disempowering environment.
Providing space for dialogue
Providing space for dialogue is mentioned by the nurses as very important for patient participation. Open dialogue increases opportunities to reflect together with the patients on their caring needs. During such dialogue, patients are able to talk about what they expect from the healthcare professional. According to the nurses, this increases the patient's opportunity to influence their own care. One of the nurses stated: I don't do anything without asking the patient if that is okay for him/her that I do it this way or that way. Is that okay for you? I don't do anything over their head in any way. This is an art, to meet a human being when one becomes a participant in their life; that I don't create my own picture, and the patient feels that, ‘No, it's not me; she doesn't grasp or understand me’.
A caring dialogue demands that nurses wait patiently for the patient's narrative. They must take the time to listen respectfully, so they can try to understand the patient. A caring dialogue requires time, and it needs to move in accord with the patient's own pace. It is also important to respect the patient's wishes when the patient indicates that they no longer want to speak.
Creating an open and welcoming environment
The nurses try to offer their patients opportunities to ask questions, and they try to be clear and concrete when they respond to a patient's thoughts. Patients' questions are often about their medication and the side effects that can occur. When a patient requests a medical consultation with a physician to have a discussion about their treatment, the nurses often try to meet their wishes. Another opportunity for participation comes when a patient is invited to participate during the daily rounds. This is likely to lead to a higher level of patient participation. During these meetings, patients have the opportunity to discuss their treatment and influence the way it is conducted.
According to the nurses, the participation level increases when patients are informed about their mental illnesses and how they should handle them. The nurses try to create conditions conducive to patient participation when they explain, guide and supervise. Because it is sometimes challenging for patients to participate, it is important that the nurses refrain from taking over and determining patients' treatments without their input. One of the nurses in this study noted: I think that participation is from two directions; we are involved in their care and they must be involved in their own care. We constantly try to think that the patient is an adult and usually a mature person who has resources and can take responsibility for his or her own behaviour.
The nurses describe how opportunities to participate can increase when patients are encouraged to suggest their own treatment proposal and when their wishes are acknowledged. This enables the patients to feel confident about expressing their wishes regarding the care they are receiving. Thus, an open and permitting environment is necessary before patients will feel secure enough to reflect on and express their wishes about their care. As one nurse described this: You need to tell me what your desire is, I can't guess …I encourage. I ask: what is your interest, what makes you happy? … I try to collect facts, somehow, how this patient lives when he/she is in his/her habitual state … And from that, so I try to see, with the patient's help, the actual caring situation.
The patient's dependency on others
The nurses said that patients may think they are in a disadvantageous position in relation to the nurses. This feeling of inferiority can cause them to feel agitated and make demands that can be difficult for the nurses to satisfy. This can impede patient participation. In these situations, the challenge is for the nurses and patients to view each other as equals. The nurses' position of power and authority in relation to compulsory institutional care is a hindrance to patients' participation in their care. One of the nurses commented: We decide, and we know what's right. And we also have the power to do this, so there will be some ethical dilemmas. We know what is best for the person, we believe. And maybe that corresponds to what the person needs, sometimes, but sometimes it doesn't …
Patient vulnerability prevents participation
The patients' vulnerability increases their risk of exposure within the context of psychiatric care. Some patients are fragile and find it difficult to handle themselves, and they can seek immediate satisfaction for their needs. As one nurse described this situation: Many of them [the patients] don't know … Why do we need to eat regularly? Why do we need to sleep? And how the impulse of anxiety makes it difficult to handle the day … that their emotions vacillate.
It is difficult for a patient to participate in dialogue when they are suffering from a serious psychiatric disease. According to the nurses, patient participation is particularly difficult when the patients are in a psychotic state. The nurses described how patients can have memory problems and difficulties in concentrating, which also hinder their participation. Participation can also be impeded when patients lack insight into the problematic nature of their perceptions and assumptions, and they do not realise that they need help. As one nurse noted: They [the patients] have, of course, a lot of hindrances …which can make them choose, in the same way, not to approach the caregiver.
A disempowering environment
The environment does not always facilitate patient participation. Even if the nurses know that a patient is feeling offended, powerless and inferior, it can be difficult to prevent them from experiencing these emotions. Through the nurses' stories, a picture emerged of how participation decreases when patients have no opportunity to influence their own care, for example, by asking questions about their treatment. Medications can be changed without informing the patient. An example of a disempowering or inhospitable environment would include a situation where patients did not feel they were welcome in the ward to which they had been admitted. Caregivers can also have different opinions about the care needed, and this means that there can be a lack of consensus in relation to the patient's care. The following illustrates a situation, described by a nurse, in which patients were exposed to hostility: There is a sharp dividing line between the different ward departments … all of the patients have equal value and importance — how hard can it be? And what if the staff can't come to an agreement … what will then happen to the patients? Years go by without the patient getting any help. We, maybe, get three to four new patients every day. A correct care plan must be done … while we have 14 to 15 other patients who need to be activated. Just such a thing … No, it hasn't gone that well. … they come here, and they feel enormously bad and they haven't, in my experience, they don't get permission to participate … take your medications; go home then you are going to feel great. Where is the discussion? What other options are there? There aren't any, of course!
Discussion
According to the aim of the present study, the intention was to investigate how nurses within psychiatric care settings experience their patients' participation and how they act to increase it. The results of the present study highlight the specific demands relating to the vulnerability caused by mental illness. Patient participation needs nurses to be committed to taking an active role in its facilitation. An open dialogue and a hospitable environment are key factors that support patient participation. Nurses have advantages due to their professional role; however, they also carry significant responsibilities in their relationships with patients.
Mental illnesses can limit patients’ ability to express themselves.8,22 Thus, the approach adopted by nurses when they first meet their patients is crucial. The results from this study suggest that there is a distinct lack of patient inclusion at all levels of care, including care planning. Good therapeutic practice requires the use of an open reflective approach and trying to see the individual behind the diagnosis. 22 This can facilitate cooperation between the nurse and patient. The results indicate the importance of acknowledging the patient's vulnerability and engendering trust rather than being the one who ‘knows what is best’ for a patient. In line with previous research grounded in the caring science perspective, there is a need to establish a caring relationship in which the caregiver and patient can together create a path that leads to well-being. 23
Less time spent with patients means less contact with them and less understanding of their expectations and needs. When the nurses in the present study described the overcrowded departments and how they had no time to create individual care plans with their patients, they indicated that they have no opportunity to get to know their patients at a deeper level or to establish an alliance based on mutual trust. Jones 24 describes the importance of patients being familiar with their own situation and with their illness. This can give the patient a sense of security, which helps them to open up and convey their requests for help at an early stage of their disease. According to earlier research, nurses need to realise the importance of patient-centred care in which they are close to the patient and where they are able to translate their knowledge into action. 25 Studies report that it is important to include patients more actively in their care planning, 26 and that nurses play an important role in facilitating several dimensions of their participation, such as shared decision-making. 27 This is in line with the findings of the present study that highlight the importance of caregivers taking time to get to know their patients so as to encourage their participation, and how the caring relationship not only creates trust but can also facilitate opportunities for patients to take responsibility for their own care. Thus, there seems to be consensus regarding the importance of involving patients more actively. However, it seems to be hard to actually implement a caring relationship in encounters with patients.
As has been highlighted, several dimensions contribute to increased patient participation, but there were also dimensions in the nurses' descriptions that contribute to non-caring. For example, a disempowering environment prevents participation, and business and task orientation become obstacles to collaboration. Due to the nurses' lack of time and the vulnerability associated with patients with mental illness, the present study's results indicate a lack of patient inclusion at all levels of care, including care planning. These aspects of structures preventing patient participation are also evident in previous studies. 26 In addition, in some situations, caregivers choose to be compliant with their colleagues' opinions rather than considering the patient's requests. 28
The situation that the nurses found most challenging was compulsory institutional care. In this situation, the nurses found themselves in asymmetric power relationships and, although they frequently tried to involve the patient, this was challenging. Hamann et al. 29 stated that there are many occasions where psychosocial treatment can be discussed with a patient. However, there are also obstacles that impede this, especially when patients cannot make proper decisions due to the nature of their mental illness. Restrictions or enforced actions should only be used if an attempt to share decision-making has failed. The nurses in the present study described the impact that these situations can have on the relationship when they are forced to decide for the patient.
The study's findings also highlighted the importance of the nurses' competence and professional experience. Being unable to identify the factors that impede participation, or not having sufficient time to do so, both affect the quality and safety of the patient's care. Participation is not a general or standardised phenomenon; rather, it is highly individual, and it does not need to cost a lot or take a great deal of the caregivers' time. Instead, it can simply involve the way in which the professionals express their attitudes towards their patients.6,9,30 However, special training programmes may be needed to facilitate healthcare professionals' readiness to support patient participation.6 More time for supervision and reflection might also be necessary. 9
Methodological considerations
Some of the findings of this study are applicable, with certain modifications, to other units, and transferability to other contexts can be undertaken, but with consideration. Because the participants were nurses who worked in both institutional care and psychiatric outpatient settings, and their age and experiences varied, the results represent a range of experience. According to Polit and Beck, 16 the sample size in qualitative research is determined by the possibility of achieving data saturation. If informants are able to reflect appropriately on the research questions, a relatively small sample can contribute to a level of satisfaction. In the present study, eight registered nurses were included. They all had experience in relation to patient participation and were able to contribute to a rich description to the study's aim. According to Holloway and Galvin, 15 rich data is of greater importance than a larger sample size.
The interview technique using open-ended questions stimulated the participants to share extensively about their experience. The chosen method was suitable for analysing the data and this made it possible to formulate the theme and its subthemes. Studies using content analysis may be considered trustworthy because they allow participants to provide rich descriptions of a phenomenon. The results need to be presented in a logical way, and the level of abstraction should be accurate and supported by relevant citations. 31 All these considerations were addressed during the research process. The intentions were to address aspects of relationships and to address the underlying meaning of the text, described as latent content by Graneheim and Lundman. 17 Although the results might differ in the level of interpretation, the analysis process contributed to the highlighting of trends in the underlying meaning.
In future research, it would be interesting to determine how patients in psychiatric care settings experience their own participation in their treatment and to compare that with the experience of other patient groups.
Conclusion
A hospitable and empowering environment that mediates understanding of the patient's situation can increase the chance of patients participating in their care so that the nurse does not take over. However, this requires nurses to have the time to support patients as they find ways to handle their situation and to ensure their well-being. As highlighted in this study, lack of time and support impedes patient participation. Nurses need time to reflect on their daily work and they need to be educated about ways of facilitating patient participation so that they can support their patients.
The findings of this study will be valuable not only in the psychiatric context but also in other healthcare settings. Patients with mental illness are cared for in many different contexts. Thus, it is important for caregivers working in a broad range of healthcare environments to consider how best to facilitate patient participation. The interpersonal skills of healthcare workers are important in every setting and situation where they meet patients or individuals in need of care.
Footnotes
Acknowledgements
The authors would like to thank the participants in the study and Linda Karlsson, Sofia Vesterinen and Levente Keresi for their support during the process of conducting this research study.
Author contributions
All authors have seen and approved the final version of the manuscript being submitted. They warrant that the article is the authors’ original work, has not received prior publication and is not under consideration for publication elsewhere. All authors have contributed equally to the manuscript and have made substantial contributions to all of the following: 1) the conception and design of the study, and analysis and interpretation of data, 2) drafting the article 3) final approval of the version to be submitted.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.