
Abstract
Preventive home visits carried out by healthcare professionals are intended to promote the health and independence of home-dwelling older persons and to prevent functional decline. The aim of this study was to describe nurses’ experiences of the benefits from long-term follow up with annual preventive home visits to older people in a Norwegian context. We conducted semi-structured interviews with nine nurses who performed the service. Manifest and latent content analysis revealed benefits within three themes: sustained ability to live independently and thrive despite age-related changes, eased transition to other healthcare services, and improved healthcare service planning. Two headlines describe the longitudinal processes involved in the creation of benefits: ‘The processes of establishing, sustaining, and widening a longitudinal room of possibilities’, and ‘The individualized health-promoting processes – the ongoing gardening work. Professional, contextual and structural factors influenced the nurses’ ability to support older persons’ changing needs during the aging process and thus their health and independence.
Introduction
The majority of older persons want to age in their own homes. 1 To support their ability to remain independent is a socio-economic goal in Western countries, impelled by the upcoming demographic changes and limited healthcare resources. 2 Thus, proactive initiatives that aim to sustain older persons' functional ability are encouraged.2,3 One initiative is preventive home visits (PHVs), that is, home visits to independently living older persons conducted by professionals, starting before disease and age-related changes set in. In general, PHVs are intended to promote home-dwelling older persons' health and independence and prevent functional decline. 4 Nurses are the most frequently used professionals in PHVs internationally and in Norway.5,6
There exists a variety of PHV interventions and regular PHV services internationally that differ in terms of target groups, aims, content, visitors' competence, frequency of visits and length of follow up. While early PHV interventions had a predominant focus on disease prevention,7,8 later PHV reviews display a more varied and broader focus.6,9 Recent studies demonstrate that Scandinavian PHVs often include disease prevention as well as support for various aspects of subjective health and coping, and thus reflect a comprehensive understanding of health and health promotion.10–12 In Scandinavia, a common approach is to offer annual PHVs to a general population of older people after a model from Denmark, in which annual PHVs from the age of 75 were legislated from 1996.4,5
It is difficult to measure effects of comprehensive PHV services because these interventions are complex and unstandardized, and benefits from health-promotive and disease-preventive initiatives often appear first after several years. Most PHV research has consisted of randomized controlled trials (RCTs) that have tested interventions of relatively short duration and follow up, and assessed outcomes merely related to a biomedical understanding of health.6,13,14 Even if the results of these RCTs varied, they demonstrated the possibility of modifying several health-related factors. However, heterogeneity and insufficient data rendered it difficult to produce consistent evidence about effectiveness.6,9 Knowledge about long-term benefits from PHV services are therefore limited.
Several researchers have questioned the one-sided focus on biomedical outcomes in PHV studies and have recommended studies that explore and assess other outcomes from PHVs.14–16 Others have questioned the use of RCTs to evaluate PHVs because these interventions are multi-focused and complex, and involve social processes, indeterminate problems, and uncontrollable variables.4,17 To be able to produce recommendations for how to create efficient PHVs, there is a need for qualitative research that provides more in-depth knowledge about the inherent processes and what contributes to the benefits for older people. In particular, the experiences and opinions of those involved with PHVs are sought.8,14,17,18
Some results exist from qualitative PHV studies. Studies exploring older people's experiences reported that PHVs could support their feeling of safety/security and sense of control,10,19–21 improve coping and preserve independence,10,21 strengthen their sense of worth,10,19,20 and support a good life. 10 Preconditions for positive outcomes were: understanding the service's aims, a trusting relationship with the visitor,10,15 and the visitors' communication competence and ability to respond to individuals' needs and preferences.10,15,19,21 Even if nurses are the most frequently used professionals in PHVs, their views have been poorly described. The nurses in a Swedish study reported that the quality of the dialogue in a first visit depended on the older persons' trust level, cooperation, and understanding of the aims of PHV, and the nurses' communication skills and attitudes. 12 We found two studies based on nurses' documentation of PHV interventions with monthly or more visits, during 22 and 8 months respectively: one set of visits being to disabled persons in the USA, 22 and one to non-frail older people in Japan. 23 Both found that positive outcomes depended on the nurses' ability to build and maintain trustful, collaborative relationships with their clients. Facilitators to positive outcomes were multiple visits, communication skills, professionalism, shared decision-making, a caring approach and the ability to give an adequate response to an individual's needs or problems.22,23 Barriers consisted of an older person's disability worsening, lack of interest, or low motivation for change. 22
In sum, the knowledge about long-term, annual PHVs is limited. To amend this gap in the literature we therefore studied nurses' experiences from a well-established comprehensive PHV service offering long-term annual follow up. In this study, we hold a comprehensive understanding of health, which is a dynamic, complementary relationship between pathogenic and salutogenic perspectives, as well as objective and subjective aspects. 24 The knowledge generated might guide healthcare authorities in planning PHV services, and support new professional visitors.
Aim
The aim of this study was to describe nurses' experiences of the benefits from long-term follow-up with annual PHVs to a general population of older people within a Norwegian context.
Methods
Study design
This study is part of a comprehensive case-study evaluation of a PHV service in a Norwegian municipality. We applied a qualitative exploratory approach due to limited knowledge of professionals' experiences in conducting long-term PHVs. 25
Setting
The setting for this study is the Norwegian welfare state model, which offers universal healthcare services, mainly free of charge, based on professional judgment of need. All municipalities have the responsibility to offer essential healthcare services to their inhabitants, including preventive and health-promoting healthcare, but each municipality can decide how to manage this responsibility. The PHV service under study took place in an urban municipality in the south-eastern part of Norway with 60,000 inhabitants. The municipality was one of the first to introduce PHVs in Norway; from 1999 as a pilot project in one part of the city, and from 2005 to all home-dwelling citizens from the age of 75 years who did not receive ordinary home healthcare.
Given the heterogeneity of PHVs, a short description of the service in the municipality follows. The stated aims of the PHV service includes the promotion of older citizens' health, well-being, and safety, supporting their ability to live at home for as long as possible, and the reduction or delay of the need for more comprehensive healthcare services. 26 Ten nurses delivered the service to approximately 2000 home-dwelling seniors aged 75 to 97 years, and each offered PHVs to older persons in one healthcare district in the municipality. The nurses had developed a theme guide for conversation during the visits, covering life history, physical and mental health status, functional ability, nutrition, activities, the home, family, and social network. The nurses offered support related to individual needs and preferences within these areas, and could refer the user to other municipal services if needed. The PHV service offered annual visits, but the service users were encouraged to call their PHV nurse if they needed any help or advice between ordinary visits, and the nurses could offer additional visits if it was deemed necessary. The service continued as long as the older person wanted it, until they needed more comprehensive healthcare services, or the person died.
Participants
We applied strategic and convenient sampling. 25 We aimed to study PHV nurses with rich experiences from long-time follow up of PHV users, and authorities in a local municipality wanted an evaluation of the PHV service initiated 11 years earlier. The ten nurses who performed the service volunteered to join the study. We excluded one nurse because she had only worked in the service for 15 months. The nine nurses covered 8.2 full-time equivalents, and had from 7 to 11 (mean 8.3) years of experience with PHVs. Each nurse had responsibility for 160–280 PHV users. All nurses were female, had had experience in geriatric nursing before starting with the PHV service, and seven had completed postgraduate education in geriatric nursing, dementia care, or mental health care. All met the criteria of being information-rich about the research topic. 27
Data collection
The first author collected the data through semi-structured interviews, which had an open conversational format, but a clear purpose, and were well suited to gain understanding of the nurses’ experiences with conducting PHVs. 28 We developed an interview guide to ensure that the conversations would cover the research questions. 28 As a function of wanting rich descriptions about the nurses’ work experiences, we started the interviews with an open question: ‘Please tell me about your work as a PHV nurse’. The following themes were included in the interview guide: descriptions of their long-term health promotive and preventive work, experiences of the users’ problems and their benefits from long-term follow up, what they perceived as important for positive outcomes with the service, and challenges in their work. The interviews lasted from 75 to 120 minutes and took place in an office in a healthcare district, or at the university. The interviewer made reflexive notes directly after each interview. A secretary transcribed all the interviews verbatim from an audio-recording, covering 353 pages.
Ethical considerations
The Norwegian regional committee for medical and health research ethics granted approval for the study (ref. 2011/122b), and the municipality's director of healthcare and social services granted formal permission to conduct the study. In line with the Declaration of Helsinki, 29 we gave the participants written information about the study, including their right to withdraw, and all granted their informed consent prior to being interviewed.
Data analysis
We performed qualitative content analyses inspired by Ritchie and Spencer's framework method.30,31 Its use allowed for systematizing the content of condensed meanings related to a research question, while keeping the content of each interview intact. The framework method also allowed for transparency and validation of the coding process. 31
The preventive home visit nurses' experiences of benefits from long-term follow up.
During the analytic process we identified underlying meaningful content related to how the nurses worked and the processes involved in the creation of the benefits. This content described longitudinal, intertwined processes that did not fit a thematic analysis and representation. A comprehensive analysis and interpretation, including shared discussions among the researchers, resulted in two descriptive headlines illustrating these processes, with the corresponding descriptions and examples. We presented our interpretations of the processes to the informants, who approved the interpretation. The two processes representing the nurses' views on the creation of benefits from long-term PHV are presented in the last part of the findings section.
Findings
The PHV nurses' experiences of benefits from long-term follow up
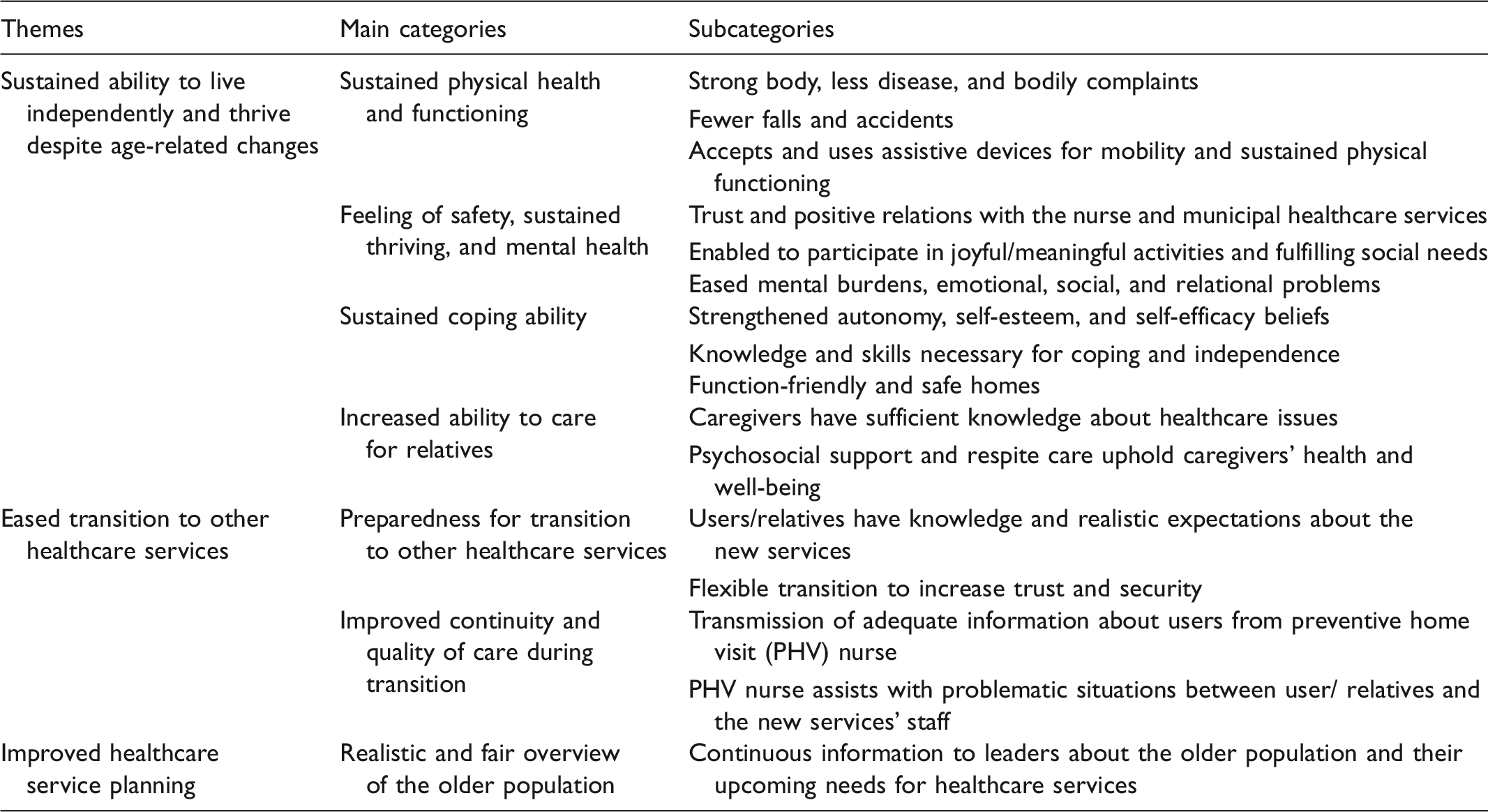
The analysis revealed benefits within three main themes: sustained ability to live independently in one's own home despite age-related changes, eased transition to other healthcare services, and improved healthcare service planning. The themes, categories, and subcategories are presented in Table 1.
Sustained ability to live independently and thrive despite age-related changes
Sustained physical health and functioning was perceived as a precondition for the users’ ability to live independently. Many responded to the nurses’ encouragement and recommendations related to physical activity, a healthy diet, and other aspects that contributed to sustaining a strong body. If there was a need for continuing support, the nurses could recommend pertinent local activities/services; for instance, physical training groups run by municipal physiotherapists. The nurses offered professional advice for common bodily problems and complaints; for instance, related to sleeping, digestion, or incontinence. They did not systematically assess disease/risk of disease, but used their professional nursing abilities and were receptive to medication problems and symptoms regarding new or existing diseases, as this nurse clarified: ‘She had lost ten kilos since last year, so then we have to find out why, you know’ (Informant 1). When they suspected disease-related problems, they advised the users to contact their GPs (general practitioners). The nurses also believed that their focus on safe homes had prevented falls and accidents. If functional problems did occur, the nurses, in cooperation with physiotherapists and occupational therapists, could help the users find and accept relevant assistive devices that could extend their self-care ability.
Feelings of safety, sustained thriving and mental health covered other critical benefits. The nurses became each user's personal contact person, who they could call if they needed help or support, which sustained a trustful, positive relation. Information from the nurses about the users' legal rights and the municipality's healthcare system added to trust and safety issues for future health problems. The nurses also helped older individuals overcome various barriers for participating in meaningful and joyful activities and fulfilling social needs. One of the nurses illustrated this: I helped a man with walking problems who had not been outdoors for four years, to get a mini-crosser. That gave him entirely new possibilities; that is really health-promotive work. He can go shopping, he has contact with his neighbors, he drives to the next village to visit his daughter every week. He suddenly got a life. (Informant 2)
Sustained coping ability covered mental as well as practical issues. Supporting the users’ autonomy was linked to the service's aims, as this nurse explained: ‘It is vital that they understand that our job is not to manage their lives, but to support them in taking responsibility for their own life’ (Informant 6). If appropriate, the nurses increased the users’ awareness about topics they knew were essential for independent living, offered relevant knowledge and advice, as well as psychosocial support to improve self-esteem and self-efficacy. Function-friendly and safe homes are important for coping abilities. The nurses offered to assess the home and inform users about available aids and possibilities for economical and practical help to carry out home modifications. They also offered information about alternative housing arrangements.
The nurses increased older persons’ ability to care for relatives with serious diseases, such as dementia. They provided insight about relevant healthcare issues, offered psychosocial support, and encouraged acceptance of respite care, as this nurse stated: ‘We cooperate with them to find acceptable respite care, to help them manage and hold out as long as possible’ (Informant 3). This help could relieve the emotional, mental, and physical strain related to being a caretaker, which could sustain their own health and well-being and extend their capacity to care for relatives at home.
Eased transition to other healthcare services
When users developed a need for more comprehensive care the nurses contributed to the users’ preparedness for transition to other healthcare services; most often home healthcare (HHC). Specific information gave users and relatives knowledge and realistic expectations that could improve cooperation with the new service providers, as this nurse explained: ‘You must answer honestly: yes, many people will come and go, but you will get better contact with some of them, so contact them if needed’ (Informant 8). The PHV nurses transferred adequate electronic information about the users from the PHV service to the new service, which saved time and facilitated continuity and quality of care. If users with dementia or mental illness needed flexible transitions to increase feelings of trust and security, the PHV nurses could extend the transition period and gradually introduce and transfer responsibility to the new staff. This preparatory work with users and relatives also eased the situation for the professionals in the subsequent service. The PHV nurses could assist if problematic situations between the user/relatives and the new services’ staff occurred after transition, as this example shows: ‘If there became problems related to the relatives, they say: We need to arrange a meeting, you know these relatives, can you join us?’ (Informant 9). This contributed to sustaining relations between the user and HHC staff.
Improved healthcare service planning
The nurses' weekly reports gave the municipal healthcare leaders an overview of the older population and continuous information about upcoming needs for healthcare services. They also shared information to improve the services to older citizens. The longitudinal approach of the PHV service enabled municipal authorities to fulfil their lawful obligations to maintain a continuous overview of the older population to offer necessary healthcare and plan for future needs.
The nurses' views on the creation of benefits from long-term PHV follow up
The analysis of the content related to the nurses’ work revealed that the creation of benefits of the PHV service rested on complex, longitudinal relational and professional processes. Two headlines describe the interpretations of these processes: ‘The processes of establishing, sustaining, and widening a longitudinal room of possibilities’, and ‘The Individualized health-promoting processes – the ongoing gardening work’.
The process of establishing, sustaining, and widening a longitudinal room of possibilities
As a non-compulsory service in the older person's home the nurses’ support was dependent on older individuals’ acceptance of the service. During the first visit the nurses paved the way for a continuing constructive collaboration, i.e., ‘the longitudinal room of possibilities’, in which the nurses’ personal and professional competence met the users’ expectations, preferences, and changing needs and problems during the aging process. The establishment of constructive collaboration ensured shared understanding of aims, roles, and responsibilities. The nurses’ role was to raise consciousness about important topics and offer knowledge and support that might enable the users to sustain their health, well-being and independence as they aged, not to tell people what to do and/or do things for them. The users’ role was to provide necessary information and utilize the service constructively, including contacting the nurse if they needed help, information, or advice between annual visits.
This initial work also included the intertwined processes of getting to know each other and developing trust. The nurses therefore prioritized relational aspects during the first visit and sought to support the users' feelings of value, self-esteem and safety. The users' level of trust defined what information they shared, and a strengthening of trust would improve collaboration, thus widening the room of possibilities. The second visit was perceived as particularly important for the widening process, but some needed several visits before they would talk about sensitive topics or make a call and come forward with upcoming needs or problems. The longitudinal approach facilitated the establishment of a trustful relation before severe problems arose. Violating the established trust could lead to a narrowing or a closure of the room of possibilities, and continuous relational work was therefore an integral part of the nurses' work during the entire follow-up period.
The individualized health-promoting processes – the ongoing gardening work
The majority of users were relatively fit and healthy when entering the service at age 75 years. During the years of follow up, various age-related changes, onset of disease, deterioration and losses often changed their situations. The nurses' way of working shared the characteristics of ongoing support for long-term processes, which demonstrated an equation with the work of a good gardener. We will therefore use this as a metaphor in the following.
The ongoing gardening work had two dimensions, the first was: To decide what to grow and to sow a seed. The longitudinal room of possibilities gave the users opportunity to bring in their problems, needs and wishes, and the nurses to assess each user's health, life situation and home environment regularly, and identify potentials for health promotion/prevention based on the totality of information. The nurses underscored the need to explore the users' awareness, opinions and status related to these potential areas. Respect for the users' right to decide their own life was a basic value in the nurses' stories, and the focus for further health promotive work, what to grow depended, therefore, on shared decisions based on the users' priorities and needs. However, the awareness-raising could often be a seed that started a process of considering, which might slowly grow into readiness for constructive actions.
The second dimension of the ongoing gardening work was: Watering, fertilizing, and supporting. Several of the benefits related to physical functioning, thriving and coping ability required that the older person made decisions, carried out practical actions, or changed their way of living. The users’ capacity to adapt constructively to aging varied. For some users, a rise in awareness about potential areas for health promotion/prevention/adaptation, or relevant information and encouragement might be sufficient. However, the nurses experienced that for many older people such actions relied on complex processes, where physical or psychological barriers led to ambivalence or difficulties, for instance in deciding about their future residence, accepting the usefulness of helping aids or carrying out life-style changes. The nurses therefore repeatedly watered and fertilized these long-term processes, offered relevant information, supported the users’ motivation and considerations, and acknowledged small improvements and autonomous decisions. They had good experience with ‘sluicing’ users who wanted life-style changes into activities or services that could offer them continuous support for the desired changes, such as exercise groups for seniors or social activities in the local senior center. To be able to suggest acceptable and suitable activities they emphasized the importance of in-depth knowledge about the users, and about local activities and services for seniors. These efforts led to considerable positive changes for many users, but not always and not for all. For some, the sum of watering and fertilizing of several small plants over time could make a difference, and the nurses advised service providers to be patient and have realistic, modest expectations of life-style changes.
The nurses also helped the users to cope with or compensate for the losses and gradual deterioration that often accompany the aging process. The longitudinal room of possibilities facilitated ongoing practical, psychosocial and emotional support, and the ability to discuss and seek advice for various health-related matters related to the benefits described in Table 1. The nurses' ability to support the users rested mainly on their professional competence, but also on their opportunity to cooperate with, and refer users to other municipal professionals with specialized competence; such as physiotherapists and occupational therapists. The lack of formalized cooperation with GPs meant that collaboration about disease prevention was dependent on each GP's goodwill.
The nurses experienced that transportation problems, waiting lists or lack of suitable activities could hinder the users' participation and hamper the creation of benefits. They also experienced gaps in the healthcare services for older persons with mental disease, and those with beginning cognitive problems living alone. When the nurses detected needs for help in these groups, they felt ethically responsible to offer the necessary help, which could take up a substantial part of their working time and reduce their capacity to fulfil the services' aims.
Discussion
The nurses described a variety of benefits related to subjective and objective health issues that supported older users' ability to live independently and thrive in their own home despite age-related challenges. The benefits included sustained physical health and functioning, feelings of safety, sustained thriving and mental health, sustained coping ability, increased ability to care for relatives, and preparedness for transitions to other healthcare services. Several researchers have questioned the dominance of biomedical outcomes in PHV studies,8,15,32 and many of the described benefits are seldom or never used in quantitative PHV studies. Several of the described benefits are similar to those identified in previous qualitative studies of users' experiences with PHV,10,19 which supports the belief that the benefits identified here might be relevant for PHV users in other contexts. The benefits also correspond to older people's definitions of aging well as a multidimensional concept, comprising sustained health, ability to adapt, autonomy and independence, social relationships and life satisfaction.33,34 Therefore, we suggest that evaluations of comprehensive long-term PHV services should include outcomes reflecting a comprehensive understanding of health.
We could not find benefits related to support for informal caregivers or transitions to other healthcare services in previous PHV literature. The evidence for caregiver support to reduce the need for professional help and sustain the caregivers' health is well documented. 35 The interest in problems related to transitions between different healthcare services is increasing. 36 We consider these new findings interesting as they extend the knowledge about potential benefits of PHV and open up interesting possibilities for the use of longitudinal PHV services.
The service had a limited focus on disease prevention. Prevention and early detection of preventable disease is a prioritized strategy internationally. 2 Even if the majority of older persons see their GPs regularly, many have undiagnosed medical conditions, which if treated properly could reduce the risk of severe complications or comorbidities. 37 A risk-based PHV intervention where nurses followed up with simple disease-preventive measures showed promising long-term effects.13,38 The necessity for close cooperation with GPs is underscored in several PHV studies.11,22 In Norway, structural barriers limit cooperation between PHV services and GPs, leading to missed opportunities for longitudinal PHV services with competent nurses to add the benefits of preventive measures for their users.
The benefits were created through individualized, complex and longitudinal relational and professional processes. The possibility to spend time – in each visit and during the long-term follow up – was a main characteristic of the nurses' work. Several reviews of PHV interventions recommend long-time follow up16,39 but do not explain why. The present study showed that a lasting, collaborative, trusting relationship, the room of possibilities, was a precondition for the creation of benefits. The establishment of such rooms included developing shared understanding of the service's aims and roles. Earlier PHV studies have found that poor understanding of the aims and roles of PHVs could reduce acceptance and utilization of their services.15,40 Trust and constructive collaboration were identified as essential in qualitative PHV studies,12,15,22 as well as other interventions to older people.41,42 The time for users to judge the nurses' personal and professional trustworthiness varied, and some users needed several visits before they engaged in constructive collaborations. The need to spend time to develop high-quality relations and personal trust, and the importance of high-quality relations for openness, quality of care, and patients' involvement have been confirmed in other studies.33,42
The longitudinal approach facilitated ongoing gardening work that allowed nurses to attend to the users' current needs in each meeting, but also to follow up and support the users' long-term changes, decisions, and adaptation processes. Collaboration with the users identified relevant areas for health promotion based on users' needs and preferences, and nurses strove to provide tailored support and adequate responses to the needs, wishes and problems brought into the room. These ways of working coincide with recommendations for support of life-style changes 43 and principles of person-centered care, shared decision-making, and motivational interviewing,22,44–46 which are related to patient satisfaction and positive outcomes in healthcare settings.
We found that contextual and structural factors outside the longitudinal room of possibilities influenced the creation of benefits for users. The nurses had access to many resources that might be utilized to support users' needs, including other healthcare services and local activities for older people. Established routines for inter-professional collaboration with physiotherapists and occupational therapists supported gardening work and improved service quality, while the lack of formalized cooperation with GPs limited disease-preventive aspects of the service. Capacity problems in certain services, mobility problems, and lack of transportation hindered participation for those with limitations. Similar barriers were found in a recent UK study which emphasized the importance of facilitating social participation in health-promotive services. 47 A consistent municipal health promotive policy and coherent healthcare services are therefore necessary for maximizing the potential of PHVs to improve older persons' health and independence.
Strengths and limitations
The informants' extensive, long-term experience is a strength of the study, and this sample covers almost the full body of experience of over ten years of conducting the PHV service in the municipality. There are always several possible interpretations of qualitative data. The informants' approval supported our interpretations of the processes involved. The use of the framework method provides transparency of categorization and validation of findings, but using the Norwegian language in analyses limits transparency. Preventive home visit services are dissimilar, which limits the transferability of results to services with a similar approach/scope and context.
Conclusions
Constructive adaptation to aging may require challenging acceptance, decision-making, and changing processes. Long-term follow up with annual preventive home visits provided by well qualified nurses offers opportunities for tailored long-term support for older people's changing needs during the aging process, which might sustain health and independence. Personal and professional competence and contextual and structural factors influence nurses' ability to create benefits for users. The study may provide important insights for those who plan to introduce or develop PHVs. More studies will be required to explore the relevance of the benefits seen in this study.
Footnotes
Acknowledgements
We thank all of the study participants for their time and involvement, and Bjørg Landmark in the Research and Development Unit in the Municipality of Drammen for facilitating the study. We also thank the University of South-Eastern Norway and the Municipality of Drammen, Norway, for funding.
Funding
The authors received financial support for the research of this article from the Municipality of Drammen, Norway and the University of South-Eastern Norway.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.