
Abstract
This study was a part of a municipal research and development programme in home healthcare (HHC). The Oulu Patient Classification instrument (OPCq), part of the RAFAELA Nursing Intensity and Staffing system, was used to measure nursing intensity (NI) for the first time in HHC in Norway. The aim was to describe nurses’ work experiences and perceptions of the usability of the OPCq instrument when classifying NI in HHC. Twenty-two members of staff participated in four focus-group interviews. Content analyses were used to analyze and interpret the data. Three themes emerged: 1) Classifying the modified OPCq levels correctly; 2) Technological problems hinder use of the instrument; 3) Classifying NI when time pressure dominates. The OPCq instrument is useful in classifying NI, although some minor adjustments might be needed for its use in HHC. The nurses considered the OPCq instrument useful in illuminating the actual work situation in HHC and the time pressure they experience.
Introduction
In the next few decades, the population of older people in developed countries will increase. 1 Currently, the number of hospital and nursing home facilities (NHFs) is decreasing, resulting in a growing concern about the expanding need for home healthcare (HHC) services. 2 As people age, their health needs become more chronic and complex, and this is a challenge for HHC. In an era of healthcare system changes, the documentation of patient intensity, nursing care and nursing resource allocation is essential. Safety risks in HHC have been associated with patients with polypharmacy, inhibited physical function and/or during adverse events such as falls, unintended weight loss, new emergency room visits or new hospital visits. 3 Visits by multidisciplinary geriatric teams to home-dwelling older persons have been shown to reduce hospital and emergency room visits. 4 Some municipalities in Norway offer promotive and preventative home visits realized by nurses, 5 but in acute/emergency situations older persons must visit a GP or the emergency room.
A reduction in the amount of time allowed for home visits and greater staff responsibility have been seen in HHC in Norway, 6 including organizational barriers that lead to clinical priorities and rationed care yet do not address existing comprehensive workload or staff shortages. 7 In NHFs, fewer nursing hours have been associated with deficiencies in care 8 while more nursing hours have been associated with better care. 9 To meet patients’ individual needs and realize person-centred care when nursing resources are limited, the correct allocation of nursing staff is essential.
Several instruments have been developed for use with patients in HHC settings: the Clinical Care Classification (CCC) system, 10 Minimum data Set-Home Care (MDS-HC), 11 Resource Utilization Groups (RUG III-HC),12,13 Resident Assessment Instrument for Home Care (RAI-HC),14,15 Community Health Intensity Rating Scale (CHIRS), 16 The Easely-Storefjell for Caseload/Workload Analysis Instrument (CL/WLA), 17 Community Client Need Classification System (CCNCS)18,19 and Caseload Intensity Tool (CIT). 20 However, these instruments are limited because they do not measure patients’ daily care needs, do not provide calculations for the optimal (daily) allocation of staff resources and use comprehensive but long scoring sheets.
The Global strategy and action plan on ageing and health 1 specifies several key strategic objectives, including aligning health systems to the needs of older populations and improving the measurement of, monitoring of and research on healthy ageing. To meet such requirements in HHC, one should systematically and regularly monitor patients’ needs for help, care, support and the interventions needed to meet these needs. In HHC, the classification of nursing intensity (NI) after each visit can provide an overall picture of patients’ needs and nurses’ workloads. NI is not equivalent to workload in that it is a concept closely related to ‘patient dependency’, ‘acuity’ and ‘severity’; 21 non-patient factors such as contextual and/or organizational factors and staff/nurse related factors 22 also affect nurses’ total workload. Total nursing time includes both nursing activities and non-nursing activities, 23 and exploring and measuring nursing workload can have a beneficial effect on nurse retention and requirement. 24 Mildon has found no evidence to indicate that nursing workload in HHC has been routinely measured. 24
The RAFAELA system is a proven and useful Finnish tool for nurse leader staff allocation in hospital settings, 25 however it has not previously been tested in an HHC setting. The actual study was a part of a research project testing the RAFAELA system in Norwegian HHC, with the aim of describing nurses’ work experiences and perceptions of the usability of the Oulu Patient Classification (OPCq) instrument when classifying NI.
Background
In hospital settings in the Nordic countries, the RAFAELA system is one of the most used patient classification systems (PCS),26–30 and it is one of few that meet the criteria for validation and reliability. 31 The validity and reliability of the RAFAELA system has been tested once in primary healthcare in Finland 32 and once in HHC in Norway. 33 The overall purpose of the RAFAELA system is to ensure that the workload per nurse (expressed in NI points per nurse) is at an optimal NI level, i.e. that patients’ care needs are in balance with the available nursing resources. This ensures person-centred nursing, good patient outcomes, good working conditions and the effective use of available resources. 34
The RAFAELA system consists of the following components: 1) Daily registration of patients’ care needs using the OPCq instrument; 2) Daily registration of actual nurse staffing resources; 3) Periodical determination of optimal NI level using the Professional Assessment of Optimal Nursing Care Intensity Level (PAONCIL) instrument (at the end of each shift for a period of four to six weeks, to determine whether resources have been sufficient in relation to patients’ needs). 35
The OPCq instrument was developed at Oulu University Hospital emanating from research by the Canadian Hospital Systems Study Group (HSSG) 36 and implemented at Vasa Central Hospital in 1995. 29 The OPCq instrument is supplied by the Finnish Consulting Group (FCG) 37 and the platform is electronic. The OPCq instrument has six sub-areas: 1) Planning and co-ordination of nursing care; 2) Breathing, blood circulation and symptoms of disease; 3) Nutrition and medication; 4) Personal hygiene and secretion; 5) Activity, sleep and rest; 6) Teaching, guidance in care and follow-up care, emotional support. When using the OPCq, nurses measure the six sub-areas at regular intervals: A = 1 point describes a patient who manages relatively well on his/her own; B = 2 points describes a patient who is occasionally in need of care; C = 3 points describes a patient who needs repeat help, complex; D = 4 points describes a patient who constantly needs help, very complex. The sum provides a total NI per patient per day in hospital or per HHC visit. Total NI can thus vary from six to 24 points. Patients are classified into five categories. Category 1: 6–8 points (minimal need for care), category II: 9–12 points (average need for care), category III: 13–15 points (more than average need for care), category IV: 16–19 points (maximum need for care) and category V: 20–24 points (intensive care required).27,28,38 For further information see previous works. 39
Aim
The aim of this study was to describe nurses’ work experiences and perception of the usability of the OPCq instrument when classifying NI in HHC.
Methods
We used an explorative qualitative approach using focus-group interviews.40,41 A qualitative approach is a trustworthy way to understand nurses’ thoughts on their experiences, especially if a research topic is relatively unresearched.
Setting
This study was a part of a collaborative research project and development programme from 2012–2014 in a Norwegian municipality and included two HHC units, the municipality’s Institute for Research and Development for Nursing Care Services and a regional university college. How HHC is defined and organized differs throughout the world. 42 In Norway the municipalities are responsible for providing HHC for their inhabitants. Each municipality determines the level of HHC services provided and these are allocated via patient services offices.
The study took place in a city with approximately 70,000 inhabitants. The two HHC units managed nursing care for about 220 home-dwelling patients. While these two units provided services to all those in need of HHC services, most patients were older Norwegians. The Finnish Consulting Group (FCG) 37 supplied the RAFAELA system used in this study. Some small modifications of the OPCq instrument were necessary for the HHC setting.
Participants and data collection
Participant background characteristics.
HHC: Home healthcare; RN: registered nurse; SE: social educator; PN; practical nurse.
We divided the participants (n = 22) into homogenous groups according to educational level, with the aim of promoting interaction. Having the same level of education may make people more comfortable in sharing opinions and experiences. 41 In April 2013, six PNs participated in one focus-group interview and five RNs and one SE in a second. In May 2013, an additional six PNs participated in a third focus-group interview and four RNs in a fourth. We included the SE in the same focus group as the RNs, as the SE had an equivalent educational level. RNs and PNs often have patients with different needs, and RNs often care for patients with more and demanding care needs and have more administrative tasks than PNs.
Data were collected through focus-group interviews, equating to empirical data on a group level, with social interaction as the source of data.40,43 We also developed a semi-structured thematic guide (Figure 1).
Semi-structured thematic guide.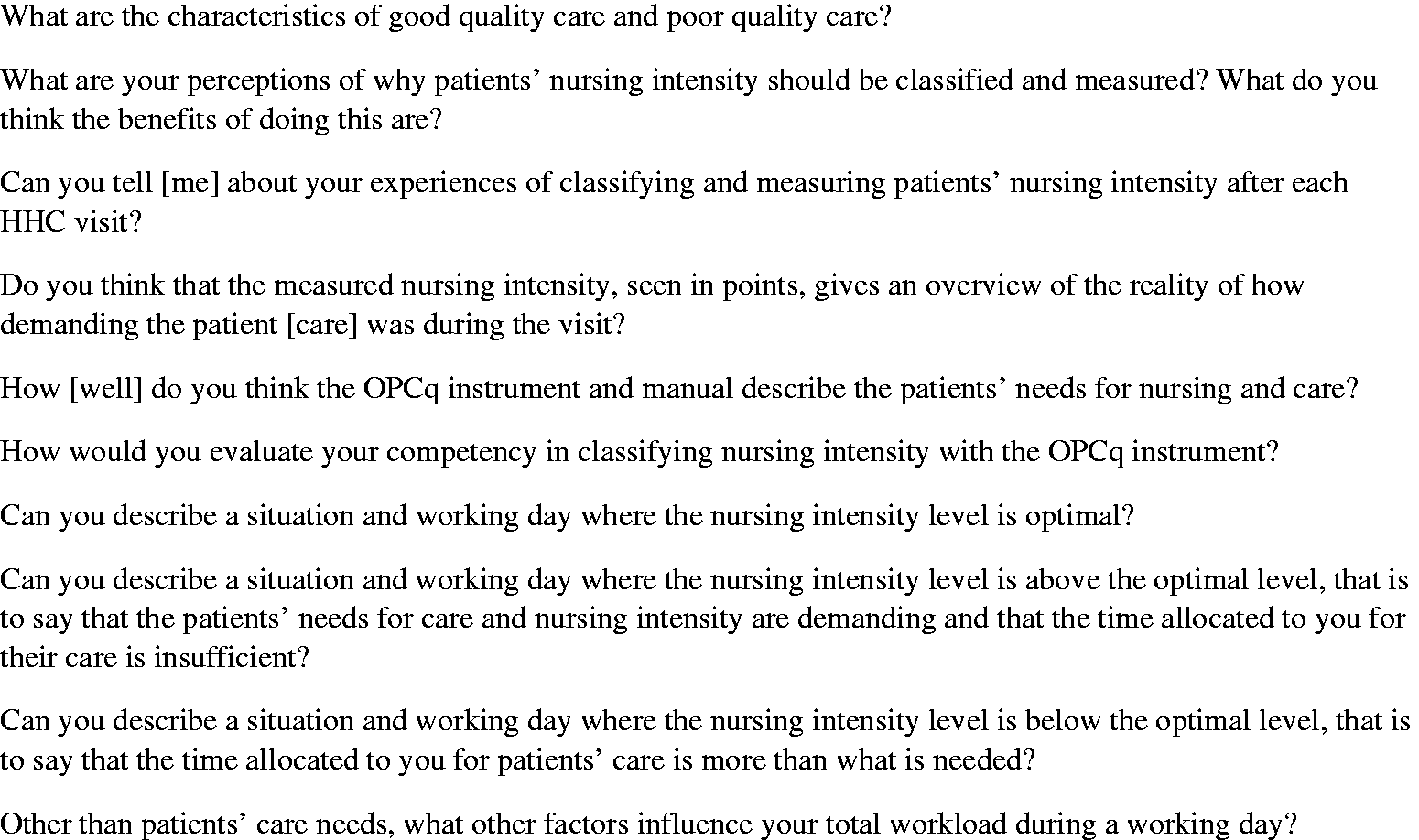
The project leader moderated all four focus-group interviews, having expertise and genuine interest in HHC and past focus-group experience. As moderator she initiated the interview, determined the topic to be discussed, followed the semi-structured thematic guide and decided when to stop the conversation. She also focused on realizing an open-minded setting where all participants could freely express themselves, and as such there were no right or wrong reflections. All focus-group interviews took place at the Institute for Research and Development for Nursing Care Services and lasted for about 60 minutes. The focus-group interviews were tape-recorded, and a research assistant transcribed the interviews verbatim.
Data analyses
Inspired by a phenomenological-hermeneutic tradition, 44 content analyses were performed in accordance with Graneheim and Lundman. 45 Content analyses are a research technique recommended for making replicable and valid inference from text. 46 There are no simple guidelines for data analysis, and results depend on several factors such as skills, insights, and analytic abilities. 47 The first author (JF) started the content analyses, with the interpretation process being carried out through reflection and discussion with the second (BL), third (ST) and fourth (LF) authors with the goal of managing shared understanding during several sessions.
The first author (JF) read all of the material from the interviews several times to garner a comprehensive understanding. Then the meaning units were highlighted. The next step was condensation, a process of shortening the meaning units while still preserving the core. Thereafter each meaning unit was sorted into a code. Then the codes were sorted into categories, the core characteristic of qualitative content analysis. A category is a grouping of content that shares a commonality. As a last step, a theme was created. Content analyses can be used in an inductive or deductive way. 44 We chose an inductive way, because there was not enough previous knowledge about the OPCq in HHC.
Ethical considerations
The Norwegian Centre for Research Data (NSD) assessed the study, and we sought appropriate permission and approval from the municipality. The municipality sought and was granted a license from the FCG to use the RAFAELA system. Participation in the study was voluntary. All participants consented to join the project and were assured that their identities would remain confidential. At the start at the interview, the moderator repeated the written information participants had previously been given about the research and clarified ethical aspects.
Findings
Codes, categories and themes.
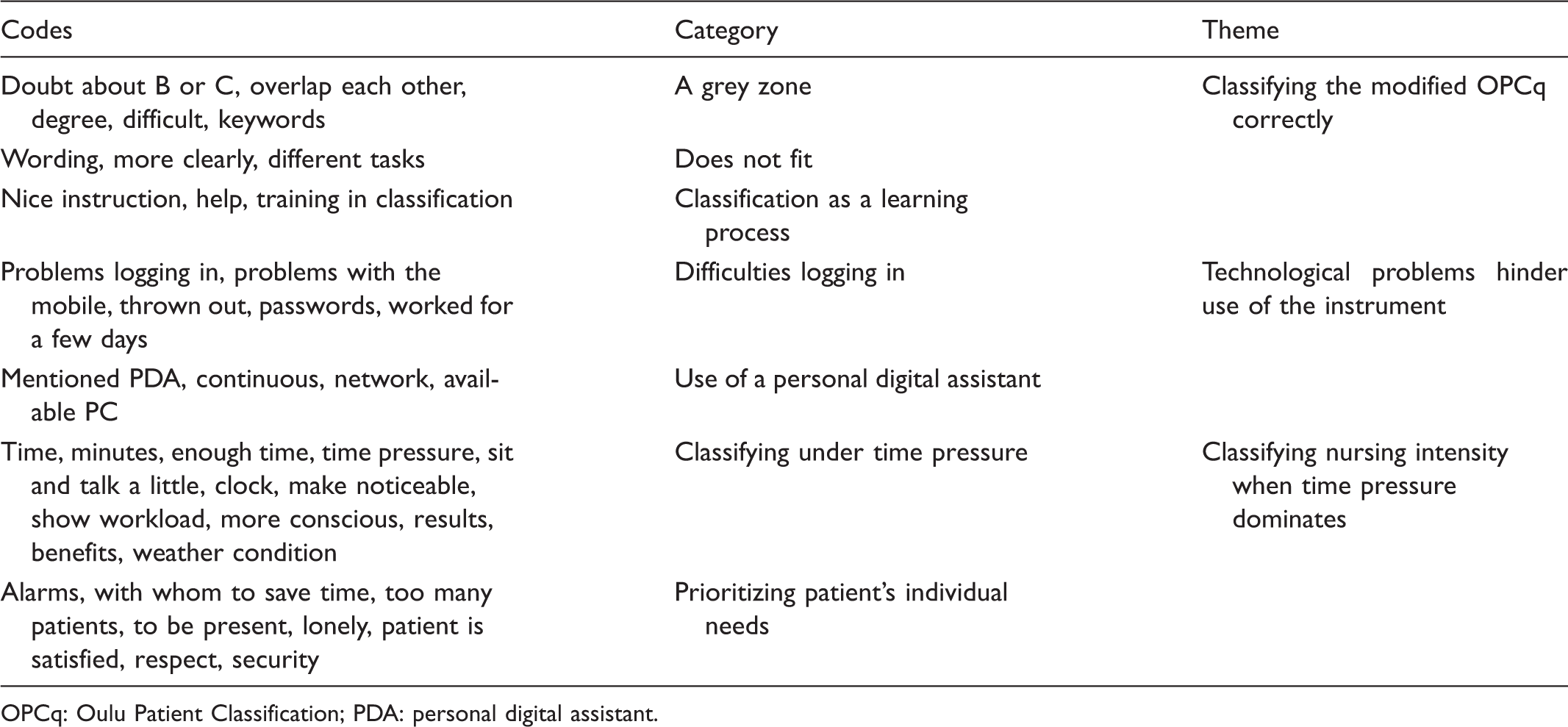
OPCq: Oulu Patient Classification; PDA: personal digital assistant.
Theme 1: Classifying the modified OPCq correctly
A grey zone
Many of the participants stated that they experienced some uncertainty about choosing between the various OPCq levels (A, B, C and D); there was a ‘grey zone’ as they expressed it, especially regarding levels B–C. If there are some changes in the [patient’s] condition, it can vary from day to day. But you must of course decide based on the condition that day, but it is difficult to distinguish between B and C then.
Does not fit
Several noted tasks or duties that they engaged in but which were not specifically listed in the OPCq. The most common example was helping patients with support stockings, and especially the RNs mentioned ‘the countless phone calls’, as they themselves expressed it. I think it’s difficult to place all the things … go to the pharmacy, take [phone calls], lots of [phone calls] with relatives, with doctors … unbelievable.
Classification as a learning process
The HHC staff were all familiar with how to use the OPCq and had participated in the pre-implementation educational programme. They noted that classifying with other nurses (joint or collective classification) helped them learn how to use the instrument and allowed them the opportunity to discuss any uncertainties. It was so that we had someone [here] one day, she just went around and asked, ‘have you documented using RAFAELA and is there anything you need?’, and that was of course very useful I think. So we sat together and classified something, like, so that I had some a-ha experiences.
Theme 2: Technological problems hinder use of the instrument
Difficulties logging in
The participants mentioned that it could sometimes be difficult to log in to the RAFAELA system due to technical problems. As one explained: … but the big problem was … to come [into the system] and log in and … but I think that as soon as [that] is done that it doesn’t take such a long time with the classification.
Use of a personal digital assistant
The majority stated that they would have preferred to register OPCq measurements using a personal digital assistant (PDA) immediately after they had visited a patient. One explained: It would have been much easier to do it continuously while you are out [working] on the [patient] list.
Theme 3: Classifying NI when time pressure dominates
Classifying under time pressure
The participants stated that a lack of time during the working day was a significant stress factor when classifying. They mentioned that they had a lot of patients on their care lists and that the OPCq could become an additional stress factor. They related that an important aspect of the care they provided was the possibility to sit down with a patient and listen or talk, even if only for a few minutes. They mentioned that they were uncomfortable when they were ‘talked out the door’, having to rush to go to the next patient. If something unexpected or unscheduled occurred, such as an acute/emergency situation or unexpected phone calls, the care that was scheduled might not be realized. One explained: Suddenly there are some phone calls on the top of what you have planned with someone who is bad/not feeling well and someone who needs to see the doctor. Like during the winter when we have to shovel snow several times in order to get inside to them.
Prioritizing patients’ individual needs
The participants noted that during an HHC visit it was important to demonstrate respect for each patient’s individual needs and desires. They maintained that good care included giving a patient a sense of security, and the variables ‘sense of security’ (peace of mind) and ‘trust’ emerged as central aspects when the participants described what good care entails. As one expressed: That you give a little of yourself then because it also creates trust and a sense of security.
Discussion
The aim of this study was to describe nurses’ work experiences and perceptions of the usability of the OPCq instrument when classifying NI in HHC. The main findings indicate that the OPCq is useful, although some adjustment might be needed to better suit an HHC setting. The participants noted constant time pressure and that they were forced to prioritize the most important care tasks, and consequently the OPCq could then become an additional stress factor.
They also mentioned technical problems, including faulty passwords, not enough computers and that personal digital assistants (PDAs) were not used. Technical solutions were found to be important in a study of the CHIRS instrument, 48 and in another study staff using the CIT instrument were required to record results on an Excel spreadsheet but found this difficult. 20 It is important that staff are knowledgeable and comfortable with the technological solutions provided.
Regarding the different levels in the OPCq, the participants expressed uncertainty and that a ‘grey zone’ existed, especially between B–C but also C–D (see previous description), even though no specifics were given. The uncertainty seen here in regard to C–D is consistent with findings from earlier studies. 32 Bing-Jonsson et al. found that RNs (Bachelor’s degree) generally demonstrated more competence than PNs (vocational degree) and assistants but that exceptions did exist, with PNs showing more competence than RNs in some areas. 49 This difference may account for PNs finding it challenging to classify patients with complex health problems. A lack of competence can be one reason why choosing between levels B–C and C–D was considered difficult, even if most of the participants here had a lot of work experience.
The participants noted that they did not know where to register such tasks as, for example, helping patients with support stockings, going to the pharmacy, taking out the garbage or taking telephone calls. Some of these are non-patient factors, and non-patient factors such as shovelling snow, which are contextual or organizational, are not included in the OPCq instrument. The OPCq is used to measure NI, and the inclusion of non-patient factors should be discussed prior to further implementation, as they are a part of the total workload in HHC. Nurse managers should be aware that non-patient factors are not measured in the OPCq instrument.
Regarding the classification learning process, the participants expressed that joint or collective classification with colleagues gave them the opportunity to discuss any uncertainties and led to an increased sense of mastery and competence, in line with a study by Hustad et al. 25 When implementing the RAFAELA system, it is important to educate users and discuss values and the meaning of good caring. 50 Systematic, continuous education and well-prepared users are essential to the implementation process. 25 These factors have been shown to be essential for the successful implementation of the RAI-HC system, used in many countries, 14 which corresponds with the findings seen here.
Frail older people in HHC need specialized nursing competence6,51 and especially after the implementation of the Coordination reform in Norway, 52 pressure on nurses in general has increased, particularly regarding time pressure and the expansion of responsibility. 6 The participants here had limited time to spend with patients and had to continuously prioritize tasks and duties related to immediate care needs, also consistent with earlier studies in HHC.7,53 According to Fagerström, the most characteristic feature of an optimal NI level is that nurses feel that they are able to respond to patients’ needs and that the time needed for nursing care exists. 54 The participants here were positive that the OPCq showed the actual NI but would have liked to have seen the results during the project, which may not have occurred because of the time it took to implement the OPCq.
For the participants it was important to show patients respect, provide a sense of security, see individual needs and be present, all in line with earlier studies. 55 Also as in earlier studies,54,56 the participants sought to provide good care and mentioned that being able to sit down and communicate with patients was important. Still, a lack of time created a barrier to good care. The RNs in this study found the number of telephone calls that they received or made disturbing, a well-known problem for RNs in HHC. 6
We found that the participants demonstrated a person-centred approach when they classified patients with the OPCq instrument. Person-centred care is underpinned by values including respect for individuals, the right to self-determination and mutual respect and understanding.57–60 We assumed that the participants, with work experience in HHC and Bachelor’s or vocational degrees, possessed the correct personal skills and competence for their jobs and we assessed that they were committed to their work. However, a person-centred approach comprises more than personal skills, competence and commitment. It also encompasses the practice context and patterns: for example shift patterns, team relationships or communication systems. 61 According to OECD health policy studies, in long-term care the need exists to use standardized assessments to plan care and allocate resources. 62
When implementing the RAFAELA system, organizational leaders should be in place to oversee the project, so that nurses know that their managers use the data and support the system. 28 Nursing leaders also need support when implementing a PCS, even more so in light of the Coordination Reform as it entails complex challenges for nursing leadership. 63
Methodological considerations
This was a small study, encompassing only two units, and further research is needed. It is important to ensure that the relationship between moderator and participants is non-hierarchical. 64 The moderator (BL) here was well known in the municipality and worked as a project leader without any management responsibility, which is a strength. A good moderator should be open-minded, respect participants and have good leadership skills, 41 all characteristics the moderator here possessed. One weakness in the study might be that only the moderator was present during the interviews; there was no supportive note-taker, as recommended. 41 We assumed a note-taker was not needed, because the discussion did not include sensitive topics, though it might have strengthened the data.
It could be a weakness that the first author (JF) did not conduct the focus-group interviews. 41 Still, there was continuous discussion with the moderator (BL) during the analysis and third (ST) and fourth (LF) authors during the interpretation of the material.
Another weakness in the study is that three participants had not used the instrument solely by themselves prior to inclusion in the study. However, we assumed they would nevertheless add valuable opinions.
The technical problems experienced during the project period may affect the results, because of the possibility that the participants focused on these problems instead of the OPCq instrument.
Conclusion
The findings from this study show the usability of the OPCq instrument. The OPCq is useful in classifying NI in HHC, although some adjustments are needed to better fit an HHC context, especially regarding levels B, C and D. There was also uncertainty about where or how to classify some non-patient factors seen in HHC. The nurses found the OPCq to be useful in illuminating their work reality, including the time pressure they experience in HHC. Despite time constraints, the nurses were aware of the individual patients’ needs and cared for each patient as a person, notwithstanding the need to prioritize tasks and duties. As seen here, when implementing a new PSC it is crucial that technological solutions work satisfactorily. In future research, it is recommended that participants should be knowledgeable and comfortable with the tool and technological solutions.
Footnotes
Acknowledgements
We thank the nurse participants for giving up their valuable time to participate in our study. We are also grateful for the head nurses’ assistance with this study.
Funding
The Norwegian Directorate of Health provided funding for this study.
Conflict of interest
The authors declare that there is no conflict of interest.