
Abstract
Some dimensions such as stigmatization have been identified in the previous literature regarding experiences of living with a sexually transmitted disease (STD). However, relatively little is known about the generic experiences of those infected. The aim of this study was to describe the experiences of living with an STD, as evaluated by those infected. Data (n = 213) were collected via an online questionnaire and analysed using statistical methods. The experiences of living with an STD varied overall. The immutability of everyday life, a thirst for knowledge, a responsible attitude towards treatment of an STD and the dilemma of disclosing the STD were considered to best describe the experiences of living with an STD. The most recently diagnosed STD and its phase were most often statistically significantly associated with the experiences. We conclude that the diversity of these experiences should be recognized in healthcare, and used in the prevention of STDs.
Background
Every year, hundreds of millions of people and their partners are affected by a sexually transmitted disease (STD). 1 STDs are contracted because of unprotected sexual encounters, and consequently are a very intimate issue. An STD invades the conscious and subconscious mind of the infected person, making it a critical element of their life. 2 On an individual level, the disease burden of STDs may vary, depending on their characteristics (curable or incurable). Chlamydia, syphilis, gonorrhoea and lymphogranuloma venereum (LGV) are STDs that can be cured with medication. In turn, viral STDs such as HIV/AIDS, human papilloma virus (HPV), herpes simplex virus (HSV) and hepatitis B and C viruses (HBV, HCV) cannot be cured, although medications can modify the disease course or symptoms.1,3
Whether the STD is curable or incurable, it poses a threat to the individual’s sexual and reproductive health,1,3,4 by causing severe human consequences such as reproductive complications (due to gonorrhoea, chlamydia), neonatal injury (due to syphilis, HSV), and in the worst case, death (due to AIDS, cervical cancer caused by HPV).1,5 In addition, the substantial psychological effects of STDs cannot be overlooked.5–7 Receiving the diagnosis is reported to be a traumatic experience. 8 Furthermore, the STD will have a negative effect on psychological wellbeing 9 and it causes daily stress, 7 anxiety and fear. 10 Thus, living with the infection can be experienced as a constant suffering. 6
In daily experiences of those infected with an STD, the perceived stigma7–9,11,12 and a lack of support8,12 are emphasized factors. A person with an STD may have a feeling of being isolated 12 and receive emotional support only from his/her peers, 6 for instance by participating in anonymous online forums. 11 In addition, the disclosure process can be experienced as frightening and the negative reactions to disclosure may have an impact on a person’s decisions about disclosing his/her STD-status in the future. 10 Furthermore, it is known that an STD has a predominantly negative effect on perceived quality of life,1,9,13,14 sexual function, 15 and sexual wellbeing.16,17
In the practice of healthcare, nurses and doctors must understand that having been diagnosed with an STD will likely have a detrimental effect on a person’s life. By providing appropriate support and information, it is possible to enhance their ability to cope with the adversity of being diagnosed with an STD.18,19 Furthermore, nurses play a critical role in educating patients about STDs, and also in screening for disease and providing treatment.5,20 It is known that nurses can improve health outcomes among people with STDs; however, they are not seen as working to their full potential.21 In addition, it is known that inconsistencies exist in the care of people living with STDs 21 and people with STDs have reported being negatively judged by healthcare professionals. 19 Thus, there is a need to explore the real needs and experiences of those who have contracted STDs, in order to improve healthcare practices6,21 and to implement a people-centred approach in prevention activities. 1
Due to a high global prevalence, STDs are considered to be a major societal problem.1,5 It should be noted that all communities are affected by STDs, albeit that significant regional, racial, ethnic, and other disparities persist, in groups such as adolescents, sex workers, men who have sex with men (MSM),1,5,22 and women being abused. 23 The WHO 1 has proposed a global health sector strategy for sexually transmitted infections 2016–2021, in which the goal is to end the STD epidemic as a major public health concern. One direction of the strategy is innovation for acceleration, where the purpose is to identify areas where there are major gaps in knowledge. 1 Although some aspects of having an STD have been identified in previous literature, relatively little is known about the experiential aspects. 18 In addition, the previous research is mainly disease-specific, and thus there is a knowledge gap in describing the generic experiences of infected persons.
Aim of the study
The aim of this study was to describe the experiences of living with an STD, as evaluated by those infected. The research questions were as follows:
How do infected persons describe their experiences of living with an STD? How are socio-demographic, STD-related factors and risky sexual behaviour associated with the experiences of living with an STD?
Methods
Sample and data collection
A purposive sample of adult Finnish people living with an STD was recruited over a six-month period from 2017 to 2018. This sampling strategy was used since the purpose was to describe the experiences of those infected with an STD in Finland, instead of aiming to generalize the results to a wider population. In addition, in Finland, there is lack of available national data on some incurable STDs such as HSV or HPV, and therefore it was not possible to determine the precise population (all infected people in Finland).24(p.258) As a third consideration, it was recognized that participants of this study were part of a so-called ‘difficult-to-reach’ population, so it was decided to implement the study as an online survey.25,26 Participants who met the criteria for inclusion in the study were: 1) adults (over 18 years old) living in Finland, 2) diagnosed with an incurable (HIV/AIDS, HPV, HSV, HBV, HCV) or a curable (chlamydia, syphilis, gonorrhoea, LGV) STD, 3) gave informed consent to participate in the study.
Recruitment for the study was conducted in Southern Finland from three university hospitals which, for instance, provide treatments for around 70% of Finnish people living with HIV (PLWH). 27 Recruitment also took place in student healthcare services (four units) in the same area. The nurses and doctors from the selected treatment providers were given instructions to recruit potential participants during STD-tests or STD-treatments. Additionally, research bulletins were placed in the waiting rooms of STD-clinics, giving information about the study as well as the website details and a QR code directing potential participants to the survey webpage. Alongside recruiting via treatment providers, the survey was advertised on social media (e.g. Facebook, Instagram, Twitter) – an approach which has been used previously in studies with difficulty-to-reach populations.26,28
Ethical considerations
The research plan was approved by the Ethics Committee of Helsinki University Hospital no. §138. Due to the sensitivity of the research topic, the following methods were used to protect the participants.26,29 Informed consent was obtained electronically in two phases. On the opening page of the survey there was a description about the study and its aims, as well as a note to participants that all possible measures would be taken to ensure the anonymity and confidentiality of their responses. The participants could proceed to the questionnaire only after declaring that they were at least 18 years old, had understood the information given, and that they were willing to participate in the study. As a second stage, participants were asked to confirm their submission of responses at the end of the survey, and given a notification to clear the page history of the web-browser if they were using a public computer. In addition, they were informed that, in the study, IP addresses could not be used to identify computers, and hence participants.25,28,30
Instrument development
Since the previous instruments related to this topic were mainly disease-specific and focused on measuring concepts such as quality of life or sexual wellbeing, a specific instrument (Experiences of living with an STD: EoLWSTD) was developed for this study. 31 The theoretical basis of the instrument has been established in previous studies considering the experiences related to living with an STD. In those studies, living with an STD has been operationalized using the experiences of becoming infected with an STD and its treatment, and the experiences of an STD in relation to everyday life, future and others.32–34 The theoretical basis of the EoLWSTD-instrument was operationalized using these constructs and a pool of items was produced. 31
An expert panel (n = 5) was set up to evaluate the content validity of the instrument.31,35 All of the experts chosen for the panel were working in the field of sexual health or infectious diseases. The experts evaluated the relevance of each item on Likert-type scale, ranging from 1 (not relevant) to 4 (highly relevant). The item-level content validity index (I-CVI) was formulated for each item by calculating the number of experts giving a rating of either 3 or 4, divided by the total number of experts. The scale-level content validity index (S-CVI/Ave) was formulated from the average of the I-CVIs for all items of the instrument. The I-CVI ranged from 0.40 to 1.00 and the S-CVI/Ave was 0.84. None of the items were excluded from the instrument, although an acceptable level of I-CVI (1.0) was not achieved with all of the items.35,36 The reason for retaining all of the items was that the instrument was in its development phase. However, the wording of 10 items was revised based on the experts’ comments. In addition, changes were made to the expressions of the socio-demographic and STD-related items, as well the items related to risky sexual behaviour.
Finally, the revised instrument was pilot-tested.37,38 However, before the pilot study was carried out, a pre-test was conducted (n = 8) to ensure the technical functionality of the online questionnaire. Based on the pre-test, two STD-related items were modified and the response instructions re-formulated. A purposive sample (n = 48) of people with a diagnosed STD infection was recruited to the pilot study from three university hospitals in Southern Finland and social media were also used to recruit participants. Otherwise, the recruitment and informing of the participants for the pilot study was conducted in a manner similar to the survey. The purpose of the pilot study was to evaluate the feasibility of the scale, the understandability of the questions, as well as the response time that was needed. The pilot study also aimed to conduct a preliminary assessment of the instrument’s internal consistency, and participants were encouraged to write their own comments regarding the layout of the questionnaire and the content of its items.37,38 Based on the results of the pilot study, there was no need to revise the instrument. Additionally, it was recognized that any decisions concerning instrument revision from a pilot study of this size should be made with caution. 37 Thus, the instrument remained unrevised, which made it possible to include the responses (n = 48) in the survey data.
Questionnaire
Socio-demographic characteristics and risky sexual behaviour of the study participants (n = 213).
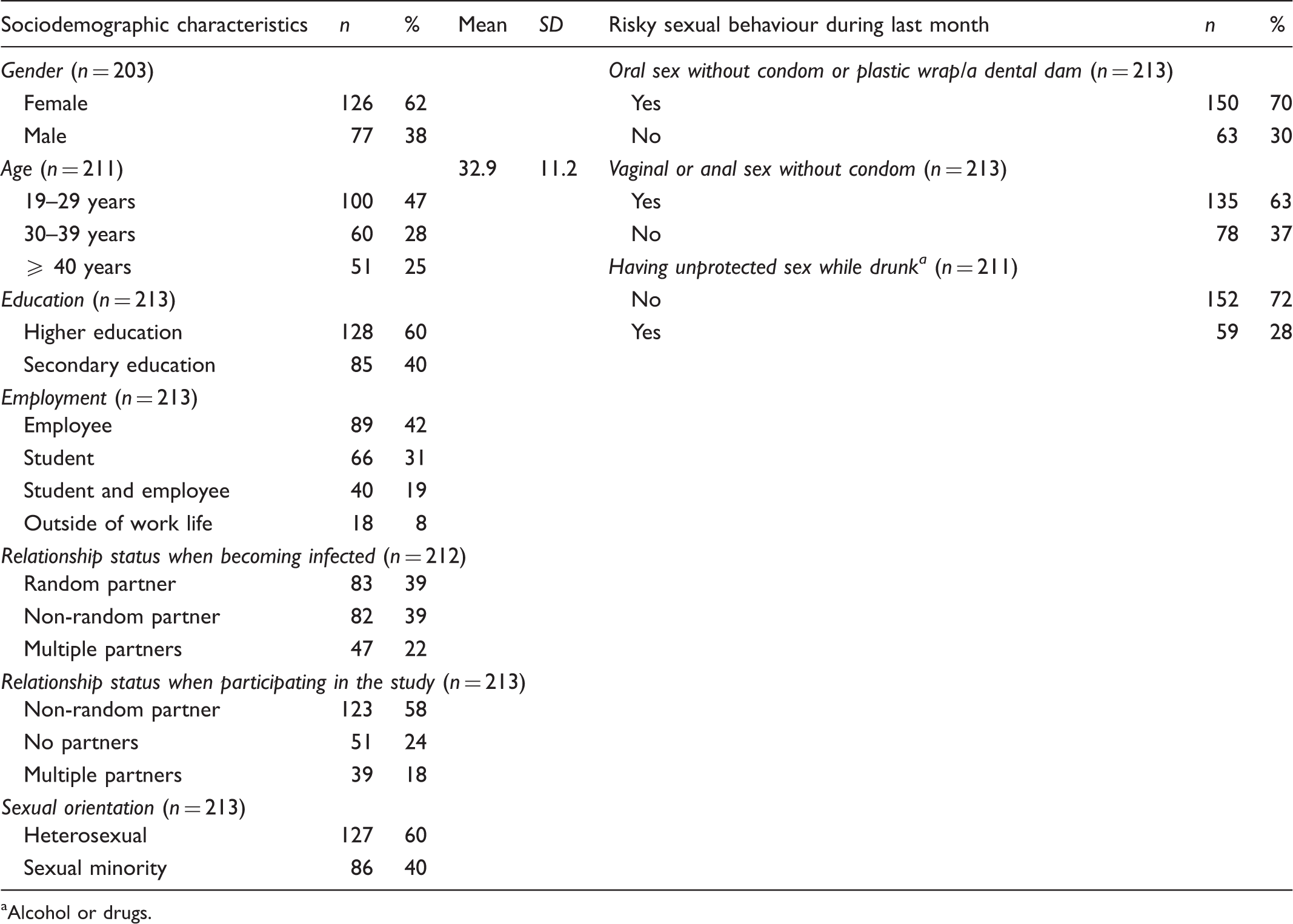
Alcohol or drugs.
STD-related characteristics of the study participants (n = 213).
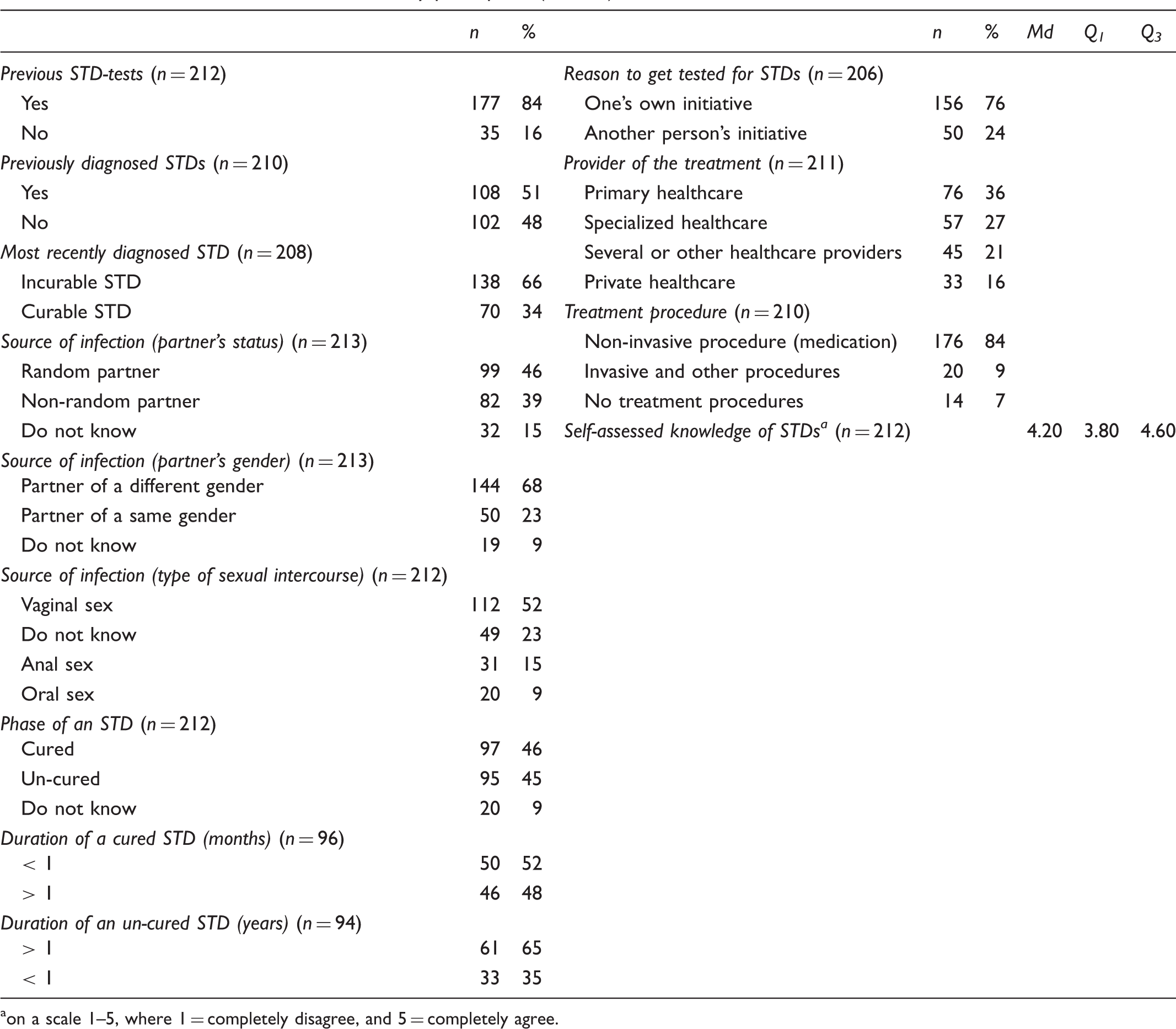
on a scale 1–5, where 1 = completely disagree, and 5 = completely agree.
Descriptive statistics and reliability of EoLWSTD-instrument and its sub-dimensions (n = 213).
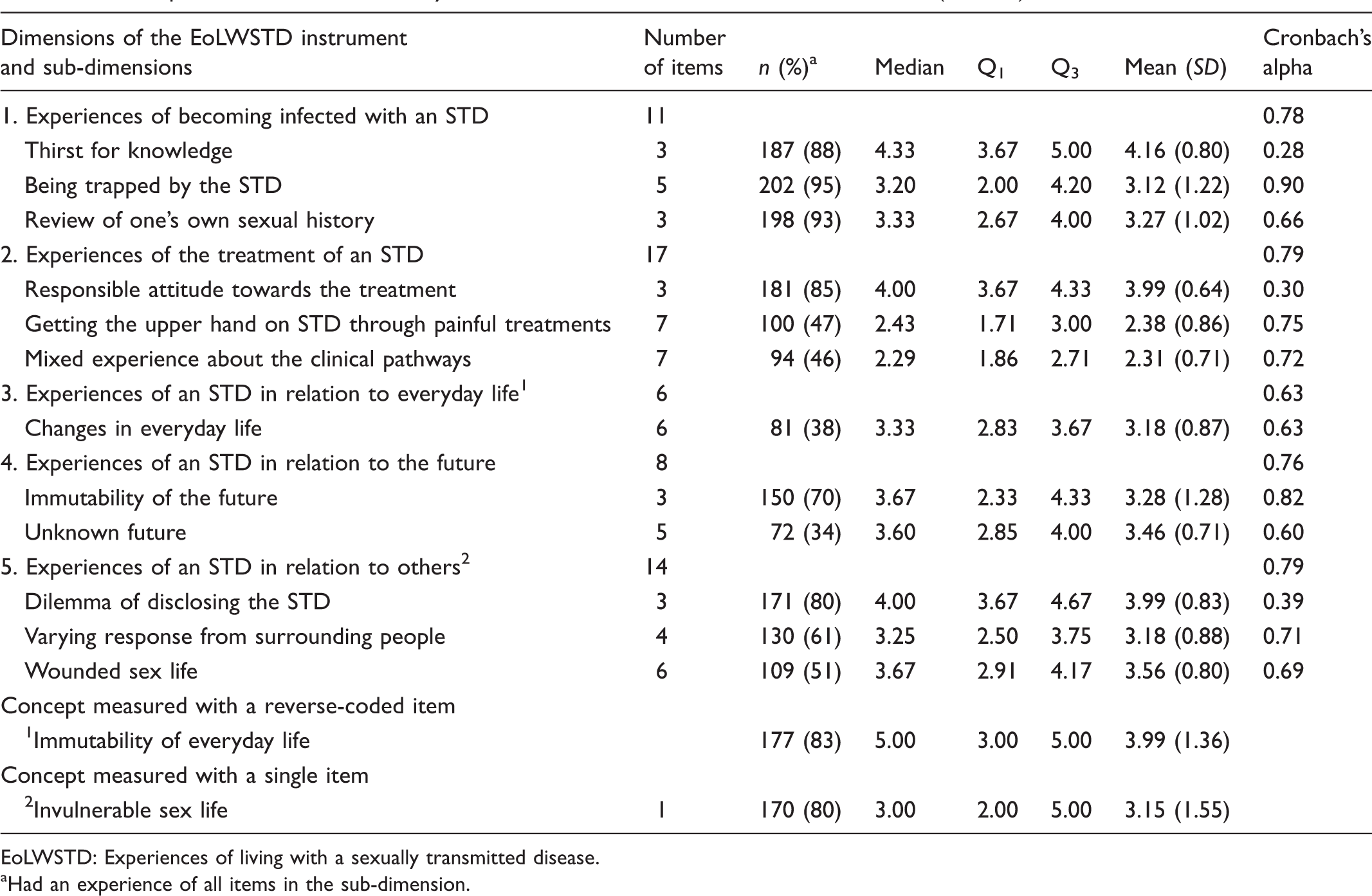
EoLWSTD: Experiences of living with a sexually transmitted disease.
Had an experience of all items in the sub-dimension.
The EoLWSTD-instrument has five dimensions. The first dimension explores experiences related to becoming infected with an STD (11 items). The second dimension explores experiences related to treatment of an STD (17 items). The third dimension explores experiences related to everyday life with an STD (6 items). The fourth dimension explores experiences related to the future with an STD (8 items), and the fifth dimension explores experiences the infected person has in relation to others (14 items). Each dimension contained sub-dimensions which were formed according to the theoretical basis of the instrument. Each item was Likert-scaled, ranging from 1 (completely disagree) to 5 (completely agree), which indicated how the items described participants’ experiences of living with an STD. The option of 0 (not applicable to me) was also included in the scales.
The socio-demographic items included gender, age, education, employment, relationship status (when becoming infected and when participating in the study) and sexual orientation. The STD-related items were measured two-fold. Firstly, the participant was asked about his/her previous STD-tests and previously diagnosed STDs. Secondly, the participant was asked questions related to their most recently diagnosed STD: diagnosed STD, source of infection (non-random/random partner, gender of the partner, type of sexual intercourse), reason to get tested for STDs, phase of the STD, duration of the STD (cured/un-cured STD), provider of the treatment and treatment procedure. In addition, the participant’s self-assessed knowledge of STDs was assessed using statements regarding STD transmission, symptoms, treatments, complications and prevention methods. The statements were in a five-point Likert form. Risky sexual behaviour during the previous month was measured using questions about having unprotected oral, vaginal or anal sex, or having unprotected sex while drunk.
Data analysis
A total of 227 people answered the online questionnaire. Fourteen responses were excluded from the analysis because either the informed consent was not obtained or data were missing for more than half of the items. Descriptive analysis was conducted using data stemming from 213 people with an STD. The data were analysed using the Statistical Package for Social Science (SPSS version 24), and the level of statistical significance was set at p < 0.05.24(pp.319–353)
Some socio-demographic items were re-categorized for the analysis. The age of participants was grouped as: 19–29 years, 30–39 years and ≥ 40 years. The education level of participants was grouped into two groups: higher education (university, college degree or PhD) and secondary education (high school, professional degree or compulsory degree). Employment status was modified into four groups: employee, student, student and employee, and outside of work life (retired, maternity, parental leave, or other). Relationship status when becoming infected was grouped as: random partner, non-random partner, and multiple partners (non-random and random partner or other). Relationship status when participating in the study was grouped as: non-random partner, no partners, and multiple partners (random partner, non-random and random partner, other). Sexual orientation was divided into two groups: heterosexual and sexual minority (homo- or bisexual, asexual, do not want to define, or other).
Some of the STD-related items were also re-categorized for the analysis. Participants’ most recently diagnosed STDs were grouped into two groups: incurable STD (HIV/AIDS, HPV, HSV, HCV) and curable STD (chlamydia, syphilis, gonorrhoea). The duration of a cured STD was modified as: < 1 month (days, weeks), and > 1 month (months, years). The duration of an un-cured STD was grouped as: > 1 year (years), and < 1 year (days, weeks, months). The reason to get tested for STDs was divided into two groups: one’s own initiative (symptoms, unprotected sexual intercourse, regular STD-tests) and another persons’ initiative (partner notification, healthcare professional’s suggestion, or screening for STDs alongside another treatment). The treatment providers were grouped as: primary healthcare (health centre, student healthcare), specialized healthcare (venereal diseases outpatient clinic or infectious diseases clinic), private healthcare, and several or other healthcare providers. The treatment procedure of an STD was modified into groups addressing non-invasive procedures (medication: tablet, cream, injection), invasive and other procedures (surgery, cryo-, laser therapy, others), and no treatment. Additionally, a sum score variable was created based on five items regarding self-assessed knowledge of STDs.
Firstly, when analysing participants’ experiences of living with an STD, the items were dichotomized (Likert 1–5 = experience exists vs. Likert 0 (not applicable to me) = experience does not exist). The purpose of this was to investigate whether the participants had experiences that were addressed by the EoLWSTD-instrument. Frequencies and percentages were calculated for those who had an experience of all of the sub-dimension items. Secondly, the option 0 was coded as a missing value for further analysis, and sum score variables (ranging from 1 to 5) were calculated for each sub-dimension. The experiences of living with an STD were then analysed using medians (Md), quartiles (Q1, Q3), means (M) and standard deviations (SD). Since the sub-dimensions of the EoLWSTD-instrument did not meet the assumption of normality, Kruskal–Wallis tests, Mann–Whitney U tests and Spearman correlation coefficients were used to analyse factors associated with the experiences of living with an STD.24(pp.319–353) Moreover, in order to evaluate the internal consistency of the dimensions and sub-dimensions of the EoLWSTD-instrument, Cronbach’s alfa coefficients (α) were separately calculated for each dimension and sub-dimension.24(p.323)
Results
Sample description
Of the participants, 62% were female. The average age of participants was 32.9 years (SD = 11.2). Most of the participants (60%) had a higher education level, and almost half (42%) reported themselves as being employees. Relationship status when becoming infected with the most recent STD was with a random partner (39% of cases), whereas at the time of participating in the study the most common relationship status was with a non-random partner (58% of cases). Most of the participants (60%) reported their sexual orientation as heterosexual. Of the participants, 70% reported risky sexual behaviour during the last month by having oral sex without a condom or plastic wrap/dental dam, and most (63%) reported having vaginal or anal sex without condom. Less than one third of the participants (28%) reported having unprotected sex while drunk (Table 1).
Of the participants, 84% reported having had a previous STD-test, and over half (51%) had been previously diagnosed with an STD. Most of the participants (66%) had most recently been diagnosed with an incurable STD. The source of infection was a random partner in 46% of cases and a partner of a different gender in 68% of cases. Over half of the participants (52%) reported having contracted an STD through vaginal sex, and almost half (46%) reported their STD as having been cured at the time of survey. The duration of a cured STD was less than a month in 52% of cases, whereas with un-cured STD the duration was more than a year in 65% of cases. Most of the participants (76%) reported that the reason for getting tested for STDs was on their own initiative. Primary healthcare was the treatment provider for STDs in 36% of cases, and non-invasive procedures (medication) were used as treatment in 84% of cases. The participants’ self-assessed knowledge of STDs was high (Md = 4.20, Q1 = 3.80, Q3 = 4.60) (Table 2).
Experiences of living with an STD
The experiences of living with an STD varied. Participants had most experiences in terms of becoming infected with an STD: being trapped by the STD (n = 202, 95%) and reviewing of one’s own sexual history (n = 198, 93%). In contrast, participants expressed fewest STD-related experiences in relation to their future: unknown future (n = 72, 34%) and in relation to their everyday life: changes in everyday life (n = 81, 38%) (Table 3).
Immutability of everyday life (Md = 5.00, Q1 = 3.00, Q3 = 5.00), thirst for knowledge (Md = 4.33, Q1 = 3.67, Q3 = 5.00), responsible attitude towards the treatment (Md = 4.00, Q1 = 3.67, Q3 = 4.33) and the dilemma of disclosing the STD (Md = 4.00, Q1 = 3.67, Q3 = 4.67) had the three highest ratings. Thus, these experiences were considered as best describing the experiences of living with an STD. In turn, mixed experiences about the clinical pathways (Md = 2.29, Q1 = 1.86, Q3 = 2.71), getting the upper hand on STD through painful treatments (Md = 2.43, Q1 = 1.71, Q3 = 3.00) and invulnerable sex life (Md = 3.00, Q1 = 2.00, Q3 = 5.00) had the three lowest ratings. Hence, these experiences were considered as worst describing the experiences of living with an STD (Table 3).
Factors associated with the experiences of living with an STD
Most recently diagnosed STD and its phase, participants’ age and previously diagnosed STDs were most often statistically significantly associated with the experiences of living with an STD. In contrast, relationship status when participating in the study, having unprotected oral sex, having unprotected sex while drunk, or the duration of an un-cured STD had no statistically significant associations with the experiences of living with an STD (online supplementary material: Tables 1–4). The factors which were most often statistically significantly associated with the experiences of living with an STD are described in more detail in the following paragraphs.
Participants who had recently been diagnosed with an incurable STD had statistically significantly higher evaluations on the following experiences: thirst for knowledge (p = 0.001), being trapped by the STD (p = 0.001), getting the upper hand on STD through painful treatments (p = 0.003), changes in everyday life (p = 0.002), unknown future (p = 0.025) and wounded sex life (p = 0.001), compared with those with a curable STD. Participants who had recently been diagnosed with a curable STD had statistically significantly higher evaluations regarding a responsible attitude towards the treatment (p = 0.001), immutability of everyday life (p = 0.001) and the future (p = 0.048), the varying response from surrounding people (p = 0.009) and an invulnerable sex life (p = 0.007), compared with those with an incurable STD (online supplementary material: Tables 1–4).
The phase of an STD (most recently diagnosed) had statistically significant associations with the following experiences: thirst for knowledge (p = 0.023), being trapped by the STD (p = 0.001), responsible attitude towards the treatment (p = 0.001), getting the upper hand on STD through painful treatments (p = 0.004), immutability of everyday life (p = 0.001), changes in everyday life (p = 0.001), immutability of the future (p = 0.001), unknown future (p = 0.002), varying response from surrounding people (p = 0.001), wounded sex life (p = 0.001) and invulnerable sex life (p = 0.001). For instance, a thirst for knowledge was evaluated highest among participants with an un-cured STD (n = 81), but lowest among participants with a cured STD (n = 87). Moreover, a responsible attitude towards treatment was rated highest in the group with a cured STD (n = 76), but lowest in the group with an un-cured STD (n = 87). Immutability of everyday life was rated highest among participants with a cured STD (n = 69), but lowest among participants with an un-cured STD (n = 90) and those who did not know the phase of an STD (n = 17). In contrast, changes in everyday life were evaluated highest among participants with an un-cured STD (n = 55), but lowest among participants with a cured STD (n = 16) (online supplementary material: Tables 1–4).
The participants’ age were statistically significantly associated with the following experiences: getting the upper hand on STD through painful treatments (p = 0.003), mixed experience about clinical pathways (p = 0.003), changes in everyday life (p = 0.001), immutability of the future (p = 0.007), varying response from surrounding people (p = 0.001), wounded sex life (p = 0.035) and invulnerable sex life (p = 0.004). In addition, having been previously diagnosed with an STD was statistically significantly associated with higher evaluations relating to a responsible attitude towards treatment (p = 0.022), immutability of the future (p = 0.006), varying response from surrounding people (p = 0.011) and invulnerable sex life (p = 0.000). However, having not having been previously diagnosed with an STD was associated with experiencing one’s sex life as being more wounded (p = 0.023) (online supplementary material: Tables 1–4).
Discussion
Based on the results of this study, experiences of living with an STD have varying evaluations. Firstly, experiences reflect responsibility in terms of the treatment of an STD and the constancy of everyday living. Secondly, experiences reflect some kind of uncertainty, such as a thirst for knowledge and a dilemma of disclosing the STD. The results of this study are mostly consistent with those of previous studies, although there is a difficulty in comparing results of this current study to other studies because the topic has not been previously investigated from this perspective.
In addition to being responsible in terms of the treatment of an STD, responsibility was also reflected in relation to STD-tests. The majority of participants in this study had previously taken STD-tests and were seeking them based on their own initiative. This result is concurrent with a previous study in which regular STD-testing was perceived as a responsible behaviour. 39 However, Christianson et al. described men as having mixed emotions around STD-testing which manifested as either a willingness or unwillingness to be tested. 40 In this present study, the method of STD-testing was not explored. However, previous studies have pointed out the importance of developing confidential, convenient 39 and easily accessible STD-testing services, and internet-based chlamydia testing service has proved to be effective in reaching at-risk groups. 41
The results of this present study differ from previous studies in terms of experiencing the immutability of everyday life. For instance, previous studies have reported that PLWH experience everyday stress 7 and constant suffering related to their condition. 6 Also, it has been described that receiving an HIV diagnosis will cause a change of direction in life which is manifested as the life before and the life after HIV.6,42 Experiences of the immutability of everyday life reported in this study may be explained by the fact that there were less recent infections among the participants. Also, the prognosis of the most recently diagnosed STD (as curable/incurable) and its phase were statistically significantly associated with the experiences of STD in relation to everyday life. In particular, previous studies have emphasized the importance of managing the emotional impact of the STD 42 and psychological adjustment for those living with an incurable STD.6,9 In turn, East et al. have also reported on the phenomenon where women living with an STD were minimizing the extent of their infections to preserve their integrity. 18
Participants assessed their knowledge of STDs as high in this study, and this was statistically significantly associated with a responsible attitude towards treatment, getting the upper hand on STD through painful treatments, and the immutability of the future. Despite this, however, a thirst for knowledge was also rated as high when describing the experiences of living with an STD. In this context, a thirst for knowledge refers to a need to know one’s own STD-status and source of the infection, as well as needing to know more about the STD. 32 However, it is possible that the high level of self-assessed knowledge of STDs reported in this study could actually be an outcome from a thirst for knowledge. This can be confirmed by previous studies which instead have reported low levels of knowledge and awareness of STDs among people without infection.43,44 From the perspective of the prevention of STDs, it is known that focus should be placed on fostering an increasing awareness of STDs at a community level, and when awareness is strengthened within the community, then the use of STD-related healthcare services tends to improve. 1
In this study, participants reported that they experienced a relatively difficult dilemma associated with telling other people about their STD, and in a way, this reflects stigmatization. STD-related stigma is a well-known phenomenon acknowledged in previous literature.1,10,45 Thus, the results of this present study are concurrent with previous findings. However, this study revealed factors associated with the dilemma of disclosing the STD which involved risky sexual behaviour (vaginal or anal sex without a condom) and the source of infection (partner’s gender and type of sexual intercourse). Relatedly, STDs have been associated throughout history with deviant immoral sexual behaviour and a study by East et al. 45 explored this relationship between stigma and stereotypes in the context of STDs. Their study revealed that women with STDs had a profound stigma attached to them, so they internalized the stereotypical views on people with STDs and carried those thoughts about themselves. 45 This can explain why, in this study, risky sexual behaviour and the source of infection were linked to the dilemma of disclosing the infection.
Methodological considerations
The present study had several strengths. To the best of our knowledge, the current topic has not been previously investigated in terms of generic experiences of infected persons, which was explored in this study using a cross-sectional survey method. As such, this study provides a new approach through which to conduct research on the experiences of infected persons. In addition, the present study encompasses the viewpoints of those living with both incurable and curable STDs.
However, the present study had some limitations that should be discussed. Firstly, the instrument used has not previously been validated, although it was shown to have fairly good psychometric properties in terms of internal consistency. Cronbach’s alpha coefficients (α) for most dimensions of the EoLWSTD instrument were considered as good (α ≥ 0.70) (Table 3), although one dimension (experiences of an STD in relation to everyday life α = 0.63) had lower α value than expected.31,35 The internal consistency of the sub-dimensions of the instrument was considered as being sufficient (α ≥ 0.60), despite a few poor α values (thirst for knowledge α = 0.28, responsible attitude towards treatment α = 0.30, dilemma of disclosing the STD α = 0.39). 46 Based on these preliminary results, it is clear that the instrument will need to be further validated in the future.
Secondly, the interpretation and generalization of these results must be undertaken with caution since the sampling strategy was purposive and the sample size (n = 213) was relatively small. As a third consideration, participation in this study was based on self-reported STD-status which can be considered as a limitation. For instance, the majority of participants reported having been most recently diagnosed with an incurable STD (n = 138, 66%), however, almost half of the participants (n = 97, 46%) also reported that their most recently diagnosed STD had been cured at the time of participating in the study. This may be explained by the fact that some STDs, such as HSV and HPV, are not cured although the visible lesions on the skin or mucous membrane have disappeared. 5 Therefore, participants in this study may have thought that their incurable STD was cured. Despite its limitations, the results of the study provide a good base for further research to be continued.
Conclusions
We conclude that experiences of living with an STD as evaluated by those infected are various. The prognosis of the most recently diagnosed STD and its phase are seen to be the strongest factors determining the experience. Therefore, the diversity of generic experiences of infected persons should be identified and taken into consideration when developing healthcare and prevention practices. For instance, it would be beneficial to produce support interventions for those infected with an STD and educational interventions for healthcare personnel involving the care of those infected.
The feeling of responsibility which infected people have should be recognized as a part of any treatment and prevention activities. Thus, policy makers should promote the accessibility of STD-testing in order to break the chain of infections. Also, it is crucial to continue developing internet-based STD-tests and to ensure that evidence-based and comprehensible information relating to the experiences of living with an STD is available in online health services. Moreover, at a community-level it should be emphasized how common these infections are, in order to reduce the stigma attached to these conditions.
Given that this study was the first to describe the generic experiences of infected people, it is clear that additional research is needed. The experiences of infected persons should be measured with larger populations and employ different sampling strategies. In addition, it is up to further research to determine whether the EoLWSTD-instrument calls for a modification to be more sensitive with measuring these generic experiences of people with different STDs.
Supplemental Material
Supplemental material for Experiences of living with a sexually transmitted disease: A cross-sectional descriptive survey
Supplementary Material for Experiences of living with a sexually transmitted disease: A cross-sectional descriptive survey by Toni Haapa, Tarja Suominen, Anna-Maija Koivisto and Jari Kylmä in Nordic Journal of Nursing Research
Footnotes
Acknowledgement
We would like to thank the healthcare professionals who recruited potential participants for their valuable contributions to the research. We would also like to thank all of the respondents who participated in the study.
Funding
This research was partly funded by the Sukupuolitautien Vastustamisyhdistys (Association for the Prevention of Sexually Transmitted Diseases), and the University of Tampere, Faculty of Social Sciences, Health Sciences.
Conflict of interest
The authors declare that there is no conflict of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.