
Abstract
The complexity of end-of-life communications has previously been described and found to be given late in the patient’s palliative care. There is a need for earlier and more continuous end-of-life-communications throughout the patient’s care to reduce anxiety, confusion, and promote participation. Registered nurses (RNs) have a unique closeness to the patient and the ability to identify early the need for end-of-life communication. The aim of this study was to describe crucial aspects of nursing in end-of-life communication in an oncology context. The study was designed as a qualitative content analysis of in-depth interviews with RNs working in oncology in-patient care units. Two domains were identified: before, and after end-of-life communications, with the categories importance of being well prepared to identify both the patient’s and their family’s needs. Cooperation and interaction between physicians and RNs were crucial to be able to support patients and their relatives around the clock. The presence of RNs encouraged further conversations about the patients’ conditions to gain insight into the new situation. End-of-life communication should not only be medicine oriented and performed by physicians. Involvement of RNs’ expertise enables increased patient/relative participation as well as reduced anxiety and suffering, creating clarity and safety for all involved in care.
Introduction
Oncology care is a multidisciplinary challenge where representatives from different specialties are of equal importance for the patient in need of palliative care and treatment. During the last decade, oncology treatment and care have tended to continue longer into disease progression, even if the patient is palliative.1,2 The National Board of Health and Welfare in Sweden 3 recommend that when curative treatment is no longer an alternative, an active decision to initiate palliative care must be made. Ågren Bolmsjö, Nilstun and Löfmark 4 define end-of-life communication as a communication about the content, orientation and goal of the care with the patient, and is also used as an administrative tool between different professions involved in the care. The Swedish national care program for palliative care defines end-of-life communication as a communication between the responsible physician, the patient and their relatives when decisions are made about transferring the patient to palliative care at the end of life. 3 This communication can be stressful and challenging for both the patient and their relatives, and flaws in communication can cause unnecessary anxiety.5,6 In Sweden, nurses can initiate this communication with the patient although they usually have a discussion with the physician or the team beforehand to ensure that all team-members have the same level of understanding. This study focuses on registered nurses’ experiences, role and possibilities within the process of end-of-life communication in oncology care.
Background
The transition to end-of-life care is a complex process. Many aspects need to be taken into account which are discussed more or less openly between the physician, the nursing team and the patient. 4 Swedish law gives every patient the right to receive continuous and adequate information about their disease and available methods for screening, care and treatment. 7 The National Board of Health and Welfare 3 stresses conversations about the content of patient care and direction, and that so-called end-of-life communication should be offered continuously to avoid anxiety or misunderstandings and to promote participation. The responsible physician or the patient can choose not to continue with the curative treatment and instead be transferred to end-of-life care. 8 Recent statistics imply that re-admissions to hospital of cancer patients are common in Sweden and that patients do not receive adequate information regarding their palliative situation. 3 The same phenomenon has also been described in a study from Canada. 1
In oncology care, communication is considered a core factor when the aim is to inform patients about their disease and treatment 5 and when changes in care and treatment are considered necessary.9,10 According to previous research, end-of-life communication with patients in an end-of-life stage often occurs too late in the process.11–13 Patients and their relatives therefore risk exposure to unnecessary suffering and losing valuable quality time at the end of life. This loss of time my affect the time relatives and patients have to plan their last moments together. 2 Although there is a consensus that communication between patients, relatives and health professionals is an important component for high-quality care, studies show that end-of-life communication is rare in many hospitals.2,11,13 Documentation in patient records is often insufficient and performed too late in the palliative care process.2,14 There are studies which suggest that the reasons for delays in having these conversations are an unwillingness among the patients and/or their relatives to accept the prognosis and worsening status, as well as an unwillingness among physicians to discuss the prognosis with their patients and relatives. 15
End-of-life communication within the oncological context has often focused on medical issues, e.g. reducing tumors. Heming and Colmer 8 show that nurses are more likely than physicians to initiate communication about end-of-life care, and to do it earlier and more often, with both the patient and the nursing team. End-of-life communication is considered to be important for both the patient and their relatives, giving them insight into the disease and thereby a chance to plan their time together. 2 The patient is entitled to the same information as the rest of the team involved in their care. 4 Recent research shows that when patients, for different reasons, do not want to discuss their disease and want to protect their relatives from information, this is perceived by the staff as an obstacle for communication. 6 The need for honest and individualized information to patients and relatives about the disease and the prognosis is the same for all diseases.10,14,15 However, recent research shows that appropriate information offered at the right time is a key factor for the patient’s ability to accept the new orientation of care. 16
Healthcare professionals experience uncertainties about when to transfer patients to end-of-life care and about communication between staff, patients and relatives. Hence education in how to communicate palliative care needs to be improved. 6 Because nurses are the ones who work most closely with the patient, patients often turn to them for more information.16,17 Nurses can also repeat and explain information given by physicians to patients and have the role of supporting and advocate the patient’s needs and/or wishes.18,19 Traditionally, physicians inform patients about any deterioration, although nurses are becoming more and more important in these conversations. 8 Patient records often fail to identify who has taken the initiative to begin end-of-life communication, although studies show that this is often initiated by nurses without them clarifying it in the documents.6,13 Healthcare staff including physicians, nurses and other professions, consider end-of-life communication important for both patients and relatives so that they know what to expect of the disease process. 20 Communication strategies will provide a foundation for qualitative care planning and have the potential to impact patient outcomes as well as inform about the need for healthcare resourses. 21 Nursing staff also often find this type of conversation important in order to be able to fully support both the patient and their relatives. 8
Most nurses consider end-of-life-care as a responsibility that comes with the profession 22 and conversations about existential issues are often central in caring relations with patients in this type of situation. 23 Having the courage to be present and confirm the conversation is important, as well as having time, without trying to solve the patients’ existential problems. 23 Aspects of time and meeting worried relatives who lack acceptance of a bad prognosis are experienced as obstacles for providing good end-of-life care. 24
Travelbee’s nursing theory 25 presents communication as one of the components for achieving a caring relationship. The theory is considered as a tool for understanding and meeting patients’ needs and helping them to master illness, suffering and alienation. Communication is generally understood as a mediating process of communicating thoughts and feelings. Nursing is specifically as an interpersonal process where the nurse helps the patient to promote and master experiences and find meaning in illness and suffering. With knowledge about the stress that comes with illness, dealing with suffering, alienation and death, the nurse has tools to meet the demands of nursing. Communication and conversations are the nurse’s most important tools and a precondition for reaching the goals of care.
It seems that end-of-life communication is not always considered as a step in the transition of the palliative process but as a one-time event that takes place too late in the patient’s life. Studies illuminating nurses’ experiences of end-of-life communication with patients in oncology care are sparse. Such studies could increase the awareness and development of caring strategies of this group of patients. Therefore the purpose of this study was to describe crucial aspects of nursing within the process of end-of-life communication in an oncological context.
Methods
The study has a qualitative descriptive explorative design consisting of in-depth interviews analyzed with qualitative content analysis. 26 This method is suitable to explore patterns in interviews and to describe the characteristics as well as to explore phenomena that are not well understood. 27 The method is also applicable for different kinds of texts with different levels of interpretation and could serve as a tool for analysis with varying levels of complexity. 26
Setting and sample
The study was conducted in an oncology in-patient ward at a university hospital in a large city in Sweden where active tumor treatment takes place using both cytostatic treatment and radiotherapy in curative and palliative stages. To obtain descriptions that were as rich as possible, a strategic sample of registered nurses (RNs) was used. Inclusion criteria were clinically active within oncology care, with at least one year of experience on the ward as an RN and with experience of actively taking part in at least one end-of life-communication. After permission from the head nurse and the chief executive officer, the possible informants received an invitation in writing to participate. The letter contained information about the study, clarified that participation was voluntary and explained that data would be collected and handled confidentially. Ten RNs chose to participate, and the interviews took place during the RNs’ working hours in a silent room connected to the hospital ward.
The RNs’ median age was 35 years. Number of years in the profession ranged from 2 to 27 years. Experience of specialized oncology practice varied between three months and 27 years. Five of the ten RNs also had experience of more general palliative care when nursing patients with different diagnoses.
Data collection
Data collection was conducted throughout using audio-taped in-depth interviews with open questions, from spring 2014 to spring 2016. An interview guide was used to ensure that the questions were connected to the aim of the study although the informants were encouraged to narrate freely, using their own words about their experience of end-of-life communications. A pilot interview with one RN working in oncology care, not noted or included as a participant in this study, was conducted to ensure that the interview guide was consistent. The interviews were labeled with numbers and transcribed verbatim by the first and second authors.
Data analysis
In this study we perform an inductive content analysis. This is claimed by Elo and Kyngas 26 as useful when earlier research on the topic is rather fragmented. The content analysis processes are represented as three main phases: preparation, organizing and reporting. 26
Preparation
A qualitative content analysis according to the descriptions of Graneheim and Lundman27,28 was used, since the intention was to study and describe the visible content in the text. Interpretation within manifest content analysis can be performed at varying levels and qualitative content aims to seek the meaning of every part of the text. All interviews included in the study are to be seen as a unit of analysis.
Organizing
The analysis was performed in several steps. First the transcribed material was read as a whole to achieve a basic understanding of the content as a whole. Early in the analysis process three domains could be identified in the text: before, during and after end-of-life communication. Domains are big blocks of the text, possible to identify with a low level of interpretation and can contain a bigger section of text that focuses on different parts/periods of people’s lives. After that, the meaning units were identified as words and sentences that applied to the content, and context was broken into meaning units by the authors. The meaning units were condensed and labeled with different words that worked as codes at a low level of abstraction without losing the content of the text. After reading and understanding the codes, they were sorted into preliminary categories representing similarities and differences in content. During this last phase one theme was formulated based on an interpretation of the common meaning in the text as a whole.
Ethical considerations
The demands of confidentially were considered by holding all data safe and locked away so that no information could be accessed by unauthorized persons and no data could be used for commercial purposes. The RNs invited to participate in the study were not in any way dependent on or related to the researchers. Every citation used by the authors was authorized by the RNs. Further ethical aspects were considered based on the World Medical Association Declaration of Helsinki. 29
Results
Reporting
The analysis resulted in the overall theme Clarity in care including three domains; Before, during and after end-of-life communication, consisting of two categories each, describing crucial aspects of nursing within the process of end-of-life communication.
Clarity in care
The theme Clarity in care that emerged from the RNs’ experiences of end-of-life communication illustrates that all professions need to bring clarity to the overall care of the patient so that all professions involved in the care professions, the patient and their relatives are connected in an overall flow aiming at the patient’s well-being. Figure 1 depicts the overall flow in the end-of-life communication process.
The overall flow in the end-of-life communication process.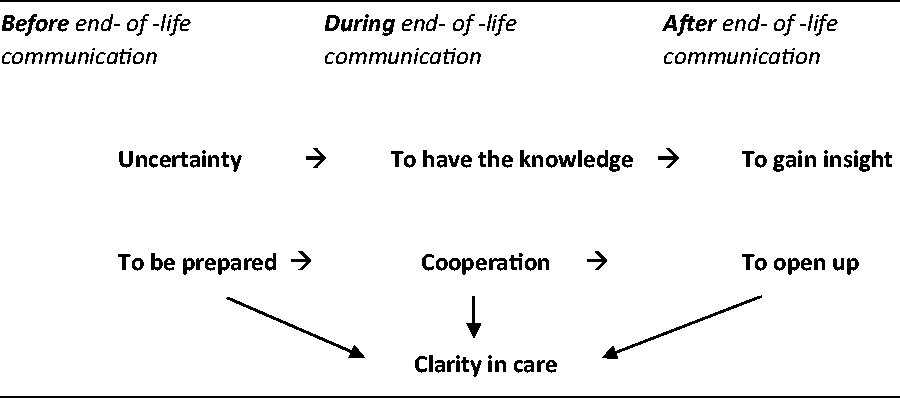
Before end-of-life communication
The domain Before end-of-life communication consisted of the two categories to be prepared and to be uncertain. They illuminate the content of the RNs’ positive and negative experiences before an end-of-life communication with the patient took place.
To be prepared
The RNs considered it very important to be well prepared before an end-of-life communication. Because of this, they tried to obtain information from the patients to get a sense of the patients’ readiness by getting to know them, thus identifying their understandings of the progress of the disease. This was especially important when the RNs felt that time was short due to a rapidly worsening patient status. In these situations, the RNs could not always prepare themselves by reading the patient records or through conversations to identify patient needs. The RNs also expressed that it was harder to communicate with the patients if they were assessed as not being on the same level of understanding. It was particularly difficult to respond to the patients’ questions when it was not apparent in the records whether the patient had received information about their disease, or how much they knew about their palliative situation.
RNs found it especially hard not to give false hopes or say too much before the physician had given information about changes in the care of the patient. To relate without saying too much … To know by the records that this is not going to be ok … One does not want to give false hope … It is this balance that is so complicated. (RN 7)
To be uncertain
Patients’ uncertainty as well as the uncertainty of the RNs made the RNs feel powerless. During conversations RNs often noticed that the patient was uncertain about their prognosis and their state of illness before the end-of-life communication. The RNs experienced a barrier in the care if the prognosis was bad and they did not know how much the patient knew. I get really stressed when I know something they don’t // and if they ask questions and I know … then it is really hard. I cannot lie but have to tell them to ask the physician about that. (RN 9)
The RNs’ ambitions were to establish a caring relationship before the end-of-life communication, aiming at creating conditions for a more open communication and patient satisfaction, with further plans for both further care and future life and death. The RNs also experienced a barrier to communication when patients focused solely on the medical issues or treatments despite a bad prognosis.
During end-of-life communication
All RNs expressed a positive attitude towards participation in end-of-life communication even if they experienced that it could be personally hard to deal with at the time. The categories shown in the domain during end-of-life communication were: to have cooperation and to have the knowledge.
Cooperation
Cooperation and interaction between physicians and RNs were described as crucial during end-of-life communication. When this worked the RNs felt relaxed and the communication became calmer and a safer mood was radiated among the people involved. Some have another way of doing it and I feel more relaxed. This not only depends on the patient but on the physician. But it also depends on how often you work together with that physician. (RN 6) You just listen during the conversation, as a nurse … it is a medical thing for the physicians … Even if I had a good relationship with the patient I did not get involved in the conversation. (RN 10)
To have the knowledge
This was seen as essential by the RNs to map out the patient’s level of understanding. This included ensuring that patients and their relatives received relevant information about the care, treatment and disease progression, and that they were able to ask questions. When the content of the end-of-life communication had a clear medical focus the patients and their relatives seemed calmer and more relaxed, probably due to the fact that they felt informed about the plans for continued care.
When the physician provided the information to the RNs, the patients, and their relatives at the same time, the nurses felt that they received more information than if they had read the information in the patient’s records. In the former case they could see the reactions of the patient and the relatives and therefore be able to be more supportive. … you receive so much information that you cannot find in written text, for example you see how patients receive the news, if it seems like they understand. (RN 5)
After end-of-life communication
Two categories were shown in the after end-of-life communication: to open up and to gain insight. These categories describe how the RNs experienced that the orientation of care changed to focus on the patient’s well-being. It then became easier for the RNs to conduct further conversations with the patient and their relatives.
To open up
After an end-of-life communication the patient processed what had been said and the RNs experienced that this stage opened up for further conversations about the patient’s situation. Both the patient and I have the courage to talk more explicitly about things that were more unclear before. The patient dared to ask about things we did not talk about earlier since none of us knew about the situation. (RN 4) One has reached over some kind of threshold when they /the patients/ get this information and one is able to support in another way. (RN 1) You know how to align the care, it becomes clearer that you don’t need to expose the patient to unnecessary medical procedures and mobilization that they cannot handle. (RN 8)
To gain insight
When the patient received the information, it became calm around the patient and the relatives, but also among the RNs. I thought that [the mood in nursing conversation] was more relaxed afterwards because she [the patient] got an answer to her questions during the end-of-life conversation. (RN 3) Then, everyone had the insight of what was going on and no one had to be on tiptoe. (RN 7) … easier to focus on relieving symptoms and not on treatment, more focused on patients’ wellbeing and no unnecessary injections and that kind of stuff … They know why we choose to refrain from things and why we choose to do other things. It is easier to explain and they gain more and more insight. (RN2)
Discussion
RNs need to be prepared before end-of-life communication to be able to meet the patient’s and their relatives’ uncertainty. The results of the current study illuminate the complexity of the RNs’ role in the palliative care of a patient in an oncological context. This is in accordance with previous findings from McLennon et al. 30 who describe nurses’ experiences of initiating conversations with patients at end of life as being ‘stuck in the middle’ between physicians, patients and their relatives, and not knowing what has already been said or understood. They also, as in the current study, highlight the importance of cooperation, having a good relationship between physicians and nurses, and having knowledge about what the other professionals have said. If this is not the case, nurses feel powerless and not able to meet the patients’ questions, wonderings or emotional reactions. Travelbee 25 reports that if the care is not structured to meet patients’ needs or the acceptance of their illness, there could be a barrier to communication. RNs in the current study also reveal that obscurity or imprecisions in patient records could be a significant barrier in their encounters and communication with patients.
The results in the current study show that whether RNs felt safe and comfortable depended on the physician’s way of acting during end-of-life communication. If the physician felt uncomfortable or insecure, the RNs needed to support the conversation. This was seen as an obstacle in the end-of-life communication by the RNs, as previously described by Schulman-Green et al. 31 Physicians’ ways of delivering information to the patient and their relatives during end-of-life communication affect how they receive and experience the bad prognosis. This is in accordance with the findings of Kirk et al. 14
The Swedish National Board of Health and Welfare 3 stresses that end-of-life communication is a communication between physicians and patients, included in a physician’s occupational duty. According to policy documents, RNs have no distinct function in end-of-life communication. However, the results of the current study showed clearly that RNs’ participation in the conversation gave better opportunities to deliver adequate and quality care. This can be understood in the light of Travelbee, 25 where communication is described as a tool nurses need to help the patient master illness and give support in stressful situations of suffering and illness. Mc Lennon et al. 30 illuminate feelings of satisfaction among nurses in the knowledge that the nurses have helped patients in difficult situations. This was also shown in the current study where RNs appreciated being able to give continued support to the patient and their relatives after end-of-life communication. 30 Effective communication at the end of life is an essential skill for nurses. The problem is that few receive formal training in this area. 32
Time and timing are important phenomena when focusing on end-of-life communication. Travelbee 25 describes difficulties when an illness is fast progressing, and it is hard for the RNs to create a relationship with the patient. This was also shown in the current study. The Swedish National Board of Health and Welfare 3 points out that end-of-life communication should be updated when the illness is in a changing phase. Still, several RNs in this study felt that end-of-life communication occurred too late in the patient’s process, which has also been shown by Kirk et al., 14 Schulman-Green et al. 31 and Ågren Bolmsjö et al. 4
Methodological issues
The considerations about validity and credibility in this study have been guided by Graneheim and Lundman27,28 as well as Elo and Kyngas 26 but also by Polit and Beck. 33 These sources claim content analysis as useful both to describe and interpret text on different levels of understanding in the caring/nursing science field. The process of analysis was guided by an open approach towards possible new understandings being revealed of the phenomena of interest. The authors also worked with a movement back and forth between the text itself and the new understanding so as not to not risk losing the possible meaning of the text. Validity is concerned with how true the results might be and a way for the reader to assess the validity is to present quotations of the interviews. 27 In this study a relatively large number of quotations were used both to show the reader validity and to give the reader a more colorful picture of the aspects of nursing that were narrated during the interviews.
According to Holloway and Biley, 34 pre-understandings are needed for the researcher to be engaged and to show experiences connected to the chosen phenomena. It gives the opportunity to ‘speak the same language’ as informants do. The interview guide was tested in a pilot interview to search for relevance according to the aim of the study. The interview guide helped the authors keep their own pre-understandings in control during the interviews. It was very important to create an interaction between the researcher and the RN during the interviews and to let the RN feel that they could narrate in the way they chose.
Conclusions and relevance to clinical practice
The purpose of this study was to describe crucial aspects of nursing within the process of end-of-life communication in an oncological context, to contribute to a wider understanding of RNs’ experiences, role and possibilities in these settings. Increased knowledge about the complexity of end-of-life communication may have the potential to improve the care of the patient. But also moving towards a model of care where openness for the orientation of the care is clear for everyone involved. End-of-life communication must be seen as a key act within oncology care, continuously taking place during the whole process of illness. The RN’s role is of significant importance in the phase before, during and after the actual end-of-life communication takes place to reduce anxiety and suffering for both patients and their relatives. An end-of-life communication that is more physician and medicine oriented, has to be supplemented by nursing-care-related aspects. This could increase patient and relative participation and experience of safety in the situation.
Footnotes
Author contributions
Study design: AR, SF, ES. Data collection: AR, SF. Analysis: AR, SF, ES, L-KG. Manuscript preparation: L-KG, AR and SF.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.