
Abstract
The aim of this population-based cross-sectional study was to describe and compare the prevalence and features of perceived loneliness among home-dwelling older adults with (n = 129) and without (n = 244) memory disorder. The latter group was randomly resampled from 789 respondents stratified by age to obtain a standardized control group. Loneliness was assessed using the six-item De Jong Gierveld Loneliness Scale, and perceived stress using Cohen, Kamarck and Mermelstein’s 10-item Perceived Stress Scale. Results show that severe loneliness was common among the home-dwelling older adults, especially those with memory disorder, who also perceived stress more frequently than those without memory disorder. Both groups, but again more frequently those with memory disorder, were more likely to be emotionally than socially lonely. Thus, when planning social and healthcare services and interventions to mitigate loneliness among older adults living at home, memory problems and emotional loneliness require particular consideration.
Background
Loneliness is generally regarded as an unpleasant negative feeling. 1 Its prevalence among older adults varies between 8% and 42% according to population surveys in Finland, Ireland, Great Britain, the Netherlands and Wales.2–9 A large cross-national study found that the prevalence of loneliness among older adults varied between 6.3% and 25.4%. 10 Loneliness has been associated with several adverse sociodemographic (e.g. higher age, low education, poor income, and living alone),2,11–14 social (e.g. death of spouse, small social network, weak community/social integration and low emotional/social togetherness),2,3,5,10,12,14,15 and functional factors, 2 as well as physical and/or mental health factors (e.g. depression, anxiety, low self-esteem and low subjective well-being).2,3,5,12,14,15 Furthermore, it is related to unmet personal needs,14,15 high healthcare utilization, 16 and mortality. 17
Prospectively, loneliness increases the risk of memory disorders,6,17,18 and perceived stress in later life. 19 Satisfying personal relationships, 10 and stable social networks 20 contribute to the overall well-being of older adults, while dissatisfaction with social environment4,21 is one of many contributors to loneliness14,22 and adversely affects human needs, expectations,4,23 and human health and survival. 24 Thus, the degree to which the social environment provides support and contacts with family members and friends, may play a major role in subjective well-being5,21 and perceived community satisfaction of home-dwelling older adults. 21
Frequent emotional support (especially from the nearest or very trusted people)25,26 could enhance older adults’ cognitive performance, reduce feelings of loneliness, 8 and/or contribute to their mental well-being. 21 Moreover, numbers of visits and contact maintenance are positively associated with perceptions of being cared for,21,22 while needing help and lack of social activities are negatively associated with survival. 27 Further, sharing experiences with peers with the same illness or religious faith is associated with well-being. 21 A positive association between socioeconomic status and provision of social support (i.e. help or assistance from family/friends/organizations) has also been reported. 26
Physical environments that enable safe activities in a supportive community may contribute to the subjective feeling of well-being and quality of life experienced by older adults.21,28 Beneficial features of such environments may include provisions of opportunities for social outdoor activities,21,28,29 and events to attend without verbal demands. 29 In addition, hobbies and activities may help older adults to cope with living alone after loss of a spouse 21 and reduce feelings of loneliness among those with memory disorder. 22 Moreover, health-promotive group-based interventions with an educational input or supportive activities may improve subjective feelings of well-being among older adults with and without memory disorder.30–33 Such activities can also prevent or alleviate their feelings of loneliness.30,32,33 Social environment here refers to a wide and subjectively experienced physical and social milieu, including interactions between people and their environment, as well as social support. Unmet personal expectations and needs relating to the social environment as an essential part of humans’ culture and history,21,34 may pose severe risks for the development of feelings of loneliness. 24 In this study, the term ‘memory disorder’ refers to a progressive neurodegenerative condition (Alzheimer’s disease, vascular dementia and other types of dementia).35,36
In summary, various factors associated with loneliness amongst older adults with and without memory disorder have been identified. However, additional information is required to facilitate the development of effective strategies to minimize their loneliness and associated adverse effects, particularly for those living at home. Therefore, the objective of the study presented here was to describe and compare the prevalence and features of perceived loneliness among home-dwelling older adults with and without memory disorder. We addressed two specific research questions: How do home-dwelling older adults with memory disorder perceive loneliness, and does a sense of loneliness differ among older adults with and without memory disorder?
Methods
Setting and study participants
The presented study was a part of the population-based Gamified Services for Older People project (GASEL), a multidisciplinary collaborative project to identify effective approaches to prevent older adults’ marginalization and promote their well-being. It is based on responses to a questionnaire survey conducted in the GASEL project. 37 After piloting with 11 volunteering seniors, the questionnaire was sent by post in November 2014 to a random sample of 1500 people living in the city of Oulu, Finland, drawn from the population register of Finland. The subjects were all aged 65–114 years at the end of 2014, spoke Finnish as their native language and were permanently residing in Oulu. If necessary, a reminder was sent out four weeks later. In total, 918 (61.2%) respondents had returned their questionnaire by a cut-off date in January 2015.
Of the 918 respondents 129 were home-dwelling older adults with a self-reported diagnosed memory disorder, 103 suffered from early-stage and 26 from middle-stage memory disorder. Of the 129 respondents with memory disorder, 18, 21, 25 and 65 were 65−70, 71−75, 76−79 and ≥80 years old, respectively. An age-standardized comparison group was formed from the others, who did not (self-reportedly) have memory disorder, by stratifying them into the same age categories. All those aged ≥80 years were retained, while the others were randomly sampled to include 1.89 times as many subjects in each age category as in the group of older adults with memory disorder. This resulted in sample sizes of 34 (from 370), 40 (from 199) and 47 (from 97) respondents of older adults without memory disorder in the 65−70, 71−75 and 76−79 years-old classes, plus 123 in the ≥80 years-old class. In total, the age-adjusted comparison group included 244 home-dwelling older adults. Mean ages of the older adults with and without memory disorder age groups were 78.87 (SD = 7.09) and 78.41 (SD = 6.55) years, respectively, with similar variances.
Ethical considerations
The study protocol was approved by the Ethics Committee of Human Sciences of the University of Oulu (statement 6/2014). A personal letter including the questionnaire described the voluntary nature of participation, the confidentiality of the data and the presentation of results. A completed questionnaire was regarded as informed consent to participate.
Questionnaire
The questionnaire included items related to the participants’ backgrounds, perceived loneliness, stress, health and social participation. The six-item De Jong Gierveld Loneliness Scale was used to measure perceived loneliness38,39 and the Perceived Stress Scale to measure perceived psychological stress.40,41 These scales are briefly described in the following sections.
The De Jong Gierveld Loneliness Scale
Loneliness among older adults with and without memory disorder. Means, frequencies and percentages.
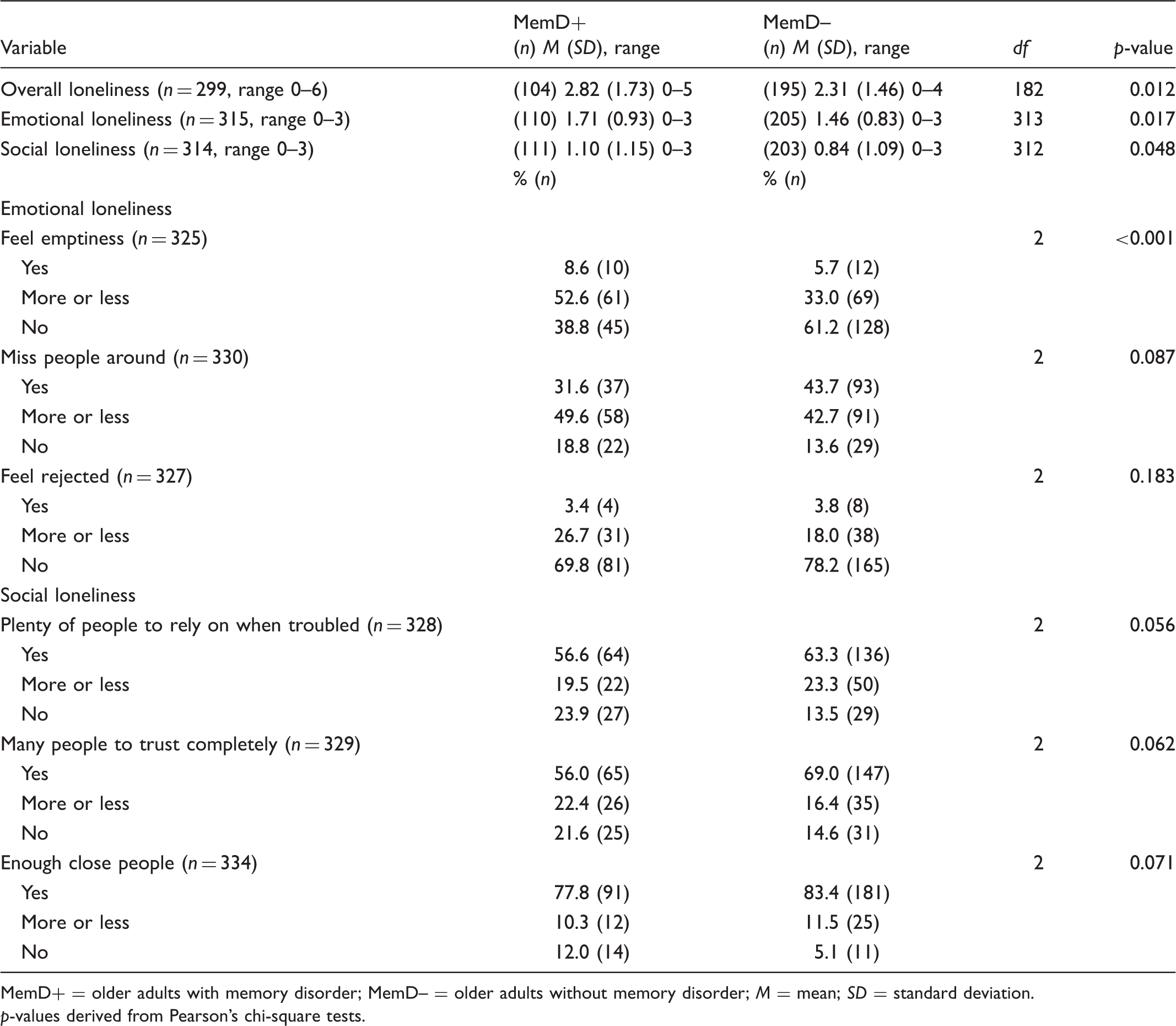
MemD+ = older adults with memory disorder; MemD– = older adults without memory disorder; M = mean; SD = standard deviation.
p-values derived from Pearson’s chi-square tests.
In score calculation, each item is rated on a five-point Likert scale ranging from definitely yes (1) to definitely no (5). The five response alternatives were collapsed to form dichotomized scores, roughly indicating the presence (1 point) or absence (0 points) of constant loneliness. Thus, the total scores range from 0 to 6, and the emotional and social subscale scores range from 0 to 3, higher scores indicating greater loneliness. 38 Moreover (departing from the guidelines), 39 for further categorization of overall loneliness, scores of 0−2, 3−4, 5 and 6 were classified as not lonely, moderately lonely, severely lonely, and very severely lonely, respectively, while emotional and social loneliness scores of 0, 1, 2 and 3 were classified as not lonely, moderately lonely, severely lonely, and very severely lonely, respectively. In contrast, to assess item-level loneliness, the five response alternatives were collapsed into three Likert categories: 1) definitely yes or yes, 2) more or less, and 3) no or definitely no.
Perceived Stress Scale (PSS)
Perceived stress among older adults with and without memory disorder.
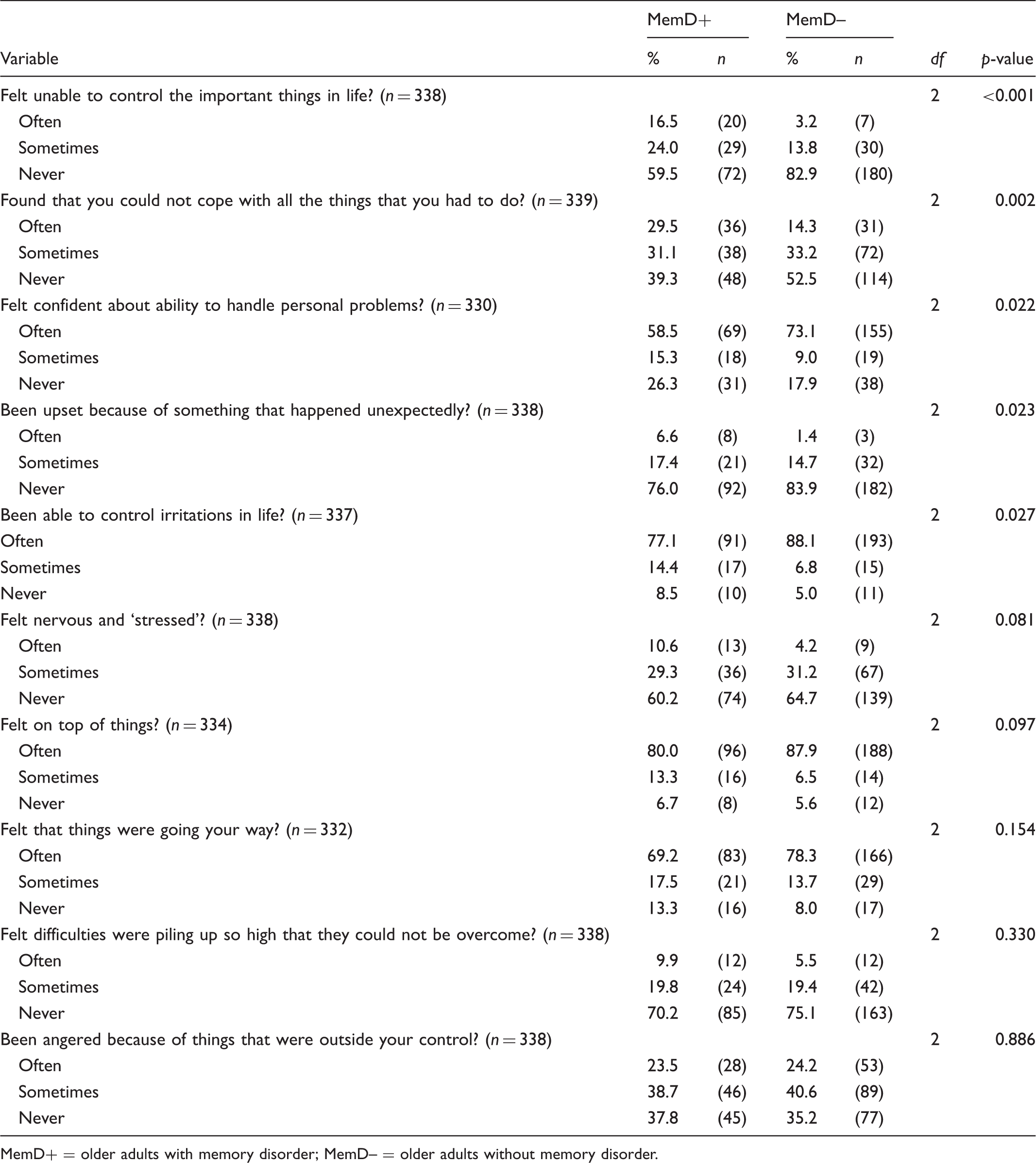
MemD+ = older adults with memory disorder; MemD– = older adults without memory disorder.
Statistical analysis
To analyze the statistical significance of differences between the respondents with and without memory disorder, cross-tabulation was used for categorical variables and independent samples t-tests for continuous variables. To assess the significance of associations and correlations between Perceived Stress Scores and loneliness scores, the Pearson chi-square test and Pearson correlation coefficient were used. For all statistical analyses, SPSS, version 23.0 (IBM Corp., Armonk, NY) was used, and differences between the groups were deemed significant if p < 0.05.
Results
Background information on the study participants.
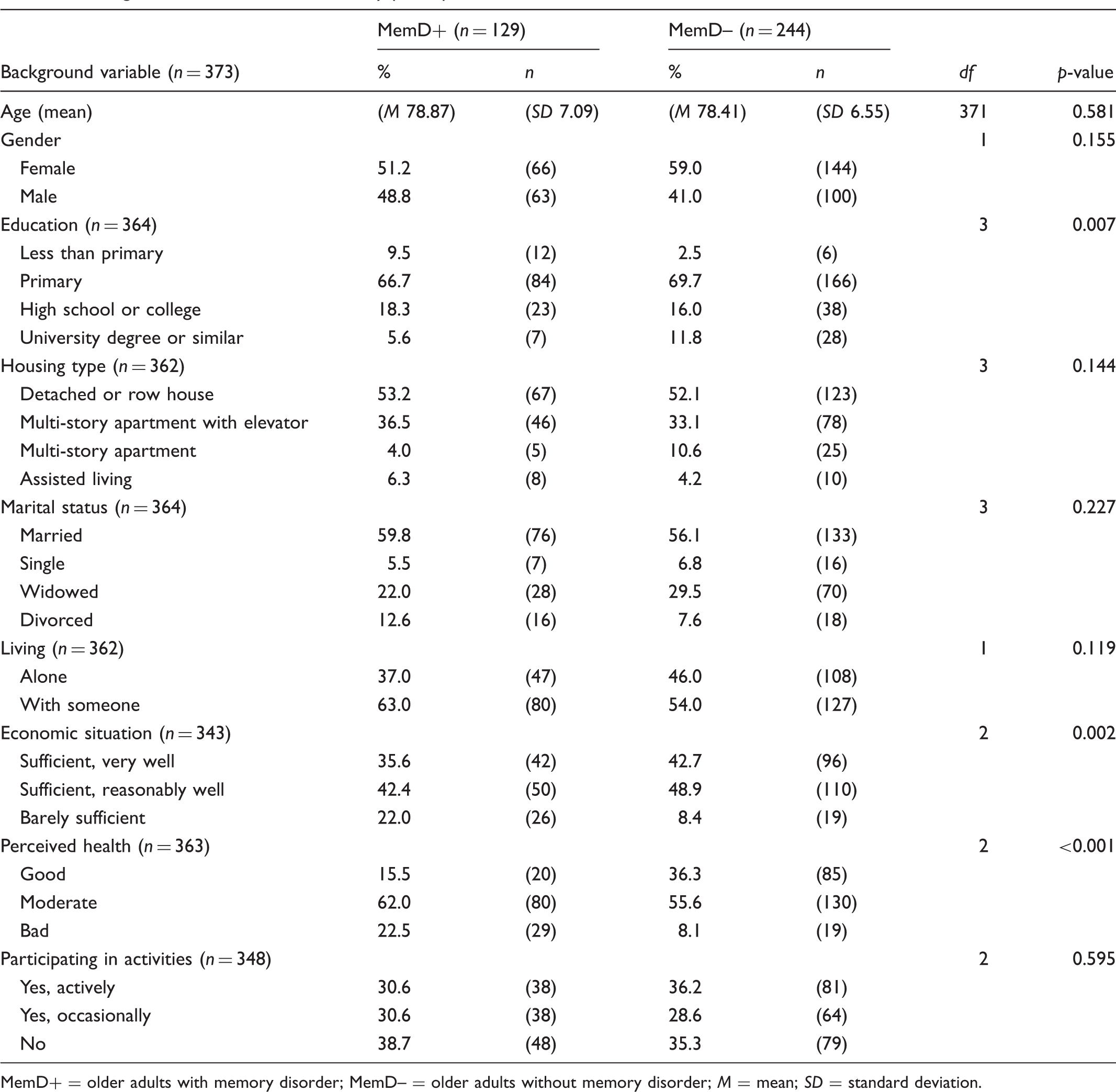
MemD+ = older adults with memory disorder; MemD– = older adults without memory disorder; M = mean; SD = standard deviation.
Overall, emotional and social loneliness
Mean overall, emotional and social loneliness scores were significantly higher among older adults with memory disorder compared to those without memory disorder (Table 1). Moreover, in analyses with categorical variables 22.1% (n = 23/104) of respondents with memory disorder felt severely or very severely lonely, while the proportion was 9.8% (n = 19/195) for respondents without memory disorder (df = 3, p = 0.013). The proportion of participants reporting very severe emotional loneliness was also higher among those with memory disorder than among their peers without it (21.8% vs. 12.7%, respectively; df = 3, p = 0.009).
The item-level analyses of emotional and social loneliness indicated that higher proportions of older adults with than without memory disorder felt emptiness (df = 2, p < 0.001), but detected no other significant differences (Table 1). A substantial proportion (43.7%) of older adults without memory disorder reported missing people around (emotional loneliness), but the majority (83.4%) had enough close people (social loneliness). For respondents with memory disorder, these figures tended to be somewhat lower (i.e. 31.6% vs. 77.8%). In general, social loneliness tended to be more common in older adults with memory disorder than in those without memory disorder, but there was no significant difference between groups in this respect. More than a fifth of the older adults with memory disorder reported not having plenty of people to rely on in case of problems, and not having many people they could completely trust.
Perceived stress
Means and percentages of Perceived Stress Scores among older adults with and without memory disorder.
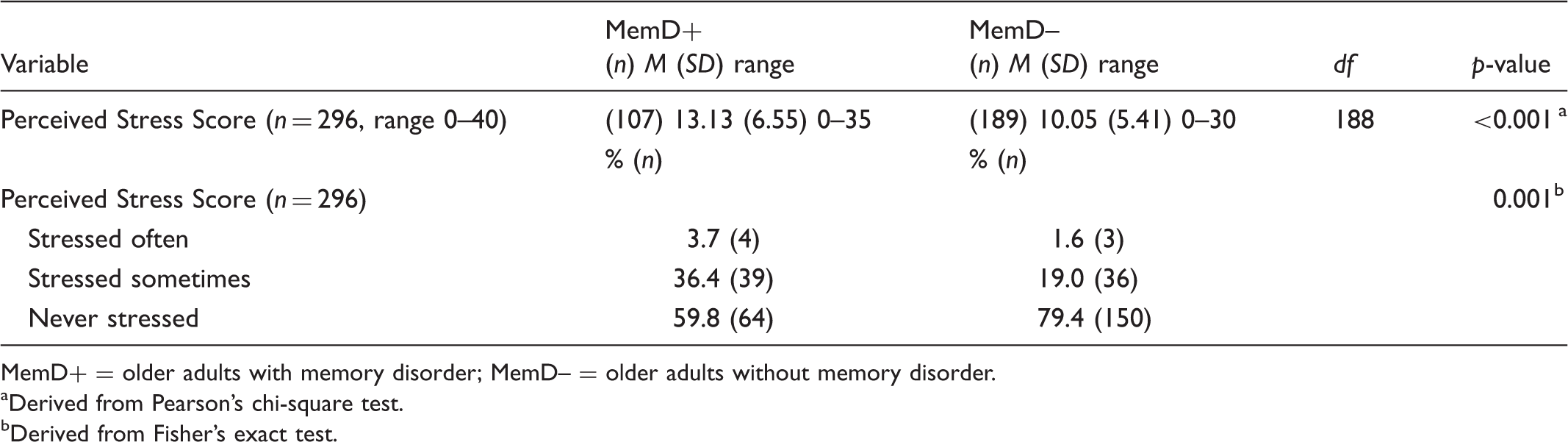
MemD+ = older adults with memory disorder; MemD– = older adults without memory disorder.
Derived from Pearson’s chi-square test.
Derived from Fisher’s exact test.
Discussion
Home-dwelling older adults in this population-based survey were found to suffer more from loneliness if they had memory disorder than if they (self-reportedly) had no such disorder. More than a fifth of participating older adults with memory disorder reported feeling severely or very severely lonely, supporting previous findings on prevalence of loneliness among older adults.2–9 Emotional loneliness, especially feeling emptiness, was more frequent among those with memory disorder, who also perceived higher stress than their peers without memory disorder.
A previous English survey using the 11-item De Jong Gierveld Loneliness scale reported low levels of emotional and social loneliness among older adults (mean scores below their respective scale mid-points). 14 In our study (using the shorter six-item version of the scale), the mean overall and social loneliness scores for both older adults with and without memory disorder were also below their respective scale mid-points, but not the emotional loneliness scores for respondents with memory disorder. The mean emotional loneliness scores we obtained were higher than those reported for older adults in every country included in a previous cross-national study except Georgia. 42 In partial accordance with findings that cognitive impairment increases feelings of loneliness among older adults in Wales, 9 we found that home-dwelling older adults with memory disorder experienced higher levels of overall, emotional, and social loneliness than home-dwelling peers without memory disorder. However, a Swedish study found that higher proportions of older adults with memory disorder compared to those without felt socially, but not emotionally, lonely. 11 These variations in reported prevalence may be at least partly due to cultural differences 10 or differences in selected indicators of loneliness. Despite its universal character, loneliness is a subjective feeling, 13 which can be affected by numerous factors that impair (or improve) the quality of life, 4 such as death (or improved health) of spouse or significant other, illness of oneself or significant others, or moving either to another area or to another house in the same area. 12
Despite the known positive correlation between loneliness and stress, 19 our mean scores for perceived stress were below the mid-point, indicating generally low levels of stress among our participants. However, those with memory disorder generally perceived higher stress than those without. Mean PSS scores of older adults in a previous analysis of data obtained in three national surveys in the USA ranged from 10.80 to 11.98 points. 44 We obtained slightly lower scores for older adults without memory disorder and slightly higher scores for those with memory disorder. We also found a four-fold higher frequency of high stress (PSS score ≥20) among older adults with memory disorder (16%) than among those without (4.3%). This may be partly due to awareness of changes in daily activities and social interactions during early stages of memory disorder heightening stress29,45 or loss of others. 22 Forgetfulness can lead to burdensome and stressful situations, accompanied by confusing and unpleasant experiences, for older adults with memory disorder.22,45 Previous studies have shown that poor mental health is associated with loneliness.3,4,15 However, another study found that stress scores increase with age among the Swedish dementia-free population, mean scores being highest for those aged ≥81 years. 46 Thus, it is important to evaluate whether feelings of loneliness among older adults might be due to a depressive mood state rather than a lack of social contacts. 3
Among the randomized population-based sample of older adults we surveyed, emotional loneliness appeared to be more prevalent than social loneliness, and more prevalent among older adults with memory disorder than without. These findings corroborate both previous suggestions that older adults may benefit from frequent emotional support, 8 and reports that emotional and social support from family members, 21 including psychological and material resources, can improve older adults’ ability to cope with stressful situations. 47 Also, positive experiences of a warm and safe formative environment can provide at least some protection against loneliness in older age 12 and help people to cope with challenges and changes in life. Thus, important challenges for our social and healthcare systems and for healthcare personnel are to develop and implement effective means to offer frequent support and prevent emotional and social loneliness of older adults.
It should be noted that this study has several limitations. First, our findings are restricted to a single cross-sectional analysis of responses of a sample drawn from a population in one Finnish city. Our results provide no indications of causation, and any generalizations or comparisons should be cautious. Another limitation concerns the ability of older adults with memory disorder to complete questionnaires, which may decline due to illnesses.11,48 Most of the home-dwelling older adults with memory disorder who participated in our study were in the early stages of their illnesses. However, the capability to complete the questionnaire either alone or with assistance decreases with advancing stages of illnesses,11,48 potentially sharply even in early moderate stages. 48 Moreover, according to published guidelines, the six-item De Jong Gierveld Loneliness Scale may not be sufficient for detailing the prevalence of loneliness. 39 Nevertheless, although we used this scale, since we classified all scores of 0−2 as not lonely, our results seem more likely to have underestimated than overestimated the respondents’ loneliness.
Conclusion
Severe loneliness is common among home-dwelling older adults. Feelings of loneliness, perceived emptiness and stress are common, especially among those with memory disorder. Older adults with memory disorder, particularly, seem to be more prone to emotional than social loneliness. As loneliness is an important risk factor for poor health, low sense of subjective well-being and premature institutionalization, the identification of social, psychosocial and psychological needs of home-dwelling older adults with memory disorder should be improved to address their perceived loneliness. Our study suggests that nurses and other healthcare professionals should distinguish between emotional and social loneliness in clinical fieldwork to enable the implementation of appropriate protective actions. It is known that evidence-based educational group interventions can potentially reduce feelings of loneliness among home-dwelling older adults, especially those with memory disorder, and help to maintain their cognitive functioning for as long as possible.
Moreover, appropriate technology can potentially improve the sense of safety among home-dwelling older adults with memory disorder. In addition, their social and psychosocial needs can partly be fulfilled through voluntary organizations offering help and support, for example age-appropriate activities and visitor services. However, more research is needed to characterize social, psychological, physical environment and health factors, and identify potential effective interventions, including various forms of emotional and social support. Furthermore, longitudinal studies could provide knowledge of causal relations between risk factors and loneliness, as well as of effects of social environmental factors on loneliness among older adults in their home environment.
Footnotes
Funding
This study was performed as part of the GASEL project, supported by the Finnish Funding Agency for Innovation [Grant No. 40270/13], and the Sense of Security at Home (TuTunKo) research project, supported by Tekes – the Finnish Funding Agency for Innovation [Grant No. 2864/31/2015].
Conflict of interest
The authors declare that there is no conflict of interest.